
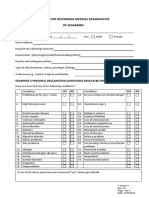
Ks 0497 Medical Examination Eng PDF
Ks 0497 Medical Examination Eng PDF
You might also like
- MPA-ANNEX B-C - Seafarer Medical Fitness and CertificateDocument6 pagesMPA-ANNEX B-C - Seafarer Medical Fitness and CertificateFred ChowNo ratings yet
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- MoH Adverse Events Policy PDFDocument33 pagesMoH Adverse Events Policy PDFnayan4uNo ratings yet
- MLC Medical FormDocument5 pagesMLC Medical FormSoekhaidir SuripnoNo ratings yet
- Hearing Meets The Section A-L/9?: PractitionerDocument13 pagesHearing Meets The Section A-L/9?: PractitionerRian Daud SadewaNo ratings yet
- Nursing Care Plan For Diabetes Mellitus Type 2 (Kenneth Regida)Document3 pagesNursing Care Plan For Diabetes Mellitus Type 2 (Kenneth Regida)Kenneth Anthony Tiu Regida100% (8)
- 5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeDocument5 pages5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeinstalasiNo ratings yet
- Medical Examination Form SeafarersDocument5 pagesMedical Examination Form SeafarersHazem ElbananNo ratings yet
- F7.6 Seafarers Medical Examination-CertificateDocument7 pagesF7.6 Seafarers Medical Examination-CertificateHerbert Maganga100% (1)
- Mpa SC052020 - Mpa Medical FormDocument6 pagesMpa SC052020 - Mpa Medical FormFred ChowNo ratings yet
- CA 67-02 (A)Document4 pagesCA 67-02 (A)Cameron BaxterNo ratings yet
- Form Malta Medical Cek UpDocument6 pagesForm Malta Medical Cek UpannuryogNo ratings yet
- Singapore Mpa Medical Oct 2013Document5 pagesSingapore Mpa Medical Oct 2013Nebojsa MijovicNo ratings yet
- C105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by AstroDocument5 pagesC105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by Astroklinik utama Bali Puri MedikaNo ratings yet
- Medical Certificate For Service at Sea: ConfidentialDocument4 pagesMedical Certificate For Service at Sea: ConfidentialADMIN MCU RSU SAHID SAHIRMAN100% (1)
- MEMO No 50 Revised Traveller Health DeclarationDocument1 pageMEMO No 50 Revised Traveller Health DeclarationMustafa EnghinNo ratings yet
- Registration Forms FoundationDocument3 pagesRegistration Forms FoundationArif ZaulkifleeNo ratings yet
- Health Declaration Form - AMSB PDFDocument4 pagesHealth Declaration Form - AMSB PDFKhairul RazaliNo ratings yet
- Biennial National Medical ReportDocument5 pagesBiennial National Medical ReportXimena FariasNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AClick TechnologyNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AHector ValleNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- The Ship Captain's Medical GuideDocument232 pagesThe Ship Captain's Medical GuideOnur çakıl100% (2)
- Format For Recording Medical Examinatios of SeafarersDocument4 pagesFormat For Recording Medical Examinatios of SeafarersАлексNo ratings yet
- Consent For Minor Dental PDFDocument2 pagesConsent For Minor Dental PDFJanNo ratings yet
- COVID-19 Vax Consent FormDocument3 pagesCOVID-19 Vax Consent FormCj CCNo ratings yet
- Bahamas Medical FormDocument9 pagesBahamas Medical FormКсения ЧучковаNo ratings yet
- I. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormDocument9 pagesI. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormAlex BensonNo ratings yet
- ME In-G Ie: Claim FormDocument4 pagesME In-G Ie: Claim FormnithiananthiNo ratings yet
- Ahmedabad Claim FormDocument5 pagesAhmedabad Claim FormFirdaus PanthakyNo ratings yet
- Form 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedDocument2 pagesForm 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedRaju.PalNo ratings yet
- Wrist Conditions Disability Benefits QuestionnaireDocument8 pagesWrist Conditions Disability Benefits QuestionnaireCombat CraigNo ratings yet
- Medical FormDocument9 pagesMedical Formaosei8185No ratings yet
- Initial Sheet Medical Case Sheet AuditDocument2 pagesInitial Sheet Medical Case Sheet AuditSrinivas Polikepati0% (1)
- Annex 7 Medical Examination FormDocument3 pagesAnnex 7 Medical Examination FormBaoPhucNo ratings yet
- Med. Report 1 (2ND ENG)Document1 pageMed. Report 1 (2ND ENG)mostafawageeh8No ratings yet
- VBA 21 0960M 12 ARE Shoulder and ArmDocument9 pagesVBA 21 0960M 12 ARE Shoulder and ArmCombat CraigNo ratings yet
- Singapore Dental Claim Form Interactive M003 60E 010115Document5 pagesSingapore Dental Claim Form Interactive M003 60E 010115Nazim SalehNo ratings yet
- Pre AdmissionDocument5 pagesPre AdmissionLaura Margaretha BatlayarNo ratings yet
- ADR AEFI Reporting FormDocument1 pageADR AEFI Reporting Formgulafsha1No ratings yet
- Medical Certificate PDFDocument1 pageMedical Certificate PDFFAIQNo ratings yet
- Medical Examination Form MLC 2013Document7 pagesMedical Examination Form MLC 2013danadimache100% (4)
- VBA-21-0960M-2-ARE Ankle PDFDocument9 pagesVBA-21-0960M-2-ARE Ankle PDFCombat CraigNo ratings yet
- VBA 21 0960M 9 ARE Knee and Lower LegDocument10 pagesVBA 21 0960M 9 ARE Knee and Lower LegCombat CraigNo ratings yet
- MEDICAL SHEET 2022 SecondaryDocument2 pagesMEDICAL SHEET 2022 SecondaryScribdTranslationsNo ratings yet
- Appendix 1: Health Declaration FormDocument3 pagesAppendix 1: Health Declaration Formmujahid_mcclellandNo ratings yet
- Appendix 1: Health Declaration FormDocument3 pagesAppendix 1: Health Declaration FormMohd ShahrirNo ratings yet
- Covid19vaccineconsentform UpdatedDocument2 pagesCovid19vaccineconsentform UpdatedGlenn ReinhardtNo ratings yet
- Attachment A of Medical RequirementDocument8 pagesAttachment A of Medical Requirementyoutuber AbheeNo ratings yet
- Pre Employement Medical Fitness Policy PDFDocument5 pagesPre Employement Medical Fitness Policy PDFShubham SharmaNo ratings yet
- RCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Document2 pagesRCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Ahmad ShodiqNo ratings yet
- Annexure 2,3 and 4 DraftDocument4 pagesAnnexure 2,3 and 4 DraftKashiramNo ratings yet
- טפסים לביטוח רפואיDocument3 pagesטפסים לביטוח רפואיmaricelangob3No ratings yet
- Annex C3 Medical Examination Form For All CoursesDocument2 pagesAnnex C3 Medical Examination Form For All CoursesveasnaNo ratings yet
- Medicare Insurance Claim Form: PolicyholderDocument2 pagesMedicare Insurance Claim Form: PolicyholdertagashiiNo ratings yet
- Surgical Safety ChecklistDocument1 pageSurgical Safety ChecklistАндрій ДанильцівNo ratings yet
- Medical Claim - Doctor'S Statement: Patient's Personal DetailsDocument3 pagesMedical Claim - Doctor'S Statement: Patient's Personal DetailsWeng Meng VISTANo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- New Frontiers of Genetics and The Risk of EugenicsDocument132 pagesNew Frontiers of Genetics and The Risk of EugenicsOscar Sanchez CarreñoNo ratings yet
- Medical College Choices 08 NovDocument1 pageMedical College Choices 08 NovamitNo ratings yet
- Janitorial ProductivityDocument7 pagesJanitorial ProductivityThe Cleaning LibraryNo ratings yet
- Test Bank For Pharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 3rd Edition WatkinsDocument6 pagesTest Bank For Pharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 3rd Edition WatkinsJean Taylor100% (46)
- Crisis and Nursing InterventionDocument44 pagesCrisis and Nursing InterventionArchana100% (4)
- Definition and Aim of EpidemiologyDocument25 pagesDefinition and Aim of EpidemiologyJeevan KumarNo ratings yet
- Suicide in Utah 2020Document6 pagesSuicide in Utah 2020McKenzie StaufferNo ratings yet
- Pedia ReviewDocument22 pagesPedia ReviewDebbie LanceroNo ratings yet
- 2012 Resistant HypertensionDocument9 pages2012 Resistant HypertensionBarry Tumpal Wouter NapitupuluNo ratings yet
- Clinical Ophthalmology: Instructions For CandidatesDocument16 pagesClinical Ophthalmology: Instructions For CandidatesdrlawrencekindoNo ratings yet
- 01 Manajemen Risiko Klinik (MRK)Document32 pages01 Manajemen Risiko Klinik (MRK)irmaNo ratings yet
- Nursing Clients With Hematologic DisordersDocument4 pagesNursing Clients With Hematologic DisordersLuna MarieNo ratings yet
- Hidden Pain: Ehlers-Danlos SyndromeDocument28 pagesHidden Pain: Ehlers-Danlos SyndromeVictoria67% (3)
- Home EconomicsDocument5 pagesHome EconomicsNicole Kathleen Caranto100% (1)
- Theatre Practice StandardsDocument54 pagesTheatre Practice StandardsNugroho WibisonoNo ratings yet
- Part Iv - Level 3 Hospital: Attachment 3.A - PersonnelDocument18 pagesPart Iv - Level 3 Hospital: Attachment 3.A - PersonnelIAN LAPINGNo ratings yet
- Complex Regional Pain SyndromeDocument24 pagesComplex Regional Pain SyndromeJanine RustNo ratings yet
- Nanotechnology For Biomedical ApplicationsDocument15 pagesNanotechnology For Biomedical ApplicationsVanitha AlagarsamyNo ratings yet
- MCN Drill 1Document23 pagesMCN Drill 1Cai Velasco DecenaNo ratings yet
- Book - OT Manager - Chap 57 Organizational EthicsDocument9 pagesBook - OT Manager - Chap 57 Organizational EthicsWhitney JosephNo ratings yet
- Health Benefits of Barley PDFDocument4 pagesHealth Benefits of Barley PDFYusrinaNoorAzizahNo ratings yet
- Adriene Vialpando: ExperienceDocument3 pagesAdriene Vialpando: ExperienceKritika NigamNo ratings yet
- Intussuseption and Hirschprung's DiseaseDocument5 pagesIntussuseption and Hirschprung's DiseaseAris Magallanes100% (2)
- Prevalence of Rifampicin Resistance Tuberculosis and Associated Factors Among Presumptive TB or MDRDocument3 pagesPrevalence of Rifampicin Resistance Tuberculosis and Associated Factors Among Presumptive TB or MDRTigray OutlookNo ratings yet
- TeleHealth Lecture NotesDocument40 pagesTeleHealth Lecture NotesKarthik100% (3)
- O Conceito de Saúde e A Diferença Entre Promoção e PrevençãoDocument9 pagesO Conceito de Saúde e A Diferença Entre Promoção e PrevençãoBreno CostaNo ratings yet
- 121 CD 2012Document36 pages121 CD 2012Bounna PhoumalavongNo ratings yet
- Tripping Over The Truth: How The Metabolic Theory of Cancer Is Overturning One of Medicine's Most Entrenched Paradigms - Travis ChristoffersonDocument5 pagesTripping Over The Truth: How The Metabolic Theory of Cancer Is Overturning One of Medicine's Most Entrenched Paradigms - Travis Christoffersonwehyryji0% (1)
























































































Download as pdf or txt
You might also like
- MPA-ANNEX B-C - Seafarer Medical Fitness and CertificateDocument6 pagesMPA-ANNEX B-C - Seafarer Medical Fitness and CertificateFred ChowNo ratings yet
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- MoH Adverse Events Policy PDFDocument33 pagesMoH Adverse Events Policy PDFnayan4uNo ratings yet
- MLC Medical FormDocument5 pagesMLC Medical FormSoekhaidir SuripnoNo ratings yet
- Hearing Meets The Section A-L/9?: PractitionerDocument13 pagesHearing Meets The Section A-L/9?: PractitionerRian Daud SadewaNo ratings yet
- Nursing Care Plan For Diabetes Mellitus Type 2 (Kenneth Regida)Document3 pagesNursing Care Plan For Diabetes Mellitus Type 2 (Kenneth Regida)Kenneth Anthony Tiu Regida100% (8)
- 5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeDocument5 pages5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeinstalasiNo ratings yet
- Medical Examination Form SeafarersDocument5 pagesMedical Examination Form SeafarersHazem ElbananNo ratings yet
- F7.6 Seafarers Medical Examination-CertificateDocument7 pagesF7.6 Seafarers Medical Examination-CertificateHerbert Maganga100% (1)
- Mpa SC052020 - Mpa Medical FormDocument6 pagesMpa SC052020 - Mpa Medical FormFred ChowNo ratings yet
- CA 67-02 (A)Document4 pagesCA 67-02 (A)Cameron BaxterNo ratings yet
- Form Malta Medical Cek UpDocument6 pagesForm Malta Medical Cek UpannuryogNo ratings yet
- Singapore Mpa Medical Oct 2013Document5 pagesSingapore Mpa Medical Oct 2013Nebojsa MijovicNo ratings yet
- C105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by AstroDocument5 pagesC105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by Astroklinik utama Bali Puri MedikaNo ratings yet
- Medical Certificate For Service at Sea: ConfidentialDocument4 pagesMedical Certificate For Service at Sea: ConfidentialADMIN MCU RSU SAHID SAHIRMAN100% (1)
- MEMO No 50 Revised Traveller Health DeclarationDocument1 pageMEMO No 50 Revised Traveller Health DeclarationMustafa EnghinNo ratings yet
- Registration Forms FoundationDocument3 pagesRegistration Forms FoundationArif ZaulkifleeNo ratings yet
- Health Declaration Form - AMSB PDFDocument4 pagesHealth Declaration Form - AMSB PDFKhairul RazaliNo ratings yet
- Biennial National Medical ReportDocument5 pagesBiennial National Medical ReportXimena FariasNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AClick TechnologyNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AHector ValleNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- The Ship Captain's Medical GuideDocument232 pagesThe Ship Captain's Medical GuideOnur çakıl100% (2)
- Format For Recording Medical Examinatios of SeafarersDocument4 pagesFormat For Recording Medical Examinatios of SeafarersАлексNo ratings yet
- Consent For Minor Dental PDFDocument2 pagesConsent For Minor Dental PDFJanNo ratings yet
- COVID-19 Vax Consent FormDocument3 pagesCOVID-19 Vax Consent FormCj CCNo ratings yet
- Bahamas Medical FormDocument9 pagesBahamas Medical FormКсения ЧучковаNo ratings yet
- I. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormDocument9 pagesI. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormAlex BensonNo ratings yet
- ME In-G Ie: Claim FormDocument4 pagesME In-G Ie: Claim FormnithiananthiNo ratings yet
- Ahmedabad Claim FormDocument5 pagesAhmedabad Claim FormFirdaus PanthakyNo ratings yet
- Form 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedDocument2 pagesForm 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedRaju.PalNo ratings yet
- Wrist Conditions Disability Benefits QuestionnaireDocument8 pagesWrist Conditions Disability Benefits QuestionnaireCombat CraigNo ratings yet
- Medical FormDocument9 pagesMedical Formaosei8185No ratings yet
- Initial Sheet Medical Case Sheet AuditDocument2 pagesInitial Sheet Medical Case Sheet AuditSrinivas Polikepati0% (1)
- Annex 7 Medical Examination FormDocument3 pagesAnnex 7 Medical Examination FormBaoPhucNo ratings yet
- Med. Report 1 (2ND ENG)Document1 pageMed. Report 1 (2ND ENG)mostafawageeh8No ratings yet
- VBA 21 0960M 12 ARE Shoulder and ArmDocument9 pagesVBA 21 0960M 12 ARE Shoulder and ArmCombat CraigNo ratings yet
- Singapore Dental Claim Form Interactive M003 60E 010115Document5 pagesSingapore Dental Claim Form Interactive M003 60E 010115Nazim SalehNo ratings yet
- Pre AdmissionDocument5 pagesPre AdmissionLaura Margaretha BatlayarNo ratings yet
- ADR AEFI Reporting FormDocument1 pageADR AEFI Reporting Formgulafsha1No ratings yet
- Medical Certificate PDFDocument1 pageMedical Certificate PDFFAIQNo ratings yet
- Medical Examination Form MLC 2013Document7 pagesMedical Examination Form MLC 2013danadimache100% (4)
- VBA-21-0960M-2-ARE Ankle PDFDocument9 pagesVBA-21-0960M-2-ARE Ankle PDFCombat CraigNo ratings yet
- VBA 21 0960M 9 ARE Knee and Lower LegDocument10 pagesVBA 21 0960M 9 ARE Knee and Lower LegCombat CraigNo ratings yet
- MEDICAL SHEET 2022 SecondaryDocument2 pagesMEDICAL SHEET 2022 SecondaryScribdTranslationsNo ratings yet
- Appendix 1: Health Declaration FormDocument3 pagesAppendix 1: Health Declaration Formmujahid_mcclellandNo ratings yet
- Appendix 1: Health Declaration FormDocument3 pagesAppendix 1: Health Declaration FormMohd ShahrirNo ratings yet
- Covid19vaccineconsentform UpdatedDocument2 pagesCovid19vaccineconsentform UpdatedGlenn ReinhardtNo ratings yet
- Attachment A of Medical RequirementDocument8 pagesAttachment A of Medical Requirementyoutuber AbheeNo ratings yet
- Pre Employement Medical Fitness Policy PDFDocument5 pagesPre Employement Medical Fitness Policy PDFShubham SharmaNo ratings yet
- RCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Document2 pagesRCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Ahmad ShodiqNo ratings yet
- Annexure 2,3 and 4 DraftDocument4 pagesAnnexure 2,3 and 4 DraftKashiramNo ratings yet
- טפסים לביטוח רפואיDocument3 pagesטפסים לביטוח רפואיmaricelangob3No ratings yet
- Annex C3 Medical Examination Form For All CoursesDocument2 pagesAnnex C3 Medical Examination Form For All CoursesveasnaNo ratings yet
- Medicare Insurance Claim Form: PolicyholderDocument2 pagesMedicare Insurance Claim Form: PolicyholdertagashiiNo ratings yet
- Surgical Safety ChecklistDocument1 pageSurgical Safety ChecklistАндрій ДанильцівNo ratings yet
- Medical Claim - Doctor'S Statement: Patient's Personal DetailsDocument3 pagesMedical Claim - Doctor'S Statement: Patient's Personal DetailsWeng Meng VISTANo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- New Frontiers of Genetics and The Risk of EugenicsDocument132 pagesNew Frontiers of Genetics and The Risk of EugenicsOscar Sanchez CarreñoNo ratings yet
- Medical College Choices 08 NovDocument1 pageMedical College Choices 08 NovamitNo ratings yet
- Janitorial ProductivityDocument7 pagesJanitorial ProductivityThe Cleaning LibraryNo ratings yet
- Test Bank For Pharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 3rd Edition WatkinsDocument6 pagesTest Bank For Pharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 3rd Edition WatkinsJean Taylor100% (46)
- Crisis and Nursing InterventionDocument44 pagesCrisis and Nursing InterventionArchana100% (4)
- Definition and Aim of EpidemiologyDocument25 pagesDefinition and Aim of EpidemiologyJeevan KumarNo ratings yet
- Suicide in Utah 2020Document6 pagesSuicide in Utah 2020McKenzie StaufferNo ratings yet
- Pedia ReviewDocument22 pagesPedia ReviewDebbie LanceroNo ratings yet
- 2012 Resistant HypertensionDocument9 pages2012 Resistant HypertensionBarry Tumpal Wouter NapitupuluNo ratings yet
- Clinical Ophthalmology: Instructions For CandidatesDocument16 pagesClinical Ophthalmology: Instructions For CandidatesdrlawrencekindoNo ratings yet
- 01 Manajemen Risiko Klinik (MRK)Document32 pages01 Manajemen Risiko Klinik (MRK)irmaNo ratings yet
- Nursing Clients With Hematologic DisordersDocument4 pagesNursing Clients With Hematologic DisordersLuna MarieNo ratings yet
- Hidden Pain: Ehlers-Danlos SyndromeDocument28 pagesHidden Pain: Ehlers-Danlos SyndromeVictoria67% (3)
- Home EconomicsDocument5 pagesHome EconomicsNicole Kathleen Caranto100% (1)
- Theatre Practice StandardsDocument54 pagesTheatre Practice StandardsNugroho WibisonoNo ratings yet
- Part Iv - Level 3 Hospital: Attachment 3.A - PersonnelDocument18 pagesPart Iv - Level 3 Hospital: Attachment 3.A - PersonnelIAN LAPINGNo ratings yet
- Complex Regional Pain SyndromeDocument24 pagesComplex Regional Pain SyndromeJanine RustNo ratings yet
- Nanotechnology For Biomedical ApplicationsDocument15 pagesNanotechnology For Biomedical ApplicationsVanitha AlagarsamyNo ratings yet
- MCN Drill 1Document23 pagesMCN Drill 1Cai Velasco DecenaNo ratings yet
- Book - OT Manager - Chap 57 Organizational EthicsDocument9 pagesBook - OT Manager - Chap 57 Organizational EthicsWhitney JosephNo ratings yet
- Health Benefits of Barley PDFDocument4 pagesHealth Benefits of Barley PDFYusrinaNoorAzizahNo ratings yet
- Adriene Vialpando: ExperienceDocument3 pagesAdriene Vialpando: ExperienceKritika NigamNo ratings yet
- Intussuseption and Hirschprung's DiseaseDocument5 pagesIntussuseption and Hirschprung's DiseaseAris Magallanes100% (2)
- Prevalence of Rifampicin Resistance Tuberculosis and Associated Factors Among Presumptive TB or MDRDocument3 pagesPrevalence of Rifampicin Resistance Tuberculosis and Associated Factors Among Presumptive TB or MDRTigray OutlookNo ratings yet
- TeleHealth Lecture NotesDocument40 pagesTeleHealth Lecture NotesKarthik100% (3)
- O Conceito de Saúde e A Diferença Entre Promoção e PrevençãoDocument9 pagesO Conceito de Saúde e A Diferença Entre Promoção e PrevençãoBreno CostaNo ratings yet
- 121 CD 2012Document36 pages121 CD 2012Bounna PhoumalavongNo ratings yet
- Tripping Over The Truth: How The Metabolic Theory of Cancer Is Overturning One of Medicine's Most Entrenched Paradigms - Travis ChristoffersonDocument5 pagesTripping Over The Truth: How The Metabolic Theory of Cancer Is Overturning One of Medicine's Most Entrenched Paradigms - Travis Christoffersonwehyryji0% (1)