Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Optimizing Thyroid Medications Ebook-3Document133 pagesOptimizing Thyroid Medications Ebook-3martuca100% (1)
- Case Study HypothyroidismDocument6 pagesCase Study HypothyroidismGabriela Valdivia100% (2)
- Urn Uvci 01 Ro Yd731x8e2voz1dl92xngp046lrm59w#tDocument2 pagesUrn Uvci 01 Ro Yd731x8e2voz1dl92xngp046lrm59w#tGeorge HonciugNo ratings yet
- UntitledDocument4 pagesUntitledCharisse Alexia DinopolNo ratings yet
- Hafnia AlveiDocument5 pagesHafnia AlveiluisNo ratings yet
- Brugada SyndromeDocument5 pagesBrugada SyndromevitriaNo ratings yet
- Public Health Nursing Population Centered Health Care in The Community Stanhope 8th Edition Test BankDocument3 pagesPublic Health Nursing Population Centered Health Care in The Community Stanhope 8th Edition Test BankMichael SingletonNo ratings yet
- Autism and EpilepsyDocument5 pagesAutism and Epilepsyclarajimena25No ratings yet
- Sindrom Uko Ene Osobe (Moersch-Woltman) : Lije Vjesn 2010 132:110-114Document5 pagesSindrom Uko Ene Osobe (Moersch-Woltman) : Lije Vjesn 2010 132:110-114bimtolaNo ratings yet
- Ski Injury Trauma Gallery Original PicturesDocument12 pagesSki Injury Trauma Gallery Original PicturesSurgicalgownNo ratings yet
- Arthroscopy: If You Have Persistent Joint Pain, Your Doctor May Suggest ArthrosDocument4 pagesArthroscopy: If You Have Persistent Joint Pain, Your Doctor May Suggest ArthrosCaty RamosNo ratings yet
- Spinal Cord Injury Without Radiological AbnormalitDocument3 pagesSpinal Cord Injury Without Radiological Abnormalitcollestein christdianNo ratings yet
- Lennox Gastaut SyndromeDocument12 pagesLennox Gastaut SyndromedulcejuvennyNo ratings yet
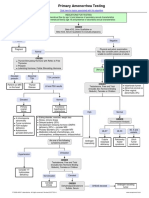
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- PasienDocument12 pagesPasienDharma Abdi Riel ManullangNo ratings yet
- Omacor: Municipal Planning and Development OfficeDocument9 pagesOmacor: Municipal Planning and Development OfficeArthur MericoNo ratings yet
- AchillodyniaDocument1 pageAchillodyniaBos NaibahoNo ratings yet
- HEALTH ASSESSMENT Module 1Document52 pagesHEALTH ASSESSMENT Module 1Sharifa Badaria AtalNo ratings yet
- Canine Parvo VirusDocument60 pagesCanine Parvo VirusPutrina SiregarNo ratings yet
- Dissociative DisordersDocument24 pagesDissociative DisordersSimón Ortiz LondoñoNo ratings yet
- UCLA Mobile Eye Clinic 2019 Needs AssessmentDocument1 pageUCLA Mobile Eye Clinic 2019 Needs AssessmentUMEC Young Professionals InitiativeNo ratings yet
- Ophthalmology Clinical Cases pixOpOpDocument61 pagesOphthalmology Clinical Cases pixOpOpUsman ImtiazNo ratings yet
- Authorization To Walk HomeDocument50 pagesAuthorization To Walk HomeAidan FranciscoNo ratings yet
- Journal Pre-Proof: Advances in Chronic Kidney DiseaseDocument19 pagesJournal Pre-Proof: Advances in Chronic Kidney DiseaseAbdul RokhmanNo ratings yet
- 1 Introduction To Medical JurisprudenceDocument2 pages1 Introduction To Medical JurisprudenceMowanNo ratings yet
- TachycardiaDocument12 pagesTachycardiaPuskesmas Pinang JayaNo ratings yet
- Nursing Care PlanDocument9 pagesNursing Care PlanRenea Joy ArruejoNo ratings yet
- Psychiatric Exam Part 1Document7 pagesPsychiatric Exam Part 1Charmaine Danica MadridNo ratings yet
- Ground Floor Plan (Main Building Facility: Project Title John Paul Silloren PiteroDocument1 pageGround Floor Plan (Main Building Facility: Project Title John Paul Silloren PiteroBryan Silloren PiteroNo ratings yet
- S.subashini Hospital Waste ManagementDocument70 pagesS.subashini Hospital Waste ManagementVenkatram PrabhuNo ratings yet