Download as pdf or txt
You might also like
- Alkaloids (1) PPTDocument11 pagesAlkaloids (1) PPTKavin Kutti0% (1)
- Antibiotics PDFDocument8 pagesAntibiotics PDFSarah JaneNo ratings yet
- Clinical Pharmacokinetics and Pharmacodynamics: Dr. Abaasi KabogoDocument52 pagesClinical Pharmacokinetics and Pharmacodynamics: Dr. Abaasi KabogoNina100% (1)
- An Updated Systematic Review of The Therapeutic Role of Hydroxychloroquine in Coronavirus Disease 19 (COVID 19)Document11 pagesAn Updated Systematic Review of The Therapeutic Role of Hydroxychloroquine in Coronavirus Disease 19 (COVID 19)johngeniusboyNo ratings yet
- Title: Finding The Dose For Hydroxychloroquine Prophylaxis For COVID-19 The Desperate Search ForDocument12 pagesTitle: Finding The Dose For Hydroxychloroquine Prophylaxis For COVID-19 The Desperate Search FormiNo ratings yet
- An EU Programme of COVID-19 Convalescent PlasmaDocument14 pagesAn EU Programme of COVID-19 Convalescent Plasmaazizk83No ratings yet
- HCQ MecanismoDocument8 pagesHCQ MecanismoPau Lo JakobyNo ratings yet
- Challenges For A Broad International Implementation of The Current Severe Community Acquired Pneumonia GuidelinesDocument13 pagesChallenges For A Broad International Implementation of The Current Severe Community Acquired Pneumonia GuidelinesDimitri GusmaoNo ratings yet
- Auto DockDocument7 pagesAuto Dockalealer2708No ratings yet
- D3Targets 2019 nCoV A Webserver For Predicting Drug Target - 2020 - Acta PharmaDocument10 pagesD3Targets 2019 nCoV A Webserver For Predicting Drug Target - 2020 - Acta PharmaMohammed Shuaib AhmedNo ratings yet
- Clinical Pharmacy Therapeu - 2020 - Covert - Utility of The Respiratory Viral Panel As An Antimicrobial Stewardship ToolDocument9 pagesClinical Pharmacy Therapeu - 2020 - Covert - Utility of The Respiratory Viral Panel As An Antimicrobial Stewardship ToolArthur Portillo DiazNo ratings yet
- Preprints ChloroquineDocument24 pagesPreprints ChloroquineJorgelina BernetNo ratings yet
- Role of Procalcitonin in Diagnosis of Community Acquired Pneumonia in ChildrenDocument9 pagesRole of Procalcitonin in Diagnosis of Community Acquired Pneumonia in ChildrenYasminNo ratings yet
- Gao2020 Article InSilicoScreeningOfPotentialChDocument6 pagesGao2020 Article InSilicoScreeningOfPotentialChIndira ShintaNo ratings yet
- Diagnostic and Prognostic Biomarkers of Sepsis in Critical CareDocument8 pagesDiagnostic and Prognostic Biomarkers of Sepsis in Critical Caremr_curiousityNo ratings yet
- Cytokine Adsorption-LancetDocument2 pagesCytokine Adsorption-Lancetbemi.fiNo ratings yet
- COVID-19: A Recommendation To Examine The Effect of Hydroxychloroquine in Preventing Infection and ProgressionDocument4 pagesCOVID-19: A Recommendation To Examine The Effect of Hydroxychloroquine in Preventing Infection and ProgressionDaniel ChávezNo ratings yet
- 1 s2.0 S1201971220300990 MainDocument8 pages1 s2.0 S1201971220300990 MainValiza nasya faatihahNo ratings yet
- 2020 Article 5149Document16 pages2020 Article 5149Annisa SetyantiNo ratings yet
- Yao Et Al., 2023Document10 pagesYao Et Al., 2023hasan andrianNo ratings yet
- Bassetti PCTDocument6 pagesBassetti PCTFaishal Ahmad FarrosiNo ratings yet
- COVID-19 A Recommendation To ExamineDocument4 pagesCOVID-19 A Recommendation To ExamineDayalisis E. RodriguezNo ratings yet
- QFErSU s13613 021 00816 6Document8 pagesQFErSU s13613 021 00816 6Dicky WahyudiNo ratings yet
- Update On Newer Approaches To Prevent or Treat COVDocument3 pagesUpdate On Newer Approaches To Prevent or Treat COVDwi Rachma Cahyati 06No ratings yet
- Journal Pre-Proof: Journal of Infection and Public HealthDocument25 pagesJournal Pre-Proof: Journal of Infection and Public HealthMohammed Shuaib AhmedNo ratings yet
- Artikel 4-1Document6 pagesArtikel 4-1Faizzal AdmajaaNo ratings yet
- Communication: Update On Use of Chloroquine/hydroxychloroquine To Treat Coronavirus Disease 2019 (COVID-19)Document3 pagesCommunication: Update On Use of Chloroquine/hydroxychloroquine To Treat Coronavirus Disease 2019 (COVID-19)IndraNo ratings yet
- Emergence of A Novel Coronavirus Disease (COVID-19) and The Importance of Diagnostic TestingDocument8 pagesEmergence of A Novel Coronavirus Disease (COVID-19) and The Importance of Diagnostic TestingpoopNo ratings yet
- Apa GituDocument8 pagesApa GituRiadi RifqiNo ratings yet
- 2019 Role of Procalcitonin in Predicting Etiology in Bacteremic PatientsDocument6 pages2019 Role of Procalcitonin in Predicting Etiology in Bacteremic PatientsAlex RojasNo ratings yet
- 11111Document19 pages11111Nejc KovačNo ratings yet
- Potential Therapeutic Effects of Dipyridamole in The S - 2020 - Acta PharmaceutiDocument11 pagesPotential Therapeutic Effects of Dipyridamole in The S - 2020 - Acta PharmaceutiMohammed Shuaib AhmedNo ratings yet
- Actividad Pubmeb # 1: Lina Maria Murgas Orozco BioinfomaticaDocument6 pagesActividad Pubmeb # 1: Lina Maria Murgas Orozco BioinfomaticaLina MurgasNo ratings yet
- European Journal of Pharmacology: Zhe Jin, Jing-Yi Liu, Rang Feng, Lu Ji, Zi-Li Jin, Hai-Bo LiDocument7 pagesEuropean Journal of Pharmacology: Zhe Jin, Jing-Yi Liu, Rang Feng, Lu Ji, Zi-Li Jin, Hai-Bo LiIndah Indryani UNo ratings yet
- Cerebrospinal Fluid Penetration of Fosfomycin in Patients With Ventriculitis An Observational StudyDocument7 pagesCerebrospinal Fluid Penetration of Fosfomycin in Patients With Ventriculitis An Observational Studyd4rkgr455No ratings yet
- Clinical Microbiology and Infection: Denise J. Wooding, Horacio BachDocument11 pagesClinical Microbiology and Infection: Denise J. Wooding, Horacio BachendaNo ratings yet
- Art 9Document13 pagesArt 9Génesis LeónNo ratings yet
- Proteomics Clinical Apps - 2023 - Brogna - Detection of Recombinant Spike Protein in The Blood of Individuals VaccinatedDocument7 pagesProteomics Clinical Apps - 2023 - Brogna - Detection of Recombinant Spike Protein in The Blood of Individuals Vaccinatedgoyapatez2No ratings yet
- 1 s2.0 S2352771420301622 Main PDFDocument7 pages1 s2.0 S2352771420301622 Main PDFVella SufaNo ratings yet
- PBPK Modeling and Simulation in Drug Research and 2016 Acta Pharmaceutica SiDocument11 pagesPBPK Modeling and Simulation in Drug Research and 2016 Acta Pharmaceutica Siydftxt6d2yNo ratings yet
- Bepridil Is Potent Against SARS-CoV-2 in VitroDocument28 pagesBepridil Is Potent Against SARS-CoV-2 in VitrosovalaxNo ratings yet
- Ofae059 240401 164437Document9 pagesOfae059 240401 164437Eduardo WaiserNo ratings yet
- Recent Advances and Potential Applications of Human Pluripotent Stem Cell-Derived PancreaticDocument8 pagesRecent Advances and Potential Applications of Human Pluripotent Stem Cell-Derived PancreaticAqsa ParveenNo ratings yet
- Efficacy and Nephrotoxicity of Polymyxin B in Elderly Patients With Carbapenem Resistant Bacterial InfectionDocument12 pagesEfficacy and Nephrotoxicity of Polymyxin B in Elderly Patients With Carbapenem Resistant Bacterial Infectiond4rkgr455No ratings yet
- Jurnal Soal DDocument15 pagesJurnal Soal DrianarahmadhanyNo ratings yet
- Journal Pre-Proof: Travel Medicine and Infectious DiseaseDocument13 pagesJournal Pre-Proof: Travel Medicine and Infectious Diseasepankaj dagurNo ratings yet
- Efficacy of Levofloxacin in The Treatment of BK Viremia - A Multicenter, Double-Blinded, Randomized, Placebo-Controlled Trial - PMCDocument15 pagesEfficacy of Levofloxacin in The Treatment of BK Viremia - A Multicenter, Double-Blinded, Randomized, Placebo-Controlled Trial - PMCWEE LENG GANNo ratings yet
- Antibody Responses and The Effects of Clinical Drugs in COVID-19 PatientsDocument11 pagesAntibody Responses and The Effects of Clinical Drugs in COVID-19 PatientsrehanaNo ratings yet
- Antibiotics 11 01664Document15 pagesAntibiotics 11 01664Ottofianus Hewick KalangiNo ratings yet
- Clinical Evaluation of Selected Pharmacological Treatments Used For Coronavirus (COVID-19) PandemicDocument5 pagesClinical Evaluation of Selected Pharmacological Treatments Used For Coronavirus (COVID-19) PandemicAbdulsalamNo ratings yet
- Comparative Pharmacokinetics of The Three Echinocandins in ICU PatientsDocument8 pagesComparative Pharmacokinetics of The Three Echinocandins in ICU PatientsAris DokoumetzidisNo ratings yet
- Pulmonoary Drug Delivery Review 2021Document21 pagesPulmonoary Drug Delivery Review 2021xeNo ratings yet
- On Absorption Modeling and Food Effect Prediction of Rivaroxaban, A BCS II Drug Orally Administered As An Immediate-Release TabletDocument22 pagesOn Absorption Modeling and Food Effect Prediction of Rivaroxaban, A BCS II Drug Orally Administered As An Immediate-Release TabletAyanda KakazaNo ratings yet
- Optimization of Flucloxacillin Dosing Regimens in Critically Ill Patients Using Population Pharmacokinetic Modelling of Total and Unbound ConcentrationsDocument9 pagesOptimization of Flucloxacillin Dosing Regimens in Critically Ill Patients Using Population Pharmacokinetic Modelling of Total and Unbound ConcentrationsMehdi El HassaniNo ratings yet
- Diagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical TechnologyDocument11 pagesDiagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical Technologycarmen rosa secce pedrazaNo ratings yet
- Antibiotics 13 00072 v222Document22 pagesAntibiotics 13 00072 v222drnguyenbvtkNo ratings yet
- FFFFFDocument15 pagesFFFFFandreiapalmeiraNo ratings yet
- Gut Dysbiosis and Fecal Calprotectin Predict Response To Immune CheckpointDocument10 pagesGut Dysbiosis and Fecal Calprotectin Predict Response To Immune CheckpointMartinaNo ratings yet
- Molecules 26 00175 v2Document16 pagesMolecules 26 00175 v2denisaNo ratings yet
- Systematic Review and Meta-Analysis of Ivermectin For Treatment of COVID-19: Evidence Beyond The HypeDocument25 pagesSystematic Review and Meta-Analysis of Ivermectin For Treatment of COVID-19: Evidence Beyond The HypeDaniel Dario Hernandez TobonNo ratings yet
- Carbapenem Alternatives For Treatment of Bloodstream Infections Due To AmpC Producing EnterobacteralesDocument6 pagesCarbapenem Alternatives For Treatment of Bloodstream Infections Due To AmpC Producing Enterobacteralesd4rkgr455No ratings yet
- Nejmoa 2019014Document12 pagesNejmoa 2019014Samuel SebastianNo ratings yet
- SARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19From EverandSARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19Rating: 3 out of 5 stars3/5 (1)
- Diabetic Ketoacidosis Complicating Gestational Dia - 2022 - AACE Clinical Case RDocument3 pagesDiabetic Ketoacidosis Complicating Gestational Dia - 2022 - AACE Clinical Case RMohammed Shuaib AhmedNo ratings yet
- A Novel Missense CASR Gene Sequence Variation Resulting - 2022 - AACE Clinical CDocument5 pagesA Novel Missense CASR Gene Sequence Variation Resulting - 2022 - AACE Clinical CMohammed Shuaib AhmedNo ratings yet
- A Case of Hypophysitis Associated With SARS CoV 2 - 2022 - AACE Clinical Case RDocument6 pagesA Case of Hypophysitis Associated With SARS CoV 2 - 2022 - AACE Clinical Case RMohammed Shuaib AhmedNo ratings yet
- A Boy With Progressive Cognitive Impairment and Da - 2022 - AACE Clinical Case RDocument2 pagesA Boy With Progressive Cognitive Impairment and Da - 2022 - AACE Clinical Case RMohammed Shuaib AhmedNo ratings yet
- Metabolic Dysregulation and Emerging Therapeutical Tar - 2022 - Acta PharmaceutiDocument23 pagesMetabolic Dysregulation and Emerging Therapeutical Tar - 2022 - Acta PharmaceutiMohammed Shuaib AhmedNo ratings yet
- Medicinal Chemistry Strategies Towards The Development - 2022 - Acta PharmaceutiDocument19 pagesMedicinal Chemistry Strategies Towards The Development - 2022 - Acta PharmaceutiMohammed Shuaib AhmedNo ratings yet
- Inhibiting Collagen I Production and Tumor Cell Colonizatio - 2022 - Acta PharmaDocument13 pagesInhibiting Collagen I Production and Tumor Cell Colonizatio - 2022 - Acta PharmaMohammed Shuaib AhmedNo ratings yet
- Coexistence of Cushing Disease With A Solitary Adrenocor - 2022 - AACE ClinicalDocument4 pagesCoexistence of Cushing Disease With A Solitary Adrenocor - 2022 - AACE ClinicalMohammed Shuaib AhmedNo ratings yet
- Inhibition of Temperature Sensitive TRPV3 Channel by Two Na - 2022 - Acta PharmaDocument12 pagesInhibition of Temperature Sensitive TRPV3 Channel by Two Na - 2022 - Acta PharmaMohammed Shuaib AhmedNo ratings yet
- The Cell Cycle Inhibitor P21 Promotes The Development of - 2022 - Acta PharmaceDocument12 pagesThe Cell Cycle Inhibitor P21 Promotes The Development of - 2022 - Acta PharmaceMohammed Shuaib AhmedNo ratings yet
- Targeting Whole Body Metabolism and Mitochondrial Bioener - 2022 - Acta PharmaceDocument21 pagesTargeting Whole Body Metabolism and Mitochondrial Bioener - 2022 - Acta PharmaceMohammed Shuaib AhmedNo ratings yet
- Preclinical Evaluation and Pilot Clinical Study of 18F Al - 2022 - Acta PharmacDocument9 pagesPreclinical Evaluation and Pilot Clinical Study of 18F Al - 2022 - Acta PharmacMohammed Shuaib AhmedNo ratings yet
- Table of Contents - 2022 - Acta Pharmaceutica Sinica BDocument11 pagesTable of Contents - 2022 - Acta Pharmaceutica Sinica BMohammed Shuaib AhmedNo ratings yet
- Adrenal Histoplasmosis A Therapeutic Restoration of - 2022 - AACE Clinical CaseDocument2 pagesAdrenal Histoplasmosis A Therapeutic Restoration of - 2022 - AACE Clinical CaseMohammed Shuaib AhmedNo ratings yet
- AACE Clinical Case Reports: John C. Parker, MD, Andreas G. Moraitis, MD, Joseph K. Belanoff, MDDocument5 pagesAACE Clinical Case Reports: John C. Parker, MD, Andreas G. Moraitis, MD, Joseph K. Belanoff, MDMohammed Shuaib AhmedNo ratings yet
- AACE Clinical Case Reports: Simrun K. Bal, MD, Meredith J. Sorensen, MD, Andrew Robert Crawford, MDDocument4 pagesAACE Clinical Case Reports: Simrun K. Bal, MD, Meredith J. Sorensen, MD, Andrew Robert Crawford, MDMohammed Shuaib AhmedNo ratings yet
- 1 s2.0 S0165032723013836 MainDocument8 pages1 s2.0 S0165032723013836 MainJorge SalazarNo ratings yet
- Introduction To Pharmacology Introduction To PharmacologyDocument46 pagesIntroduction To Pharmacology Introduction To Pharmacologyagama_lNo ratings yet
- Pengadaan Maret 2023Document2 pagesPengadaan Maret 2023Endah Masmulia NNo ratings yet
- Prescription Regulation Summary Chart: March 2020Document3 pagesPrescription Regulation Summary Chart: March 2020Sylvia AmakaNo ratings yet
- Revised PR Summer 2024 Poona College of Pharmacy, 2nd April 2024Document19 pagesRevised PR Summer 2024 Poona College of Pharmacy, 2nd April 2024Dhaval TelangNo ratings yet
- Chlorthalidone HygrotonDocument2 pagesChlorthalidone HygrotonLIEZEL GRACE VELAYONo ratings yet
- MDP CH 01Document6 pagesMDP CH 01Nishchaya SinghNo ratings yet
- An Up-To-Date Review of Digoxin Toxicity and Its ManagementDocument6 pagesAn Up-To-Date Review of Digoxin Toxicity and Its ManagementNusieba IbrahimNo ratings yet
- DM GiaDocument169 pagesDM GiaVăn Diện ĐinhNo ratings yet
- Adult Infusion StandardsDocument11 pagesAdult Infusion StandardsNathalia OchoaNo ratings yet
- Usp Catalog20100910-DlDocument258 pagesUsp Catalog20100910-DlrobykokaNo ratings yet
- Rundown Acara Seminar Internasional 25Document2 pagesRundown Acara Seminar Internasional 25Ros Nila100% (1)
- Silodosin Versus Tamsulosin in Symptomatic Benign Prostatic Hyperplasia-Our ExperienceDocument3 pagesSilodosin Versus Tamsulosin in Symptomatic Benign Prostatic Hyperplasia-Our ExperienceIOSR Journal of PharmacyNo ratings yet
- DSP 16 - 08 - 23Document34 pagesDSP 16 - 08 - 23Iffa FelasyifaNo ratings yet
- HNBB Drug StudyDocument2 pagesHNBB Drug StudyJennah Ricci Tuazon100% (4)
- Guaifenesin: What Is in This LeafletDocument6 pagesGuaifenesin: What Is in This LeafletKate Felongco CambelNo ratings yet
- Gastrointestinal DrugsDocument11 pagesGastrointestinal DrugsAbby MataNo ratings yet
- Osmotic Pump DDSDocument11 pagesOsmotic Pump DDSRumaisa FatimaNo ratings yet
- Sedative-Hypnotic Drugs: Michael H. Nelson, PH.D., R.PHDocument10 pagesSedative-Hypnotic Drugs: Michael H. Nelson, PH.D., R.PHHan HopperNo ratings yet
- Infectious Diseases Society of America Guidelines On The Treatment and Management of Pa - Tients With COVID-19, 14 MARTIE 2023 PDFDocument56 pagesInfectious Diseases Society of America Guidelines On The Treatment and Management of Pa - Tients With COVID-19, 14 MARTIE 2023 PDFdavid mangaloiuNo ratings yet
- Assignment No. 002 STSDocument2 pagesAssignment No. 002 STSSteffie Anne GavinaNo ratings yet
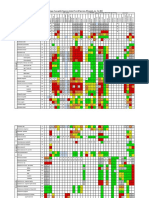
- Organism: Percentage of Susceptible Organisms Isolated From All Specimen, 83 Hospitals, Jan - Dec 2020Document2 pagesOrganism: Percentage of Susceptible Organisms Isolated From All Specimen, 83 Hospitals, Jan - Dec 2020BaronKornNo ratings yet
- First Time in The History of CdscoDocument2 pagesFirst Time in The History of Cdscoshahbaz6299No ratings yet
- Protein Binding of DrugDocument22 pagesProtein Binding of DrugManikanta GupthaNo ratings yet
- Dubai Community Pharmacy Licensure and Pharmaceutical Practices GuideDocument27 pagesDubai Community Pharmacy Licensure and Pharmaceutical Practices GuidedharmeswarNo ratings yet
- Drugs and Drug Development StagesDocument50 pagesDrugs and Drug Development StagesmotlhankanalaronaNo ratings yet
- Guidelines On Safe Use of High Alert Medications (Version 2 April 2019)Document13 pagesGuidelines On Safe Use of High Alert Medications (Version 2 April 2019)Eman MohamedNo ratings yet