
Wegener's Granulomatosis
Wegener's Granulomatosis
You might also like
- Sarcoidosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandSarcoidosis, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (1)
- Doctors OrderDocument10 pagesDoctors OrderJan Mikhail Frasco100% (4)
- VasculitisDocument42 pagesVasculitissamaNo ratings yet
- Pathoma Lecture Notes 2017Document42 pagesPathoma Lecture Notes 2017Priyesh PrinceNo ratings yet
- Acute GlomerulonephritisDocument7 pagesAcute GlomerulonephritisSel CuaNo ratings yet
- VasculitisDocument5 pagesVasculitisFatima GamalNo ratings yet
- C C C CC C: Adiong, Joanne Ignacio, Dianne Grace Julian, MarivicDocument9 pagesC C C CC C: Adiong, Joanne Ignacio, Dianne Grace Julian, MarivicufrieNo ratings yet
- 06-TB 1Document51 pages06-TB 1Mihraban OmerNo ratings yet
- Comp of #Document19 pagesComp of #Shamini MargammuthuNo ratings yet
- Objective - SURGERYDocument54 pagesObjective - SURGERYlaraNo ratings yet
- Polyarteritis NodosaDocument10 pagesPolyarteritis Nodosaaaron mbindyoNo ratings yet
- Interstitial Lung Diseases Radiology 22222Document26 pagesInterstitial Lung Diseases Radiology 22222Daniel AshooriNo ratings yet
- Summaru 2023Document126 pagesSummaru 2023kgjmjvq2stNo ratings yet
- 4 - VasculitisDocument22 pages4 - VasculitisIrakli GhlontiNo ratings yet
- Wegeners GranulomatosisDocument65 pagesWegeners GranulomatosisLily HaslinaNo ratings yet
- Acute Glomerulonephritis (AGN)Document5 pagesAcute Glomerulonephritis (AGN)smashayielNo ratings yet
- BehcetsDocument4 pagesBehcetsKate ClarksonNo ratings yet
- Renal and Perinephric Abscess - UpToDateDocument27 pagesRenal and Perinephric Abscess - UpToDate76q88b4yrxNo ratings yet
- Interstitial Lung Diseases RadiologyDocument26 pagesInterstitial Lung Diseases RadiologyDaniel AshooriNo ratings yet
- NephritisDocument5 pagesNephritisPooja ChapdiNo ratings yet
- Urinary PropedDocument52 pagesUrinary PropedDivesh DarshanNo ratings yet
- Buerger'S Disease: Brief DescriptionDocument5 pagesBuerger'S Disease: Brief DescriptionJanine P. Dela CruzNo ratings yet
- Kidney Cross Section: by Mayo Clinic StaffDocument7 pagesKidney Cross Section: by Mayo Clinic StaffReavin FuentesNo ratings yet
- Buergers Disease, Thoracic Outlet Syndrome & AneurysmDocument21 pagesBuergers Disease, Thoracic Outlet Syndrome & AneurysmrohitNo ratings yet
- Extra-Cranial Complications of CSOMfinalDocument37 pagesExtra-Cranial Complications of CSOMfinalAarthi Gopal100% (2)
- SyringomyeliaDocument9 pagesSyringomyeliashodhgangaNo ratings yet
- Transient SynovitisDocument9 pagesTransient SynovitisMuhammad Taufik AdhyatmaNo ratings yet
- Set 3 COMP-2Document71 pagesSet 3 COMP-2Appu ayyalaNo ratings yet
- Orbital CellulitisDocument42 pagesOrbital Cellulitismuhammad iqbalNo ratings yet
- Case PresentationDocument59 pagesCase PresentationKaneez FatimaNo ratings yet
- Lecturio Granulomatosis With PolyangitisDocument6 pagesLecturio Granulomatosis With PolyangitisPranjali WeladiNo ratings yet
- Systemic: Manifestations Erythema NodosumDocument6 pagesSystemic: Manifestations Erythema NodosumMuhammad ZubaidiNo ratings yet
- Pott's Disease PDFDocument14 pagesPott's Disease PDFRaja RajanNo ratings yet
- Pleurisy, Pleural Effusion, Emphysema, Pulmonary Edema and ARS (CORROS)Document64 pagesPleurisy, Pleural Effusion, Emphysema, Pulmonary Edema and ARS (CORROS)Jam CorrosNo ratings yet
- Dysplasia & Multicystic KidneyDocument8 pagesDysplasia & Multicystic KidneyShintia MalindaNo ratings yet
- Rheumatoid ArthritisDocument45 pagesRheumatoid ArthritisParamedis BluescopeNo ratings yet
- Buergers Disease, Thoracic Outlet Syndrome & AneurysmDocument21 pagesBuergers Disease, Thoracic Outlet Syndrome & AneurysmrohitNo ratings yet
- Yanyan 2Document48 pagesYanyan 2Nuraine OthmanNo ratings yet
- Course 5 Pleuro-Pulmonary Surgical SemiologyDocument23 pagesCourse 5 Pleuro-Pulmonary Surgical SemiologyvladutNo ratings yet
- Acute Appendicitis in Adults - Clinical Manifestations and Differential Diagnosis - UpToDateDocument9 pagesAcute Appendicitis in Adults - Clinical Manifestations and Differential Diagnosis - UpToDateSebastian CamachoNo ratings yet
- Complications of FracturesDocument13 pagesComplications of FracturesmilananandNo ratings yet
- Pterigium Dan Pendarahan SubkonjungtivaDocument20 pagesPterigium Dan Pendarahan SubkonjungtivaRasya DanardhonoNo ratings yet
- Lecture Combined PDFDocument81 pagesLecture Combined PDFPrincess Aira Bucag CarbonelNo ratings yet
- Nephritis by Triveni SidhaDocument23 pagesNephritis by Triveni SidhaTriveni SidhaNo ratings yet
- Pott DiseaseDocument15 pagesPott DiseasejunkirinNo ratings yet
- Bronchiectasis: Reported by Jehanne CalingaDocument16 pagesBronchiectasis: Reported by Jehanne CalingaJehanne CalingaNo ratings yet
- Symptoms: Thromboangiitis ObliteransDocument5 pagesSymptoms: Thromboangiitis ObliteransDuke Vladimir SuarezNo ratings yet
- Bronchiectasis DesieDocument77 pagesBronchiectasis DesieAbebe GelawNo ratings yet
- Cogan Syndrome Surger 4, AnkitDocument18 pagesCogan Syndrome Surger 4, AnkitAnkit Tonger AnkyNo ratings yet
- 4 Respiratory ExaminationsDocument53 pages4 Respiratory Examinationscawsey mohamedNo ratings yet
- D17B PresentationDocument28 pagesD17B PresentationBruno KandatamNo ratings yet
- ClubbingDocument4 pagesClubbingAlfrin AntonyNo ratings yet
- Chronic Glumerulonephritis HandoutsDocument8 pagesChronic Glumerulonephritis HandoutsLanzen DragneelNo ratings yet
- GlomerulonephritisDocument16 pagesGlomerulonephritisamalaros22No ratings yet
- Interstitial Lung Disease (ILD)Document42 pagesInterstitial Lung Disease (ILD)AkhilaNo ratings yet
- Surgical Nursing (III)Document32 pagesSurgical Nursing (III)Opio MosesNo ratings yet
- Rheumatoid ArthritisDocument53 pagesRheumatoid ArthritisnsamariosNo ratings yet
- Disease of PleuraDocument25 pagesDisease of PleuragodzahadesNo ratings yet
- Septicarthritis 110426090729 Phpapp02Document21 pagesSepticarthritis 110426090729 Phpapp02Diana MayasariNo ratings yet
- Lokesh RanaDocument19 pagesLokesh RanaOlga GoryachevaNo ratings yet
- Throat Diseases and SepsisDocument15 pagesThroat Diseases and SepsisOlga GoryachevaNo ratings yet
- Treatment of Erectile DysfunctionDocument25 pagesTreatment of Erectile DysfunctionOlga GoryachevaNo ratings yet
- Lokesh Rana AKIDocument30 pagesLokesh Rana AKIOlga GoryachevaNo ratings yet
- Algorithm For Helping With Cardiac ArrestDocument52 pagesAlgorithm For Helping With Cardiac ArrestOlga GoryachevaNo ratings yet
- Hypovolemic ShockDocument21 pagesHypovolemic ShockOlga GoryachevaNo ratings yet
- How To Stop Paroxysm of SVT and AF at Home and in HospitalDocument35 pagesHow To Stop Paroxysm of SVT and AF at Home and in HospitalOlga Goryacheva100% (1)
- ERECTILE DysfunctionDocument32 pagesERECTILE DysfunctionOlga GoryachevaNo ratings yet
- Acute Coronary Syndrome - Management, Diagnostics and TreatmentDocument27 pagesAcute Coronary Syndrome - Management, Diagnostics and TreatmentOlga GoryachevaNo ratings yet
- Hepato Pulmonary: Syndrome by Piyush Barwal and Abhishek RajDocument30 pagesHepato Pulmonary: Syndrome by Piyush Barwal and Abhishek RajOlga GoryachevaNo ratings yet
- Pacemaker SyndromeDocument26 pagesPacemaker SyndromeOlga GoryachevaNo ratings yet
- Small - Intestinal Neoplasms and Carcinoid TumorsDocument51 pagesSmall - Intestinal Neoplasms and Carcinoid TumorsOlga GoryachevaNo ratings yet
- Behcet's SyndromeDocument18 pagesBehcet's SyndromeOlga GoryachevaNo ratings yet
- Colorectal Cancer: By:-Vaibhav SwarupDocument18 pagesColorectal Cancer: By:-Vaibhav SwarupOlga GoryachevaNo ratings yet
- Vascular Disease of The BowelDocument28 pagesVascular Disease of The BowelOlga GoryachevaNo ratings yet
- Pulmonary EosinophiliaDocument19 pagesPulmonary EosinophiliaOlga GoryachevaNo ratings yet
- Irritable Bowel SyndromeDocument19 pagesIrritable Bowel SyndromeOlga GoryachevaNo ratings yet
- Pulmonary Sequestration: by - Happy Malik (3 Course)Document43 pagesPulmonary Sequestration: by - Happy Malik (3 Course)Olga GoryachevaNo ratings yet
- Empyema: By-Komal JaiswalDocument29 pagesEmpyema: By-Komal JaiswalOlga GoryachevaNo ratings yet
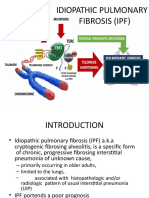
- Idiopathic Pulmonary FibrosisDocument52 pagesIdiopathic Pulmonary FibrosisOlga GoryachevaNo ratings yet
- Eisenmenger SyndromeDocument17 pagesEisenmenger SyndromeOlga GoryachevaNo ratings yet
- Ebstein Anomaly: By:-Vaibhav SwarupDocument22 pagesEbstein Anomaly: By:-Vaibhav SwarupOlga GoryachevaNo ratings yet
- Myocarditis and Pericarditis in ECGDocument34 pagesMyocarditis and Pericarditis in ECGOlga GoryachevaNo ratings yet
- Tetralogy of FallotDocument22 pagesTetralogy of FallotOlga GoryachevaNo ratings yet
- Complications of Myocardial Infarction in ECGDocument39 pagesComplications of Myocardial Infarction in ECGOlga GoryachevaNo ratings yet
- Cor Triatriatum: Edited by - HAPPY MALIK (3 Year Student)Document26 pagesCor Triatriatum: Edited by - HAPPY MALIK (3 Year Student)Olga GoryachevaNo ratings yet
- Isolated Congenital Aortic Valve DiseaseDocument24 pagesIsolated Congenital Aortic Valve DiseaseOlga GoryachevaNo ratings yet
- Perioperative NursingDocument18 pagesPerioperative Nursinglagunda100% (2)
- Dr. Neelu Mundhada (Agrawal) : Fellowship in Paediatric OphthalmologyDocument3 pagesDr. Neelu Mundhada (Agrawal) : Fellowship in Paediatric OphthalmologyNeelu MundhadaAgrawalNo ratings yet
- ISlabDocument3 pagesISlabpixiedustNo ratings yet
- WPW With Af Case ReportDocument4 pagesWPW With Af Case Report王怡君No ratings yet
- Epidemiology Of, Risk Factors For, and Possible Causes of Rheumatoid Arthritis - UpToDateDocument13 pagesEpidemiology Of, Risk Factors For, and Possible Causes of Rheumatoid Arthritis - UpToDateNova YuniscaNo ratings yet
- Peptic Ulcer DiseaseDocument22 pagesPeptic Ulcer Diseaserosamundrae100% (1)
- BUMC MEDLINE Plus/OVID Fact Sheet: Alumni Medical Library Boston University Medical CenterDocument2 pagesBUMC MEDLINE Plus/OVID Fact Sheet: Alumni Medical Library Boston University Medical CenterRay PermanaNo ratings yet
- CHN CH 4 Maternal and Child Care Including Bemonc and CemoncDocument5 pagesCHN CH 4 Maternal and Child Care Including Bemonc and CemoncElaiza RiegoNo ratings yet
- Presention SdaDocument13 pagesPresention SdaBikhu MatreNo ratings yet
- Hering's Three Rules ArticleDocument5 pagesHering's Three Rules Articlemikembad100% (1)
- Avoid Spot Treat HeatDocument1 pageAvoid Spot Treat HeatMichael CooperNo ratings yet
- Health Emergency Kits Training 2019 PDFDocument33 pagesHealth Emergency Kits Training 2019 PDFrema_rhere95No ratings yet
- Tugas Basing 1Document2 pagesTugas Basing 1Alfrits TampemawaNo ratings yet
- Best Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihDocument7 pagesBest Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihARS University BandungNo ratings yet
- Pediatric Nursing Dissertation TopicsDocument8 pagesPediatric Nursing Dissertation TopicsCustomCollegePaperCanada100% (1)
- Cavernous Sinus Thrombosis of Odontogenic Origin: March 2016Document8 pagesCavernous Sinus Thrombosis of Odontogenic Origin: March 2016Putu WidiastriNo ratings yet
- Hipertiroidism - EnglezaDocument13 pagesHipertiroidism - Englezaalexya2008No ratings yet
- CV KPM Jan 2020Document13 pagesCV KPM Jan 2020Prof. Dr. Kamlesh MehtaNo ratings yet
- Senior Project Paper FinalDocument5 pagesSenior Project Paper Finalapi-281742815No ratings yet
- 8C Summary SheetDocument2 pages8C Summary Sheet박찬우100% (2)
- Helicobacter Pylori, Diagnosis and TreatmentDocument7 pagesHelicobacter Pylori, Diagnosis and TreatmentTrifan_DumitruNo ratings yet
- Abortion Nursing Care Planning and ManagementDocument11 pagesAbortion Nursing Care Planning and ManagementSyamsiah ChandrawatiNo ratings yet
- PractocleDocument10 pagesPractoclePalwasha KhanNo ratings yet
- Pooja Gangwar:::: Patient Age / Sex 23 Y / Female BranchDocument1 pagePooja Gangwar:::: Patient Age / Sex 23 Y / Female BranchSnehal GholapNo ratings yet
- Nursing Performance Checklist TracheostomyDocument3 pagesNursing Performance Checklist TracheostomySyahrilKiyai100% (1)
- Policy InformationDocument20 pagesPolicy InformationMandyLynnEdwardsNo ratings yet
- Skeletal Anchorage in Orthodontics With Mini and MicrosrewsDocument8 pagesSkeletal Anchorage in Orthodontics With Mini and Microsrewso_eisa2002No ratings yet
- Nasal Lacrimal Duct ObstructionDocument2 pagesNasal Lacrimal Duct ObstructionAgitha Melita PutriNo ratings yet
- Shortened Dental ArchDocument9 pagesShortened Dental ArchSanjay HirekodiNo ratings yet



















































































































Download as pdf or txt
You might also like
- Sarcoidosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandSarcoidosis, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (1)
- Doctors OrderDocument10 pagesDoctors OrderJan Mikhail Frasco100% (4)
- VasculitisDocument42 pagesVasculitissamaNo ratings yet
- Pathoma Lecture Notes 2017Document42 pagesPathoma Lecture Notes 2017Priyesh PrinceNo ratings yet
- Acute GlomerulonephritisDocument7 pagesAcute GlomerulonephritisSel CuaNo ratings yet
- VasculitisDocument5 pagesVasculitisFatima GamalNo ratings yet
- C C C CC C: Adiong, Joanne Ignacio, Dianne Grace Julian, MarivicDocument9 pagesC C C CC C: Adiong, Joanne Ignacio, Dianne Grace Julian, MarivicufrieNo ratings yet
- 06-TB 1Document51 pages06-TB 1Mihraban OmerNo ratings yet
- Comp of #Document19 pagesComp of #Shamini MargammuthuNo ratings yet
- Objective - SURGERYDocument54 pagesObjective - SURGERYlaraNo ratings yet
- Polyarteritis NodosaDocument10 pagesPolyarteritis Nodosaaaron mbindyoNo ratings yet
- Interstitial Lung Diseases Radiology 22222Document26 pagesInterstitial Lung Diseases Radiology 22222Daniel AshooriNo ratings yet
- Summaru 2023Document126 pagesSummaru 2023kgjmjvq2stNo ratings yet
- 4 - VasculitisDocument22 pages4 - VasculitisIrakli GhlontiNo ratings yet
- Wegeners GranulomatosisDocument65 pagesWegeners GranulomatosisLily HaslinaNo ratings yet
- Acute Glomerulonephritis (AGN)Document5 pagesAcute Glomerulonephritis (AGN)smashayielNo ratings yet
- BehcetsDocument4 pagesBehcetsKate ClarksonNo ratings yet
- Renal and Perinephric Abscess - UpToDateDocument27 pagesRenal and Perinephric Abscess - UpToDate76q88b4yrxNo ratings yet
- Interstitial Lung Diseases RadiologyDocument26 pagesInterstitial Lung Diseases RadiologyDaniel AshooriNo ratings yet
- NephritisDocument5 pagesNephritisPooja ChapdiNo ratings yet
- Urinary PropedDocument52 pagesUrinary PropedDivesh DarshanNo ratings yet
- Buerger'S Disease: Brief DescriptionDocument5 pagesBuerger'S Disease: Brief DescriptionJanine P. Dela CruzNo ratings yet
- Kidney Cross Section: by Mayo Clinic StaffDocument7 pagesKidney Cross Section: by Mayo Clinic StaffReavin FuentesNo ratings yet
- Buergers Disease, Thoracic Outlet Syndrome & AneurysmDocument21 pagesBuergers Disease, Thoracic Outlet Syndrome & AneurysmrohitNo ratings yet
- Extra-Cranial Complications of CSOMfinalDocument37 pagesExtra-Cranial Complications of CSOMfinalAarthi Gopal100% (2)
- SyringomyeliaDocument9 pagesSyringomyeliashodhgangaNo ratings yet
- Transient SynovitisDocument9 pagesTransient SynovitisMuhammad Taufik AdhyatmaNo ratings yet
- Set 3 COMP-2Document71 pagesSet 3 COMP-2Appu ayyalaNo ratings yet
- Orbital CellulitisDocument42 pagesOrbital Cellulitismuhammad iqbalNo ratings yet
- Case PresentationDocument59 pagesCase PresentationKaneez FatimaNo ratings yet
- Lecturio Granulomatosis With PolyangitisDocument6 pagesLecturio Granulomatosis With PolyangitisPranjali WeladiNo ratings yet
- Systemic: Manifestations Erythema NodosumDocument6 pagesSystemic: Manifestations Erythema NodosumMuhammad ZubaidiNo ratings yet
- Pott's Disease PDFDocument14 pagesPott's Disease PDFRaja RajanNo ratings yet
- Pleurisy, Pleural Effusion, Emphysema, Pulmonary Edema and ARS (CORROS)Document64 pagesPleurisy, Pleural Effusion, Emphysema, Pulmonary Edema and ARS (CORROS)Jam CorrosNo ratings yet
- Dysplasia & Multicystic KidneyDocument8 pagesDysplasia & Multicystic KidneyShintia MalindaNo ratings yet
- Rheumatoid ArthritisDocument45 pagesRheumatoid ArthritisParamedis BluescopeNo ratings yet
- Buergers Disease, Thoracic Outlet Syndrome & AneurysmDocument21 pagesBuergers Disease, Thoracic Outlet Syndrome & AneurysmrohitNo ratings yet
- Yanyan 2Document48 pagesYanyan 2Nuraine OthmanNo ratings yet
- Course 5 Pleuro-Pulmonary Surgical SemiologyDocument23 pagesCourse 5 Pleuro-Pulmonary Surgical SemiologyvladutNo ratings yet
- Acute Appendicitis in Adults - Clinical Manifestations and Differential Diagnosis - UpToDateDocument9 pagesAcute Appendicitis in Adults - Clinical Manifestations and Differential Diagnosis - UpToDateSebastian CamachoNo ratings yet
- Complications of FracturesDocument13 pagesComplications of FracturesmilananandNo ratings yet
- Pterigium Dan Pendarahan SubkonjungtivaDocument20 pagesPterigium Dan Pendarahan SubkonjungtivaRasya DanardhonoNo ratings yet
- Lecture Combined PDFDocument81 pagesLecture Combined PDFPrincess Aira Bucag CarbonelNo ratings yet
- Nephritis by Triveni SidhaDocument23 pagesNephritis by Triveni SidhaTriveni SidhaNo ratings yet
- Pott DiseaseDocument15 pagesPott DiseasejunkirinNo ratings yet
- Bronchiectasis: Reported by Jehanne CalingaDocument16 pagesBronchiectasis: Reported by Jehanne CalingaJehanne CalingaNo ratings yet
- Symptoms: Thromboangiitis ObliteransDocument5 pagesSymptoms: Thromboangiitis ObliteransDuke Vladimir SuarezNo ratings yet
- Bronchiectasis DesieDocument77 pagesBronchiectasis DesieAbebe GelawNo ratings yet
- Cogan Syndrome Surger 4, AnkitDocument18 pagesCogan Syndrome Surger 4, AnkitAnkit Tonger AnkyNo ratings yet
- 4 Respiratory ExaminationsDocument53 pages4 Respiratory Examinationscawsey mohamedNo ratings yet
- D17B PresentationDocument28 pagesD17B PresentationBruno KandatamNo ratings yet
- ClubbingDocument4 pagesClubbingAlfrin AntonyNo ratings yet
- Chronic Glumerulonephritis HandoutsDocument8 pagesChronic Glumerulonephritis HandoutsLanzen DragneelNo ratings yet
- GlomerulonephritisDocument16 pagesGlomerulonephritisamalaros22No ratings yet
- Interstitial Lung Disease (ILD)Document42 pagesInterstitial Lung Disease (ILD)AkhilaNo ratings yet
- Surgical Nursing (III)Document32 pagesSurgical Nursing (III)Opio MosesNo ratings yet
- Rheumatoid ArthritisDocument53 pagesRheumatoid ArthritisnsamariosNo ratings yet
- Disease of PleuraDocument25 pagesDisease of PleuragodzahadesNo ratings yet
- Septicarthritis 110426090729 Phpapp02Document21 pagesSepticarthritis 110426090729 Phpapp02Diana MayasariNo ratings yet
- Lokesh RanaDocument19 pagesLokesh RanaOlga GoryachevaNo ratings yet
- Throat Diseases and SepsisDocument15 pagesThroat Diseases and SepsisOlga GoryachevaNo ratings yet
- Treatment of Erectile DysfunctionDocument25 pagesTreatment of Erectile DysfunctionOlga GoryachevaNo ratings yet
- Lokesh Rana AKIDocument30 pagesLokesh Rana AKIOlga GoryachevaNo ratings yet
- Algorithm For Helping With Cardiac ArrestDocument52 pagesAlgorithm For Helping With Cardiac ArrestOlga GoryachevaNo ratings yet
- Hypovolemic ShockDocument21 pagesHypovolemic ShockOlga GoryachevaNo ratings yet
- How To Stop Paroxysm of SVT and AF at Home and in HospitalDocument35 pagesHow To Stop Paroxysm of SVT and AF at Home and in HospitalOlga Goryacheva100% (1)
- ERECTILE DysfunctionDocument32 pagesERECTILE DysfunctionOlga GoryachevaNo ratings yet
- Acute Coronary Syndrome - Management, Diagnostics and TreatmentDocument27 pagesAcute Coronary Syndrome - Management, Diagnostics and TreatmentOlga GoryachevaNo ratings yet
- Hepato Pulmonary: Syndrome by Piyush Barwal and Abhishek RajDocument30 pagesHepato Pulmonary: Syndrome by Piyush Barwal and Abhishek RajOlga GoryachevaNo ratings yet
- Pacemaker SyndromeDocument26 pagesPacemaker SyndromeOlga GoryachevaNo ratings yet
- Small - Intestinal Neoplasms and Carcinoid TumorsDocument51 pagesSmall - Intestinal Neoplasms and Carcinoid TumorsOlga GoryachevaNo ratings yet
- Behcet's SyndromeDocument18 pagesBehcet's SyndromeOlga GoryachevaNo ratings yet
- Colorectal Cancer: By:-Vaibhav SwarupDocument18 pagesColorectal Cancer: By:-Vaibhav SwarupOlga GoryachevaNo ratings yet
- Vascular Disease of The BowelDocument28 pagesVascular Disease of The BowelOlga GoryachevaNo ratings yet
- Pulmonary EosinophiliaDocument19 pagesPulmonary EosinophiliaOlga GoryachevaNo ratings yet
- Irritable Bowel SyndromeDocument19 pagesIrritable Bowel SyndromeOlga GoryachevaNo ratings yet
- Pulmonary Sequestration: by - Happy Malik (3 Course)Document43 pagesPulmonary Sequestration: by - Happy Malik (3 Course)Olga GoryachevaNo ratings yet
- Empyema: By-Komal JaiswalDocument29 pagesEmpyema: By-Komal JaiswalOlga GoryachevaNo ratings yet
- Idiopathic Pulmonary FibrosisDocument52 pagesIdiopathic Pulmonary FibrosisOlga GoryachevaNo ratings yet
- Eisenmenger SyndromeDocument17 pagesEisenmenger SyndromeOlga GoryachevaNo ratings yet
- Ebstein Anomaly: By:-Vaibhav SwarupDocument22 pagesEbstein Anomaly: By:-Vaibhav SwarupOlga GoryachevaNo ratings yet
- Myocarditis and Pericarditis in ECGDocument34 pagesMyocarditis and Pericarditis in ECGOlga GoryachevaNo ratings yet
- Tetralogy of FallotDocument22 pagesTetralogy of FallotOlga GoryachevaNo ratings yet
- Complications of Myocardial Infarction in ECGDocument39 pagesComplications of Myocardial Infarction in ECGOlga GoryachevaNo ratings yet
- Cor Triatriatum: Edited by - HAPPY MALIK (3 Year Student)Document26 pagesCor Triatriatum: Edited by - HAPPY MALIK (3 Year Student)Olga GoryachevaNo ratings yet
- Isolated Congenital Aortic Valve DiseaseDocument24 pagesIsolated Congenital Aortic Valve DiseaseOlga GoryachevaNo ratings yet
- Perioperative NursingDocument18 pagesPerioperative Nursinglagunda100% (2)
- Dr. Neelu Mundhada (Agrawal) : Fellowship in Paediatric OphthalmologyDocument3 pagesDr. Neelu Mundhada (Agrawal) : Fellowship in Paediatric OphthalmologyNeelu MundhadaAgrawalNo ratings yet
- ISlabDocument3 pagesISlabpixiedustNo ratings yet
- WPW With Af Case ReportDocument4 pagesWPW With Af Case Report王怡君No ratings yet
- Epidemiology Of, Risk Factors For, and Possible Causes of Rheumatoid Arthritis - UpToDateDocument13 pagesEpidemiology Of, Risk Factors For, and Possible Causes of Rheumatoid Arthritis - UpToDateNova YuniscaNo ratings yet
- Peptic Ulcer DiseaseDocument22 pagesPeptic Ulcer Diseaserosamundrae100% (1)
- BUMC MEDLINE Plus/OVID Fact Sheet: Alumni Medical Library Boston University Medical CenterDocument2 pagesBUMC MEDLINE Plus/OVID Fact Sheet: Alumni Medical Library Boston University Medical CenterRay PermanaNo ratings yet
- CHN CH 4 Maternal and Child Care Including Bemonc and CemoncDocument5 pagesCHN CH 4 Maternal and Child Care Including Bemonc and CemoncElaiza RiegoNo ratings yet
- Presention SdaDocument13 pagesPresention SdaBikhu MatreNo ratings yet
- Hering's Three Rules ArticleDocument5 pagesHering's Three Rules Articlemikembad100% (1)
- Avoid Spot Treat HeatDocument1 pageAvoid Spot Treat HeatMichael CooperNo ratings yet
- Health Emergency Kits Training 2019 PDFDocument33 pagesHealth Emergency Kits Training 2019 PDFrema_rhere95No ratings yet
- Tugas Basing 1Document2 pagesTugas Basing 1Alfrits TampemawaNo ratings yet
- Best Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihDocument7 pagesBest Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihARS University BandungNo ratings yet
- Pediatric Nursing Dissertation TopicsDocument8 pagesPediatric Nursing Dissertation TopicsCustomCollegePaperCanada100% (1)
- Cavernous Sinus Thrombosis of Odontogenic Origin: March 2016Document8 pagesCavernous Sinus Thrombosis of Odontogenic Origin: March 2016Putu WidiastriNo ratings yet
- Hipertiroidism - EnglezaDocument13 pagesHipertiroidism - Englezaalexya2008No ratings yet
- CV KPM Jan 2020Document13 pagesCV KPM Jan 2020Prof. Dr. Kamlesh MehtaNo ratings yet
- Senior Project Paper FinalDocument5 pagesSenior Project Paper Finalapi-281742815No ratings yet
- 8C Summary SheetDocument2 pages8C Summary Sheet박찬우100% (2)
- Helicobacter Pylori, Diagnosis and TreatmentDocument7 pagesHelicobacter Pylori, Diagnosis and TreatmentTrifan_DumitruNo ratings yet
- Abortion Nursing Care Planning and ManagementDocument11 pagesAbortion Nursing Care Planning and ManagementSyamsiah ChandrawatiNo ratings yet
- PractocleDocument10 pagesPractoclePalwasha KhanNo ratings yet
- Pooja Gangwar:::: Patient Age / Sex 23 Y / Female BranchDocument1 pagePooja Gangwar:::: Patient Age / Sex 23 Y / Female BranchSnehal GholapNo ratings yet
- Nursing Performance Checklist TracheostomyDocument3 pagesNursing Performance Checklist TracheostomySyahrilKiyai100% (1)
- Policy InformationDocument20 pagesPolicy InformationMandyLynnEdwardsNo ratings yet
- Skeletal Anchorage in Orthodontics With Mini and MicrosrewsDocument8 pagesSkeletal Anchorage in Orthodontics With Mini and Microsrewso_eisa2002No ratings yet
- Nasal Lacrimal Duct ObstructionDocument2 pagesNasal Lacrimal Duct ObstructionAgitha Melita PutriNo ratings yet
- Shortened Dental ArchDocument9 pagesShortened Dental ArchSanjay HirekodiNo ratings yet