Professional Documents
Culture Documents
Research Report
Research Report
Uploaded by
Thanwarat PongvichaiOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Research Report
Research Report
Uploaded by
Thanwarat PongvichaiCopyright:
Available Formats
Research Report
Motor Control Exercises, Sling
Exercises, and General Exercises for
Patients With Chronic Low Back Pain:
A Randomized Controlled Trial With
1-Year Follow-up
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
Monica Unsgaard-Tøndel, Anne Margrethe Fladmark, Øyvind Salvesen,
Ottar Vasseljen
M. Unsgaard-Tøndel, MSc, is a PhD
candidate in the Department of
Public Health and General Practice,
Background. Exercise benefits patients with chronic nonspecific low back pain;
Faculty of Medicine, Norwegian Uni- however, the most effective type of exercise remains unknown.
versity of Science and Technology,
Trondheim, Norway. Mailing ad- Objective. This study compared outcomes after motor control exercises, sling
dress: Department of Public Health exercises, and general exercises for low back pain.
and General Practice, Norwegian
University of Science and Technol-
ogy, Faculty of Medicine, Medisinsk Design. This was a randomized controlled trial with a 1-year follow-up.
Teknisk Forskningssenter, 7489
Trondheim, Norway. Address all Setting. The study was conducted in a primary care setting in Norway.
correspondence to Mrs Unsgaard-
Tøndel at: monica.unsgaard. Patients. The participants were patients with chronic nonspecific low back pain
tondel@ntnu.no.
(n!109).
A.M. Fladmark, MSc, is Research
Assistant, Department of Public Interventions. The interventions in this study were low-load motor control
Health and General Practice, Fac-
exercises, high-load sling exercises, or general exercises, all delivered by experienced
ulty of Medicine, Norwegian Uni-
versity of Science and Technology. physical therapists, once a week for 8 weeks.
Ø. Salvesen, MSc, is Assistant Measurements. The primary outcome measure was pain reported on the Nu-
Professor, Department of Cancer
Research and Molecular Medi- meric Pain Rating Scale after treatment and at a 1-year follow-up. Secondary outcome
cine, Faculty of Medicine, Nor- measures were self-reported activity limitation (assessed with the Oswestry Disability
wegian University of Science and Index), clinically examined function (assessed with the Fingertip-to-Floor Test), and
Technology. fear-avoidance beliefs after intervention.
O. Vasseljen, PhD, is Associate
Professor, Department of Public Results. The postintervention assessment showed no significant differences
Health and General Practice, Fac- among groups with respect to pain (overall group difference) or any of the outcome
ulty of Medicine, Norwegian Uni- measures. Mean (95% confidence interval) group differences for pain reduction after
versity of Science and Technology.
treatment and after 1 year were 0.3 ("0.7 to 1.3) and 0.4 ("0.7 to 1.4) for motor
[Unsgaard-Tøndel M, Fladmark control exercises versus sling exercises, 0.7 ("0.6 to 2.0) and 0.3 ("0.8 to 1.4) for
AM, Salvesen Ø, Vasseljen O. Mo- sling exercises versus general exercises, and 1.0 ("0.1 to 2.0) and 0.7 ("0.3 to 1.7)
tor control exercises, sling exer-
cises, and general exercises for pa-
for motor control exercises versus general exercises.
tients with chronic low back pain:
a randomized controlled trial with Limitations. The nature of the interventions made blinding impossible.
1-year follow-up. Phys Ther. 2010;
90:1426 –1440.] Conclusions. This study gave no evidence that 8 treatments with individually
© 2010 American Physical Therapy instructed motor control exercises or sling exercises were superior to general exer-
Association cises for chronic low back pain.
Post a Rapid Response to
this article at:
ptjournal.apta.org
1426 f Physical Therapy Volume 90 Number 10 October 2010
Exercises for Patients With Chronic Low Back Pain
N
onspecific low back pain ery in both the short term and long ferent effects compared with either
(LBP) is a major public health term, but that the improvements were high-load motor control exercises
problem in industrialized soci- small.20 Another study that added spe- potentially stimulating both local
eties, with lifetime prevalence be- cific stabilization exercises to general and global supporting lumbar mus-
tween 60% and 85%.1 Reviews point exercises, however, did not provide cles when performed in neutral
to beneficial effects of supervised any evidence of beneficial effects on spine positions or general exer-
exercises in people with chronic pain and disability.21 According to cises designed for strength (force-
LBP,2,3 but there is no clear evidence Richardson et al,22 the first step in re- generating capacity) and flexibility.
that any specific type of exercise is habilitating motor skill is to train the
better than other forms of exer- patient to cognitively contract the The purpose of this study was to
cise.4 – 6 The term “specific exercise” deep trunk muscles independently. compare supervised low-load (pri-
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
has been used to describe quite dif- The ADIM has been emphasized in the marily ADIM) motor control exer-
ferent types of exercises, such as sta- early phase of exercises to regain con- cises and supervised high-load sling
bilization exercises and abdominal trol of the deep abdominal muscles exercises with general exercises in
drawing-in maneuver (ADIM),7,8 indi- and provide stability to the lumbar the early phase of rehabilitation for
vidualized exercises,9 supervised ex- spine before progressing to heavier patients with chronic LBP. Primary
ercises,10 and even what appear to exercises. This low-load exercise ap- outcome measures were pain after
be general exercises.11,12 It is plausi- proach has been met with consider- intervention and at a 1-year follow-up.
ble, therefore, that specifically tar- able criticism by other authors who Secondary outcome measures were
geted exercises with potential bene- argued that stability of the spine disability, fear avoidance, and trunk
fits relative to more general exercises should be targeted by forceful abdom- flexibility after intervention.
may be concealed when different inal muscle contraction.23,24 Whether
studies are summarized in reviews. the ADIM has a direct effect on pain Method
and function and how the effect of Setting and Participants
Motor control exercises for the deep such low-load exercises compares A randomized controlled trial with 3
trunk muscles were introduced for with that of high-load or general exer- intervention groups was conducted,
patients with chronic LBP based on cises in the early phase of rehabili- with participants recruited from gen-
evidence of motor control dysfunc- tation have not been studied. Hypo- eral practitioners or physical thera-
tion, including delayed onset of ac- thetically, low-load motor control pists (29/109) and by announcement
tivity in the transversus abdominis exercises targeting local supporting to employees at a large local hospital
(TrA) and internal oblique abdomi- lumbar muscles may produce dif- (80/109) in Norway. The employees
nal muscles13 and segmental hyper-
trophy of the lumbar multifidus mus-
cle.14 Early studies that tried to target
these discrepancies with specific in- The Bottom Line
terventions15–19 provided promising
evidence for beneficial effects. A re- What do we already know about this topic?
cent placebo-controlled study of pa-
tients with chronic LBP confirmed Supervised exercises benefit patients with chronic nonspecific low back
that motor control exercises pro- pain; however, the most effective type of exercise remains unknown.
duced improvements in both activity
What new information does this study offer?
and patients’ impressions of recov-
This study compared motor control exercises, sling exercises, and general
exercises in the early phase of rehabilitation for patients with chronic non-
Available With specific low back pain. A course of 8 treatments did not show any overall
This Article at group differences in pain, self-reported activity limitation, or function.
ptjournal.apta.org
If you’re a patient, what might these findings mean
• The Bottom Line Podcast
for you?
• Audio Abstracts Podcast
These 3 exercise programs appear to be equally effective, so you should
This article was published ahead of
print on July 29, 2010, at choose a program based on such issues as program availability, the costs
ptjournal.apta.org. of each program, and your preferences.
October 2010 Volume 90 Number 10 Physical Therapy f 1427
Exercises for Patients With Chronic Low Back Pain
and participants recruited from the
health care providers had similar pain
levels and ages. The participants in-
cluded were 19 to 60 years of age with
chronic nonspecific LBP of at least 3
months’ duration and with pain at pre-
sentation between 2 and 10 on the
Numeric Pain Rating Scale (NPRS) (0 –
10).25 Participants were excluded for
the following reasons: previous back
surgery, radiating pain below the knee
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
or neurologic signs from nerve-root
compression, systemic or widespread
pain, overweight preventing ultra-
sound imaging, pregnancy, diagnosed
psychiatric disease, sick leave for more
than 1 year, recipient of disability ben-
efits, unresolved social security or in-
surance problems, or insufficient lan-
guage capabilities. Written informed
consent was given by all participants
before randomization.
Randomization and
Interventions
Participants were randomly assigned
to 1 of 3 treatment groups: (1) those
who received low-load, individually
instructed, ultrasound-guided motor
control exercises (MCE group);
(2) those who received high-load, in-
dividually instructed sling exercises
(SE group); or (3) those who received
general exercises (GE group). Eligibil-
ity was assessed by a research physical
therapist, and enrolled patients were
randomly assigned to groups after the
pretreatment assessment. The ran-
domization was administered by an
independent study secretary via tele-
phone. The secretary consecutively re-
ported group allocation for included
participants from a list of random
numbers between 0 and 1 that were
computationally generated. Partici-
pants with numbers in the lower third
of the interval were assigned to the
MCE group, those in the middle third
of the interval were assigned to the SE
group, and those in the upper third of
the interval were assigned to the GE
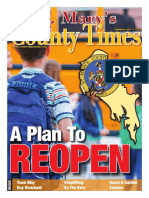
Figure 1. group. The column of random num-
Exercise interventions in the study: (A) motor control exercises, (B) sling exercises, bers was arbitrarily subdivided into
and (C) general exercises. variable blocks of 3 to 9 to obtain even
1428 f Physical Therapy Volume 90 Number 10 October 2010
Exercises for Patients With Chronic Low Back Pain
distribution of participants in the continuously monitored by direct ob- The supported position where the
groups. servation of respiration and by real- participants could no longer main-
time b-mode ultrasound imaging of su- tain the neutral spine position was
The participants in all treatment perficial and deep muscle activity. used as the baseline for further exer-
groups attended treatment once a Activity in the abdominal muscles was cise progression. By placing the par-
week for 8 weeks. The attendance at visualized on the ultrasound screen for ticipants in demanding but pain-free
weekly treatment sessions was re- each participant and used for feedback positions and asking them to hold
corded, but adherence to home ex- in all treatment sessions. Participants the spine in neutral, the aim was to
ercise was not recorded. All partici- also were instructed in pelvic-floor activate the deep and superficial sta-
pants were encouraged to stay active and multifidus muscle contractions. bilizing trunk muscles (local and
in their daily life, as recommended Furthermore, a goal was to obtain con- global muscles). When weakness,
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
by systematic reviews on advice for trolled co-contraction of the TrA, the pain, fatigue, or asymmetry was iden-
management of LBP.26 In addition, all deep fibers of the multifidus muscle, tified, this position served as starting
participants received a booklet with and the pelvic-floor muscles while point for training and further pro-
general information on LBP provided keeping other muscles relaxed. Partic- gression. The number of repetitions
by the Norwegian Network of Back ipants who achieved isolated activity and sets was individually adjusted ac-
Pain (http://www.formi.no; in Nor- of the TrA in the supine position pro- cording to pain and fatigue (Appen-
wegian) that also emphasized bene- gressed to activation of the TrA simi- dix 2). The sling exercises were per-
fits of varied physical activity for non- larly in sitting and standing positions. formed for 40 minutes once a week
specific LBP. Participants were not in a physical therapy clinic.
allowed to receive other treatment for Toward the end of the intervention
LBP during the intervention period. period, the participants were in- General exercises. The general
structed to incorporate the ADIM exercise intervention is shown in
Motor control exercises. The mo- into activities of daily living. Written Figure 1C. This group received gen-
tor control exercise intervention is instruction to carry out the ADIM at eral trunk strengthening and stretch-
shown in Figure 1A. The motor con- home was provided, and participants ing exercises, as recommended in the
trol treatments lasted 40 minutes and were encouraged to perform 10 management of nonspecific LBP.21,32
took place in an outpatient clinic. The pain-free contractions 2 to 3 times Exercises were instructed by a phys-
low-load motor control exercises were per day, holding each contraction for ical therapist and performed in small
individualized and taught by a spe- 10 seconds.22 groups of 2 to 8 people. Exercises
cially trained physical therapist ac- performed were, for instance, trunk
cording to a protocol on therapeutic Sling exercises. The sling exercise extension, flexion, and rotation with
exercise for lumbopelvic stabiliza- intervention is shown in Figure 1B. resistance and stretching of trunk
tion27 and ultrasound imaging.28,29 The participants in this group were and extremity muscles (Appendix 3).
Ultrasound imaging was used as both a instructed individually by a specially The exercises were performed for 1
teaching tool and an evaluation tool trained physical therapist. The exer- hour weekly in a local fitness center
(separate substudy). Patients with mo- cises were chosen from a predefined with a traditional resistance appa-
tor control deficits may benefit from set of back exercises in slings on the ratus and with 10 repetitions in 3
visual feedback of muscle function basis of an assessment of each par- sets.33,34 The exercise instructor su-
from ultrasound imaging.30 Ultrasound ticipant’s ability to keep the lumbar pervised each participant and indi-
imaging is increasingly used among cli- spine stable in the neutral position vidually directed and adapted the
nicians to retrain motor control in the through a range of leg and arm posi- exercise performance when needed.
deep abdominal muscles. tions and movements (Appendix 1).
The sling method for dosing lum- The physical therapists were experi-
The low-load motor control exercises bopelvic exercises has been assessed enced in the exercise methods
focused on isolated control and activ- in combination with other treatment applied. Participants in all treatment
ity of the TrA during the ADIM.22 The modalities in earlier studies.18,31 Un- groups received home exercises for
aim of the ADIM was to voluntary ac- loading elastic bands were attached flexibility when considered necessary.
tivate TrA thickening and lateral slide to the pelvis to help participants
while the internal oblique and exter- maintain the neutral spine position Outcome Measures
nal oblique abdominal muscles re- at all times and for exercises to Self-reported current pain was the
mained relatively unchanged. The ex- progress without pain. Exercise pro- main outcome measure and was
ercises were executed with low effort gression was achieved by gradually rated using the NPRS (0 –10).25 The
and with relaxed respiration and were reducing the elastic band support. strongest experienced pain in the
October 2010 Volume 90 Number 10 Physical Therapy f 1429
Exercises for Patients With Chronic Low Back Pain
Table 1.
Characteristics of Participants (n!109) in the 3 Intervention Groups for Background and Outcome Variables at Baselinea
MCE Group SE Group GE Group
Variable (n!36) (n!36) (n!37)
Sex, male/female, n 7/29 13/23 13/24
Age (y) 40.9 (11.5) 43.4 (10.2) 36.0 (10.3)
Body mass index, kg/m2 24.9 (3.1) 24.9 (3.1) 24.3 (2.8)
Height (cm) 171.4 (7.7) 172.6 (7.7) 171.2 (8.7)
Weight (kg) 73.3 (11.6) 74.5 (11.6) 71.1 (9.9)
Low back pain, years since first episode, 6.0 (2–19) 9.0 (2–15) 6.0 (3.5–11.5)
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
median (interquartile range)
NPRS (0–10), present at moment 3.3 (1.3) 3.6 (1.7) 3.3 (1.9)
NPRS (0–10), strongest last month 6.0 (2.0) 6.7 (2.4) 5.9 (1.8)
ODI (0–100) 19.4 (7.3) 22.3 (12.1) 20.8 (9.8)
Fingertip-to-Floor Test 11.9 (13.0) 15.0 (12.5) 8.8 (9.7)
FABQ, physical activity 7.8 (5.2) 8.8 (5.6) 9.2 (5.4)
FABQ, work 13.2 (9.2) 14.4 (10.9) 13.2 (8.7)
a
Data are mean (SD) unless otherwise denoted. MCE group received low-load motor control exercises, SE group received high-load sling exercises, and GE
group received general exercises. NPRS!Numeric Pain Rating Scale, ODI!Oswestry Disability Index, FABQ!Fear-Avoidance Beliefs Questionnaire.
previous 4 weeks also was recorded Data Analysis Role of the Funding Source
using the NPRS. The Oswestry Dis- This study was part of a larger The Norwegian Fund for Postgradu-
ability Index (ODI), modified ver- project studying the effects of spe- ate Training in Physiotherapy fi-
sion,35 was used to assess disability,36 cific low back exercises on symp- nanced the study. The funding orga-
also termed “self-reported activity lim- toms and underlying neuromuscular nization had no authority over or
itation,” and the total score was ex- mechanisms in which the sample size input into any part of the study. Sling
pressed as a percentage. The Fear- was determined to detect between- exercise equipment was provided
Avoidance Beliefs Questionnaire group changes in feed-forward ac- without obligations by Redcord AS.
(FABQ)37 was used to address nega- tivity in the TrA with an estimated
tive beliefs that can contribute to effect size of 0.8 (unpublished re- Results
prolonged disability.38 The Fingertip- search). We performed an intention- Recruitment and inclusion of par-
to-Floor Test39 was used to examine to-treat analysis, and used mixed linear ticipants were performed between
the participants’ ability to bend for- models to estimate mean scores, to January 2006 and September 2007.
ward in standing by measuring the estimate baseline-adjusted between- After randomization, 36 patients
distance between the longest finger- group differences, and to test whether were allocated to the MCE group, 36
tip and the floor. Lower scores are baseline-adjusted group differences at patients were allocated to the SE
associated with decreased symptoms posttest were significantly different. group, and 37 patients were allo-
for all outcome measures. Participants completing fewer than 6 cated to the GE group (Tab. 1). All
of the 8 treatment sessions were ex- participants were included in the sta-
All outcome measures were applied cluded from postintervention evalua- tistical analyses, independent of
at baseline and after the intervention tion, but their baseline data were in- completion. One physical therapist
period. Although the baseline assess- cluded in the mixed models analysis. performed interventions for all pa-
ment was performed blinded, the The statistical analyses were per- tients allocated to the MCE group.
physical therapist conducting the post- formed with SPSS version 17.0* and The sling exercise and general exer-
intervention evaluation was not NCSS 2007.† The level for statistical cise interventions were led by 4 al-
blinded to treatment group allocation. significance was set at P!.05. ternating physical therapists. In the
At the 1-year follow-up (14 months af- SE group, the therapists instructed
ter randomization), the participants 22, 8, 4, and 2 participants, respec-
answered a questionnaire on pain and tively. In the GE group, the 4 thera-
health care utilization. The person * SPSS Inc, 233 S Wacker Dr, Chicago, IL pists were continuously alternating.
60606.
who analyzed the data was blinded to †
NCSS, 329 North 1000 East, Kaysville, UT Twelve of 80 participants who were
group assignment. 84037. recruited by announcement at the
1430 f Physical Therapy Volume 90 Number 10 October 2010
Exercises for Patients With Chronic Low Back Pain
Potentially eligible participants (n=120)
Enrollment
Excluded (n=11)
Not meeting inclusion criteria (n=10)
▼
Declined to participate (n=1)
▼
Randomized (n=109)
Allocation
▼ ▼ ▼
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
Motor control exercises (n=36) Sling exercises (n=36) General exercises (n=37)
≤5 sessions: 14% ≤5 sessions: 17% ≤5 sessions: 30%
6-8 sessions: 86% 6-8 sessions: 83% 6-8 sessions: 70%
▼ ▼ ▼
Follow-up
Follow-up Follow-up
Follow-up
7 treatment nonadherence
1 treatment nonadherence 3 withdrawals from the study
3 lost to follow-up
4 lost to follow-up 3 lost to follow-up
1 withdrawal from the study
8 weeks (n=31 [86%]) 8 weeks (n=30 [83%])
8 weeks (n=26 [70%])
1 year (n=30 [83%]) 1 year (n=34 [94%])
1 year (n=33 [89%])
▼ ▼ ▼
Analysis
Analyzed (n=36) Analyzed (n=36) Analyzed (n=37)
Figure 2.
Enrollment of patients and completion of study.
local hospital and 10 of 29 partici- ried out as planned and are de- group compared with the GE group,
pants who were recruited from pri- scribed in the “Method” section. and 1.0 ("0.1 to 2.0) in the MCE
mary care dropped out during the group compared with the GE group
intervention period. Reasons for Postintervention and (P!.19 for overall group difference,
dropouts during the intervention pe- 1-Year Follow-up Assessments Tab. 2). At the 1-year follow-up as-
riod are shown in Figure 2. At the No significant differences were found sessment, group differences in mean
1-year follow-up assessment, 2 peo- among the groups at the postinterven- current pain adjusted for baseline
ple in the MCE and GE groups each tion assessment for pain, activity limi- score were 0.4 ("0.7 to 1.4) in the
and 1 person in the SE group did not tation (ODI), the FTF, fear-avoidance MCE group compared with the SE
return the questionnaire. The people beliefs for physical activity, or fear- group, 0.3 ("0.8 to 1.4) in the SE
who dropped out were compared avoidance beliefs for work (Tab. 2, group compared with the GE group,
with those who completed the study Fig. 3). Mean current pain group dif- and 0.7 ("0.3 to 1.7) in the MCE
for initial score on background and ferences (95% confidence interval) group compared with the GE group
outcome variables at baseline, and after intervention, adjusted for base- (P!.42 for overall group difference).
no significant differences were line score, were 0.3 ("0.7 to 1.3) in Mean adjusted group differences in ac-
found, as indirectly evident in Tables the MCE group compared with the tivity limitation score (ODI) after inter-
1 and 2. The interventions were car- SE group, 0.7 ("0.6 to 2.0) in the SE vention were 0.6 ("4.3 to 5.4) in the
October 2010 Volume 90 Number 10 Physical Therapy f 1431
Exercises for Patients With Chronic Low Back Pain
Table 2.
Estimated Mean (SD) Unadjusted Scores for the Different Treatment Groups and Times and Estimated Mean (95% Confidence
Interval) Baseline-Adjusted Group Differences After Intervention as Given by the Mixed Linear Modelsa
Mean Outcome Adjusted Mean Group Differenceb
MCE Group SE Group GE Group MCE Group vs SE Group vs MCE Group vs
Variable (n!36) (n!36) (n!37) SE Group GE Group GE Group Pc
d
Pain
Current
Baseline 3.31 (1.42) 3.61 (1.75) 3.30 (1.74)
2 mo 1.76 (1.54) 2.34 (2.26) 2.73 (2.32) 0.27 ("0.73 to 1.27) 0.71 ("0.55 to 1.97) 0.97 ("0.08 to 2.03) .19
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
1y 2.01 (1.94) 2.70 (2.22) 2.66 (2.03) 0.39 ("0.65 to 1.44) 0.27 ("0.83 to 1.36) 0.66 ("0.34 to 1.66) .42
Strongest
Baseline 6.25 (1.99) 6.39 (2.32) 6.22 (2.03)
2 mo 4.09 (2.08) 4.80 (2.41) 5.26 (2.74) 0.57 ("0.57 to 1.71) 0.63 ("0.74 to 2.01) 1.20 ("0.03 to 2.44) .15
e
Disability
Baseline 19.44 (8.38) 22.28 (11.22) 20.84 (9.43)
2 mo 12.78 (7.62) 16.18 (10.88) 17.75 (9.63) 0.56 ("4.25 to 5.37) 3.02 ("2.44 to 8.47) 3.58 ("0.47 to 7.63) .21
Trunk flexionf
Baseline 11.94 (10.86) 15.00 (10.86) 8.78 (10.86)
2 mo 7.44 (10.86) 11.13 (10.86) 7.57 (10.86) 0.6 ("3.2 to 4.4) 2.7 ("1.3 to 6.6) 3.3 ("0.7 to 7.3) .23
FABQ, physical
activityg
Baseline 7.75 (5.35) 8.78 (5.82) 9.22 (5.03)
2 mo 7.31 (4.22) 6.76 (5.37) 8.60 (5.14) "1.58 ("4.00 to 0.84) 1.40 ("1.25 to 4.05) "0.18 ("2.42 to 2.07) .41
h
FABQ, work
Baseline 13.19 (9.18) 14.46 (10.26) 13.53 (9.64)
2 mo 11.86 (9.67) 12.72 (9.46) 12.44 (8.80) "0.40 ("3.81 to 3.01) 0.65 ("2.70 to 4.00) 0.25 ("2.74 to 3.24) .93
a
MCE group received low-load motor control exercises, SE group received high-load sling exercises, and GE group received general exercises.
b
Group-wise comparison of estimated mean posttest scores adjusted for baseline, contrast estimates. Positive value indicates greater improvement in first
group.
c
Overall between-groups difference in score after intervention, adjusted for baseline. The P values refer to F tests of whether estimated group differences
were significantly different from zero.
d
Pain as assessed with the Numeric Pain Rating Scale. Score range: 0 (“no pain”) to 10 (“worst imaginable pain”). Strongest pain indicates worst pain
experienced during the last 4 weeks.
e
Disability as assessed with the Oswestry Disability Index. Score range: 0 (no activity limitation) to 100 (full activity limitation) for the 10 functions screened.
f
Trunk flexion as assessed with the Fingertip-to-Floor Test (in centimeters).
g
Fear-Avoidance Beliefs Questionnaire for physical activity. Score range: 0 (no fear) to 24 (maximum fear).
h
Fear-Avoidance Beliefs Questionnaire for work. Score range: 0 (no fear) to 42 (maximum fear).
MCE group compared with the SE LBP the year after intervention. One cent) change in ODI score40 and a
group, 3.0 ("2.4 to 8.5) in the SE participant in the SE group reported 2-point change in NPRS score (0 –10)
group compared with the GE group, adverse effects of the intervention and have been suggested as minimum im-
and 3.6 ("0.5 to 7.6) in MCE group withdrew from the study. portant changes for patients25,40,41
compared with the GE group (P!.21 and have been interpreted to repre-
for overall group difference). Discussion sent clinically relevant between-group
This study compared motor control differences.3 The observed mean ef-
Of the participants, 48% in the MCE exercises, sling exercises, and general fects in this study did not reach these
group, 41% in the SE group, and 50% exercises in the early phase of rehabil- levels. However, we cannot exclude
in the GE group sought therapy for itation for patients with chronic non- that motor control exercises are favor-
LBP the year after intervention specific LBP. A course of 8 treat- able for reducing pain relative to gen-
(Tab. 3), and 24% in the MCE group, ments did not show any overall eral exercises because the clinically
31% in the SE group, and 42% in the group effects in pain, disability, and important difference for pain40 was
GE group used medication because of fear-avoidance beliefs. A 10-unit (per- included in the confidence interval
1432 f Physical Therapy Volume 90 Number 10 October 2010
Exercises for Patients With Chronic Low Back Pain
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
Figure 3.
Mean scores, with 95% confidence intervals, for the outcome measures in each of the 3 intervention groups: (A) pain scores (Numeric
Pain Rating Scale [NPRS]) before and after intervention and at the 1-year follow-up, (B) activity limitation scores (Oswestry Disability
Index) before and after intervention, and (C) distance between fingertip and floor before and after intervention. MCE group received
low-load motor control exercises, SE group received high-load sling exercises, and GE group received general exercises.
Table 3.
Health Care Utilization Before, During, and After (Follow-up Period) the Interventiona
Variable MCE Group SE Group GE Group
Low back pain therapyb
Before 26 (75%) 26 (72%) 21 (57%)
After 14 (48%) 12 (41%) 12 (50%)
Low back pain medication
Before 10 (32%) 8 (27%) 6 (24%)
During 6 (19%) 5 (17%) 7 (27%)
After 7 (24%) 9 (31%) 10 (42%)
a
MCE group received low-load motor control exercises, SE group received high-load sling exercises, and GE group received general exercises.
b
Low back pain treatment administered by a physician, physical therapist, chiropractor, osteopath, or acupuncture practitioner.
October 2010 Volume 90 Number 10 Physical Therapy f 1433
Exercises for Patients With Chronic Low Back Pain
(Tab. 2). The results from this study who were recruited from health care differences in the present study were
gave no evidence of added benefit of providers, there was a difference in larger for pain and smaller for disabil-
specific exercises over general exer- dropout rate (15% versus 40%, respec- ity relative to pooled effect sizes in a
cises for people with chronic LBP. tively). This difference might have review on motor control exercises
been due to a greater degree of moti- versus other forms of exercise.4 An
Certain limitations apply to this study. vation among the participants who 8-week program of motor control ex-
Sample size was calculated based on initiated participation themselves. The ercises resulted in better short-term
desired effects on onset of muscle ac- exercise interventions were carried function, reduced pain, and improved
tivity in the TrA (unpublished re- out to reflect clinical practice, which perceived effect relative to general ex-
search). With the reported effect sizes strengthens generalization and inter- ercises.7 Effect sizes (95% confidence
for pain (Tab. 2), the study would have pretation of the results. interval) for pain after 8 weeks and 1
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
needed 59 participants in each group year were 0.8 (0.1 to 1.6) and 0.3
to declare a difference as statistically Distress and fear-avoidance beliefs ("0.6 to 1.3) in favor of motor control
significant at the P!.05 level (80% can contribute to the maintenance of exercises compared with general ex-
power). Still, for clinically important LBP.42 Exercises may lessen the be- ercises on a scale of 0 to 10. Corre-
changes in pain of 2 points on the havioral, cognitive, and affective as- sponding effect sizes in the present
NPRS, the study had acceptable power pects of chronic nonspecific LBP,43 study were 1.0 ("0.1 to 2.1) and 0.6
(#80%). Blinding is practically impos- but no change in fear-avoidance be- ("0.4 to 1.7) in favor of motor control
sible in exercise interventions. This liefs was observed in this study. exercises. The effect sizes were similar
limitation was mainly critical for the despite a more extensive motor con-
fingertip-to-floor measurements in Motor control exercises for people trol exercise approach in the former
this study because pain, disability, with LBP consist of several stages, study. Costa et al20 compared a com-
and fear avoidance were assessed by from cognitive awareness and isolated prehensive motor control exercise
the participants without interfer- activation of deep trunk muscles to program with placebo ultrasound and
ence of the researchers. Adherence control of movement and stability in shortwave therapy. After 12 treat-
to allocated treatment is important more-complex functional tasks of ments, motor control exercises had
for sound comparison of interven- daily living.22 Motor control theories beneficial effects on global impression
tions, which was the reason for ex- imply that functionally oriented and of recovery, activity, and activity limi-
cluding participants who attended varied exercise should be incorpo- tation. Improvement also was found in
fewer than 6 treatment sessions from rated early in rehabilitation.44,45 The pain intensity at 12 months but not at
the postintervention evaluation. This objective of the motor control exer- 2 and 6 months. The authors argued
exclusion of participants may have cise intervention in this study was to that because the clinical improve-
created biased results. However, increase activity and voluntary control ments were small, some patients and
the baseline data for these individu- of the deep abdominal muscles. Visual clinicians may not consider these ef-
als were included in the mixed feedback from real-time ultrasound fects clinically worthwhile. The cited
model analysis. Twice as many par- imaging was used to optimize perfor- studies and the present study support
ticipants dropped out of the GE mance, which was further empha- the findings of systematic reviews that
group compared with the other ex- sized through individual instruction motor control exercises4 and stabiliz-
ercise groups. If most of the drop- and encouragement by the therapist ing exercises5 are not more effective
outs in the GE group were due to operating the ultrasound device. This or only marginally more effective than
lack of effect, this factor would un- intervention may be regarded as early- general exercises. However, a recent
derestimate the between-groups dif- stage exercises in a more comprehen- review concluded that motor control
ferences (ie, reduce the difference sive motor control exercise program, exercises were better than minimal
between the GE group and the MCE with little focus on integrating the ex- intervention in reducing pain in the
and SE groups). ercises into everyday activities. It is short term, intermediate term, and
possible that a more comprehensive long term by 10 to 15 points on a
Some caution should be advocated in approach encompassing all aspects of 100-point scale, but not better than
generalizing the results to clinical pop- motor control retraining could pro- other forms of exercises.4
ulations. A large proportion of partici- duce different results.
pants were recruited directly by an- The sling exercise intervention ad-
nouncement at a local hospital (73%). The effects of motor control exer- dressed the ability to stabilize the
Although participants who were re- cises in people with chronic LBP lumbar spine while moving the
cruited directly were not differenti- have been investigated in a few stud- lower extremities with unstable sup-
ated by pain symptoms from those ies. The MCE group versus GE group port. Both strength and muscle coor-
1434 f Physical Therapy Volume 90 Number 10 October 2010
Exercises for Patients With Chronic Low Back Pain
dination were needed to maintain toward that observed in individuals Unsgaard-Tøndel and Ms Fladmark provided
the neutral spine position. No dis- who were healthy by as little as 2 data collection, participants, and clerical
support. Mrs Unsgaard-Tøndel, Mr Salvesen,
cernable difference in absenteeism weeks with motor skill training.51
and Dr Vasseljen provided data analysis. Mrs
was found between a sling exercise Only marginal changes in muscle con- Unsgaard-Tøndel, Ms Fladmark, and Dr Vas-
group and a general exercise group traction properties (abdominal muscle seljen provided consultation (including re-
in the only previous study of sling slide and thickness) during the ADIM view of manuscript before submission).
exercises for people with LBP.46 were observed in participants over the The authors thank the Norwegian Fund for
Women with pelvic girdle pain after intervention period in a separate sub- Post-Graduate Training in Physiotherapy for fi-
pregnancy showed significantly study.52 There is a need to scrutinize nancing the study and the physical therapists
lower pain and improved function links between neural mechanisms and at the Multidisciplinary Back Clinic at St. Olav
University Hospital, Trondheim Physiotherapy
after 20 weeks with a specific exer- symptoms to advance outcome mea- Clinic, and Elixia Fitness Centre, for conducting
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
cise program in slings relative to or- sures in LBP research. patient treatments and Redcord AS for supply-
dinary physical therapy.18,19 Individ- ing exercise equipment. They also thank Astrid
ual treatment program was based on Patients with nonspecific LBP con- Woodhouse, Ingrid Riphagen, and Jan Ove
a clinical examination. Compared stitute a heterogeneous group.6 Rein for technical support and Jon Magnussen,
Stephen Lock, and Tor Inge Andersen for com-
with the present trial, a considerably Mechanism-based classification meth- menting on the manuscript.
more extensive sling exercise pro- ods that can identify subgroups in
gram was used in the study by Stuge need of either movement or control The study was approved by the Regional
Ethics Committee.
et al,18 including sling exercises at enhancement have been proposed.53,54
home and motor control exercises The specific exercises in the present The results of this study were presented at
for the deep abdominal muscles. Pos- trial aimed to address muscle dysfunc- the 7th Interdisciplinary World Congress on
Low Back and Pelvic Pain; November 9 –12,
sible additive effects of combining tions,55,56 but subject-specific deficits 2010; Los Angeles, California.
high-load and low-load specific exer- in neuromuscular control were not a
cises, as in the studies by Stuge and selection criterion. To date, classifica- The Norwegian Fund for Post-Graduate Train-
ing in Physiotherapy financed the study.
colleagues,18,19 also should be inves- tion systems for LBP are insufficiently
tigated for nonspecific LBP. supported by scientific evidence.57 The study was preregistered in ClinicalTrials.
Whether exercises tailored to deficits gov with identifier NCT00201513.
The GE group served as control in strength, flexibility, neural firing This article was submitted December 21,
group, and the general exercise in- patterns, or voluntary control of mus- 2009, and was accepted May 31, 2010.
tervention was constructed to ad- cles that stabilize the spine lead to en- DOI: 10.2522/ptj.20090421
here to current evidence of best hanced clinical outcome needs to be
practice,47,48 with advice and super- explored.
vised activity that included strength- References
1 World Health Organization. The burden of
ening and stretching exercises that Conclusion musculoskeletal conditions at the start of
are central in LBP rehabilitation32,48 No significant group differences were the new millennium. 2003. Available at:
http://whqlibdoc.who.int/trs/WHO_
and with individual guidance by a found in pain, disability, trunk flexibil- TRS_919.pdf. Accessed November 2, 2004.
physical therapist when considered ity, or fear-avoidance beliefs after 8 2 Airaksinen O, Brox JI, Cedraschi C, et al.
necessary. The results indicate that weeks of motor control exercises, Chapter 4; European guidelines for the
management of chronic nonspecific low
general exercises could be recom- sling exercises, and general exercises back pain. Eur Spine J. 2006;15(suppl 2):
mended, similar to sling exercises and in patients with chronic nonspecific S192–S300.
motor control exercises, when aiming LBP. However, confidence intervals 3 van Middelkoop M, Rubinstein SM, Verha-
gen AP, et al. Exercise therapy for chronic
to reduce pain and disability in the for improved outcome spanned clini- nonspecific low-back pain. Best Pract Res
early phase of LBP rehabilitation. cally important differences in favor of Clin Rheumatol. 2010;24:193–204.
the motor control exercise interven- 4 Macedo LG, Maher CG, Latimer J, McAuley
JH. Motor control exercise for persistent,
Motor control exercises are intended tion compared with the general exer- nonspecific low back pain: a systematic
to alter underlying neural mechanisms cise intervention, meaning clinically review. Phys Ther. 2009;89:9 –25.
shown to be associated with LBP. As important additive effects of motor 5 Rackwitz B, de Bie R, Limm H, et al. Seg-
mental stabilizing exercises and low back
little as one session with muscle con- control exercises cannot be excluded. pain, what is the evidence: a systematic
traction practice can alter cortical ex- review of randomized controlled trials.
Clin Rehabil. 2006;20:553–567.
citation49 and cause improvement in
Dr Vasseljen provided concept/idea/ 6 Standaert CJ, Weinstein SM, Rumpeltes J.
deep abdominal muscle onset of activ- research design, fund procurement, facili- Evidence-informed management of chronic
ity.50 Isolated voluntary contractions ties/equipment, and institutional liaisons. low back pain with lumbar stabilization ex-
ercises. Spine J. 2008;8:114 –120.
of the TrA have induced a shift in mo- Mrs Unsgaard-Tøndel and Dr Vasseljen pro-
tor cortical representation of the TrA vided writing and project management. Mrs
October 2010 Volume 90 Number 10 Physical Therapy f 1435
Exercises for Patients With Chronic Low Back Pain
7 Ferreira ML, Ferreira PH, Latimer J, et al. 20 Costa LO, Maher CG, Latimer J, et al. Mo- 35 Baker D, Pynsent PB, Fairbank J. The Oswe-
Comparison of general exercise, motor tor control exercise for chronic low back stry Disability Index revised: its reliability,
control exercise and spinal manipulative pain: a randomized placebo-controlled tri- repeatability and validity, and a comparison
therapy for chronic low back pain: a ran- al. Phys Ther. 2009; 89:1275–1286. with the St Thomas Disability Index. In: Ro-
domized trial. Pain. 2007;131:31–37. land MO Jr, ed. Back Pain. New Approaches
21 Koumantakis GA, Watson PJ, Oldham JA. to Rehabilitation and Education. Manches-
8 Niemisto L, Rissanen P, Sarna S, et al. Cost- Trunk muscle stabilization training plus ter, United Kingdom: Manchester University
effectiveness of combined manipulation, general exercise versus general exercise Press; 1990:175– 181.
stabilizing exercises, and physician consul- only: randomized controlled trial of pa-
tation compared to physician consultation tients with recurrent low back pain. Phys 36 Fairbank JC, Couper J, Davies JB, et al. The
alone for chronic low back pain: a pro- Ther. 2005;85:209 –225. Oswestry Low Back Pain Disability Question-
spective randomized trial with 2-year fol- naire. Physiotherapy. 1980;66:271– 273.
22 Richardson CA, Hodges PW, Hides JA.
low-up. Spine (Phila Pa 1976). 2005;30: Therapeutic Exercise for Lumbopelvic 37 Waddell G, Newton M, Henderson I, et al.
1109 –1115. Stabilization: A Motor Control Approach A Fear-Avoidance Beliefs Questionnaire
9 Descarreaux M, Normand MC, Laurencelle for the Treatment and Prevention of Low (FABQ) and the role of fear-avoidance be-
L, Dugas C. Evaluation of a specific home Back Pain. Edinburgh, Scotland: Churchill liefs in chronic low back pain and disabil-
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
exercise program for low back pain. J Ma- Livingstone; 2004. ity. Pain. 1993;52:157–168.
nipulative Physiol Ther. 2002;25:497–503. 23 Grenier SG, McGill SM. Quantification of 38 Williamson E. Fear-Avoidance Beliefs
10 Marshall PW, Murphy BA. Muscle activa- lumbar stability by using 2 different ab- Questionnaire (FABQ). Aust J Physiother.
tion changes after exercise rehabilitation dominal activation strategies. Arch Phys 2006;52:149.
for chronic low back pain. Arch Phys Med Med Rehabil. 2007;88:54 – 62. 39 Perret C, Poiraudeau S, Fermanian J, et al.
Rehabil. 2008;89:1305–1313. 24 Vera-Garcia FJ, Elvira JL, Brown SH, McGill Validity, reliability, and responsiveness of
11 Frost H, Lamb SE, Klaber Moffett JA, et al. SM. Effects of abdominal stabilization ma- the Fingertip-to-Floor Test. Arch Phys Med
A fitness programme for patients with neuvers on the control of spine motion Rehabil. 2001;82:1566 –1570.
chronic low back pain: 2-year follow-up of and stability against sudden trunk pertur- 40 Ostelo RW, Deyo RA, Stratford P, et al.
a randomised controlled trial. Pain. 1998; bations. J Electromyogr Kinesiol. 2007;17: Interpreting change scores for pain and
75:273–279. 556 –567. functional status in low back pain: to-
12 Hurwitz EL, Morgenstern H, Chiao C. Ef- 25 Childs JD, Piva SR, Fritz JM. Responsive- wards international consensus regarding
fects of recreational physical activity and ness of the numeric pain rating scale in minimal important change. Spine (Phila
back exercises on low back pain and psy- patients with low back pain. Spine (Phila Pa 1976). 2008;33:90 –94.
chological distress: findings from the Pa 1976). 2005;30:1331–1334. 41 Pengel LH, Refshauge KM, Maher CG. Re-
UCLA Low Back Pain Study. Am J Public 26 Liddle SD, Gracey JH, Baxter GD. Advice sponsiveness of pain, disability, and phys-
Health. 2005;95:1817–1824. for the management of low back pain: a ical impairment outcomes in patients with
13 Hodges PW, Richardson CA. Delayed pos- systematic review of randomised con- low back pain. Spine (Phila Pa 1976).
tural contraction of transversus abdominis trolled trials. Man Ther. 2007;12:310 –327. 2004;29:879 – 883.
in low back pain associated with move- 27 Hides JA. Local segmental control. In: 42 Grotle M, Vollestad NK, Veierod MB, Brox
ment of the lower limb. J Spinal Disord. Richardson CA, Hodges P, Hides J, eds. JL. Fear-avoidance beliefs and distress in
1998;11:46 –56. Therapeutic Exercise for Lumbopelvic relation to disability in acute and chronic
14 Hides JA, Stokes MJ, Saide M, et al. Evi- Stabilization. Toronto, Ontario, Canada: low back pain. Pain. 2004;112:343–352.
dence of lumbar multifidus muscle wast- Churchill Livingstone; 1989:202–218. 43 Rainville J, Hartigan C, Martinez E, et al.
ing ipsilateral to symptoms in patients 28 Teyhen DS, Gill NW, Whittaker JL, et al. Exercise as a treatment for chronic low
with acute/subacute low back pain. Spine Rehabilitative ultrasound imaging of the back pain. Spine J. 2004;4:106 –115.
(Phila Pa 1976). 1994;19:165–172. abdominal muscles. J Orthop Sports Phys 44 Braun DA, Aertsen A, Wolpert DM, Mehring
15 Hides JA, Jull GA, Richardson CA. Long- Ther. 2007;37:450 – 466. C. Motor task variation induces structural
term effects of specific stabilizing exer- 29 Whittaker JL. Treatment applications. In: learning. Curr Biol. 2009; 19:352–357.
cises for first-episode low back pain. Whittaker JL, ed. Ultrasound Imaging for
Spine. 2001;26:E243–248. 45 van Vliet PM, Heneghan NR. Motor control
Rehabilitation of the Lumbopelvic Re- and the management of musculoskeletal
16 Hides JA, Richardson CA, Jull GA. Multifi- gion. London, United Kingdom: Churchill dysfunction. Man Ther. 2006;11:208 –213.
dus muscle recovery is not automatic after Livingstone; 2007:120 –140.
resolution of acute, first-episode low back 46 Ljunggren AE, Weber H, Kogstad O, et al.
30 Teyhen DS, Childs JD, Flynn TW. Rehabil-
pain. Spine (Phila Pa 1976). 1996; 21: Effect of exercise on sick leave due to low
itative ultrasound imaging: When is a pic-
2763–2769. back pain: a randomized, comparative,
ture necessary? J Orthop Sports Phys Ther. long-term study. Spine (Phila Pa 1976).
17 O’Sullivan PB, Phyty GD, Twomey LT, Al- 2007;37:579 –580. 1997;22:1610 –1617.
lison GT. Evaluation of specific stabilizing 31 Ljunggren AE, Weber H, Kogstad O, et al.
exercise in the treatment of chronic low 47 Hayden JA, van Tulder MW, Malmivaara
Effect of exercise on sick leave due to low
back pain with radiologic diagnosis of AV, Koes BW. Meta-analysis: exercise ther-
back pain: a randomized, comparative,
spondylolysis or spondylolisthesis. Spine apy for nonspecific low back pain. Ann
long-term study. Spine (Phila Pa 1976).
(Phila Pa 1976). 1997;22:2959 –2967. Intern Med. 2005;142:765–775.
1997;22:1610 –1617.
18 Stuge B, Laerum E, Kirkesola G, Vollestad 48 Hayden JA, van Tulder MW, Tomlinson G.
32 Liddle SD, Baxter GD, Gracey JH. Exercise
N. The efficacy of a treatment program Systematic review: strategies for using ex-
and chronic low back pain: what works
focusing on specific stabilizing exercises ercise therapy to improve outcomes in
[erratum in Pain. 2004;109:200 –201]?
for pelvic girdle pain after pregnancy: a chronic low back pain. Ann Intern Med.
Pain. 2004;107:176 –190.
randomized controlled trial. Spine (Phila 2005;142:776 –785.
Pa 1976). 2004;29:351–359. 33 Jones RE. Reliability of the ten repetition 49 Hayashi S, Hasegawa Y, Kasai T. Transcra-
maximum for assessing progressive resis-
19 Stuge B, Veierod MB, Laerum E, Vollestad nial magnetic stimulation study of plastic
tance exercise. J Am Phys Ther Assoc.
N. The efficacy of a treatment program changes of human motor cortex after re-
1962;42:661– 662.
focusing on specific stabilizing exercises petitive simple muscle contractions. Per-
for pelvic girdle pain after pregnancy: a 34 Andersen LL, Magnusson SP, Nielsen M, cept Mot Skills. 2002;95(3 pt 1):699 –705.
two-year follow-up of a randomized clini- et al. Neuromuscular activation in con-
cal trial. Spine (Phila Pa 1976). 2004;29: ventional therapeutic exercises and
E197–203. heavy resistance exercises: implications
for rehabilitation. Phys Ther. 2006;86:
683– 697.
1436 f Physical Therapy Volume 90 Number 10 October 2010
Exercises for Patients With Chronic Low Back Pain
50 Tsao H, Hodges PW. Immediate changes in 53 Dankaerts W, O’Sullivan P, Burnett A, 56 Kiesel KB, Uhl T, Underwood FB, Nitz
feedforward postural adjustments follow- Straker L. Altered patterns of superficial AJ. Rehabilitative ultrasound measure-
ing voluntary motor training. Exp Brain trunk muscle activation during sitting in ment of select trunk muscle activation
Res. 2007;181:537–546. nonspecific chronic low back pain patients: during induced pain. Man Ther. 2008;
importance of subclassification. Spine 13:132–138.
51 Tsao H, Galea MP, Hodges PW. Driving (Phila Pa 1976). 2006;31:2017–2023.
plasticity in the motor cortex in recurrent 57 Kamper SJ, Maher CG, Hancock MJ, et al.
low back pain. Eur J Pain. February 22, 54 Vibe Fersum K, O’Sullivan PB, Kvale A, Skouen Treatment-based subgroups of low back
2010 [Epub ahead of print]. JS. Inter-examiner reliability of a classification pain: a guide to appraisal of research
system for patients with non-specific low back studies and a summary of current evi-
52 Vasseljen O, Fladmark AM. Abdominal pain. Man Ther. 2009;14:555–561. dence. Best Pract Res Clin Rheumatol.
muscle contraction thickness and function 2010;24:181–191.
after specific and general exercises: a ran- 55 Hodges PW, Moseley GL, Gabrielsson A,
domized controlled trial in chronic low Gandevia SC. Experimental muscle pain
back pain patients. Man Ther. In press. changes feedforward postural responses
of the trunk muscles. Exp Brain Res. 2003;
151:262–271.
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
October 2010 Volume 90 Number 10 Physical Therapy f 1437
Exercises for Patients With Chronic Low Back Pain
Appendix 1.
Sling Exercises: (A) Bilateral Hip Extension With Unilateral Closed Chain, (B) Unilateral Hip Flexion With Contralateral Closed
Chain, and (C) Unilateral Hip Abduction With Contralateral Closed Chain
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
1438 f Physical Therapy Volume 90 Number 10 October 2010
Exercises for Patients With Chronic Low Back Pain
Appendix 2.
Description of Interventions
The motor control and sling exercise interventions are both termed “specific stabilizing exercises” in this article.
Motor Control Exercises
The home exercises, as well as the exercises performed with therapist instruction, were individually adapted, and
the participants who managed to perform an isolated contraction of the transversus abdominis muscle were
instructed to perform co-contractions of deep abdominal and back muscles together with pelvic-floor contractions.
The participants received stretching exercises when considered necessary.
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
Sling Exercises
The sling exercises were based on a treatment method that aims at regaining normal functional movement patterns
in patients with musculoskeletal disorders by using high levels of neuromuscular activation (Kirkesolaa). Body
weight-bearing exercises, gradual increase of resistance (workload), and no pain or increase of existing pain are
central elements. This method includes testing procedures for neuromuscular function of the kinetic chains and the
integration of local and global muscle function. The sling exercises in this study were built upon principles described
in Fysioterapeuten (the Norwegian journal of physical therapy)a but with only manual handling of the slings.
a
Kirkesola G. Neurac: a new treatment method for chronic musculoskeletal pain [abstract in English]. Fysioterapeuten. 2009;76(12):10.
October 2010 Volume 90 Number 10 Physical Therapy f 1439
Exercises for Patients With Chronic Low Back Pain
Appendix 3.
General Exercises: (A) Trunk Extension, (B) Leg Curl, and (C) Arm Extension
Downloaded from https://academic.oup.com/ptj/article/90/10/1426/2737713 by guest on 14 September 2020
1440 f Physical Therapy Volume 90 Number 10 October 2010
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Barry S. Fogel, Donna B. Greenberg-Psychiatric Care of The Medical Patient-Oxford University Press (2015) PDFDocument1,813 pagesBarry S. Fogel, Donna B. Greenberg-Psychiatric Care of The Medical Patient-Oxford University Press (2015) PDFhalamadrid77100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 5 The Knee PDFDocument515 pages5 The Knee PDFjongski100% (2)
- Laboratory Evaluation of Wood and Other Cellulosic Materials For Resistance To TermitesDocument3 pagesLaboratory Evaluation of Wood and Other Cellulosic Materials For Resistance To TermitesAnvit GadkarNo ratings yet
- A Blue Ocean StrategyDocument22 pagesA Blue Ocean StrategyNaru TosNo ratings yet
- Worksheet 25 - 26 - 3rd - MSP - EDocument8 pagesWorksheet 25 - 26 - 3rd - MSP - EMelissaNo ratings yet
- Bengkel Biologi SmartGDocument6 pagesBengkel Biologi SmartGK XuanNo ratings yet
- Lecture 2 The Meanings and Dimensions of Culture NewDocument30 pagesLecture 2 The Meanings and Dimensions of Culture NewKanwal100% (1)
- 8100 Series Fire Pumps: Replacement Parts ForDocument10 pages8100 Series Fire Pumps: Replacement Parts ForAlvialvarezNo ratings yet
- Push Up GuideDocument11 pagesPush Up GuideRafaela NarbaesNo ratings yet
- UASA English Workshop Part 1 - 5Document30 pagesUASA English Workshop Part 1 - 5khomala ruebanNo ratings yet
- 1st Quarter Test in Science With ToS KeyDocument6 pages1st Quarter Test in Science With ToS KeyGizelle R MANo ratings yet
- 2020-07-16 St. Mary's County TimesDocument32 pages2020-07-16 St. Mary's County TimesSouthern Maryland OnlineNo ratings yet
- Non-Catalytic Pyrolysis of Ethane To Ethylene in The Presence of CO2 With or Without Limited O2Document7 pagesNon-Catalytic Pyrolysis of Ethane To Ethylene in The Presence of CO2 With or Without Limited O2Sharry ApudNo ratings yet
- RNA PowerPointDocument20 pagesRNA PowerPointAnki0391100% (1)
- 2.TT Ref620Document21 pages2.TT Ref620Nermina MalićevićNo ratings yet
- Curriculum Vitae: Technical SkillsDocument5 pagesCurriculum Vitae: Technical SkillsIvan StojkovNo ratings yet
- Polymer Materials From Recycled Plastic in Road ConstructionDocument7 pagesPolymer Materials From Recycled Plastic in Road ConstructionYuv RajNo ratings yet
- M CHAT ScoringDocument4 pagesM CHAT ScoringClaritaNo ratings yet
- Emergency Preparedness Audit - GuideDocument20 pagesEmergency Preparedness Audit - GuideMaricris Napigkit SerranoNo ratings yet
- Cell Structure and Organelles: SBI4U-2016/10/14Document16 pagesCell Structure and Organelles: SBI4U-2016/10/14LBJNo ratings yet
- Especificaciones de Valvulas Normas APIDocument2 pagesEspecificaciones de Valvulas Normas APIÀngel Rodriguez0% (1)
- Oxygen MSDSDocument9 pagesOxygen MSDSariNo ratings yet
- Renewable Energy TypesDocument4 pagesRenewable Energy TypesNaufal IhsanNo ratings yet
- Conscientious Objector Info Pack Part 2Document194 pagesConscientious Objector Info Pack Part 2Shot_infoNo ratings yet
- The One Minute ManagerDocument20 pagesThe One Minute ManagerYashwant J100% (2)
- Chew 2021Document22 pagesChew 2021Pedro Hygor100% (1)
- Worried About The Fall in Gold Price?: Ashish Ranawade, Head of Products, Emkay Global. Annexure: Gold Price ChartDocument1 pageWorried About The Fall in Gold Price?: Ashish Ranawade, Head of Products, Emkay Global. Annexure: Gold Price ChartspeedenquiryNo ratings yet
- Olear Ehv GroupDocument16 pagesOlear Ehv GroupSRINIVAS KOMMINENINo ratings yet
- MCCB Catalogue PDFDocument84 pagesMCCB Catalogue PDFSudipta ChatterjeeNo ratings yet
- Paper 1 Micro Economics Extended Response PaperDocument11 pagesPaper 1 Micro Economics Extended Response Paperanonymous100% (1)