
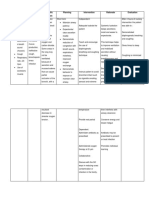
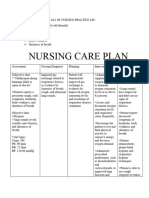
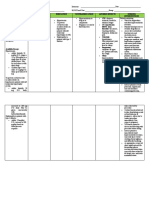
Nursing Care Plan: Cues Nursing Diagnosis Analysis Planning Nursing Interventions Rationale Evaluation
Nursing Care Plan: Cues Nursing Diagnosis Analysis Planning Nursing Interventions Rationale Evaluation
You might also like
- NCP 1 N 2Document5 pagesNCP 1 N 2Cuttie Anne GalangNo ratings yet
- Mindray Wato EX-65 Anaesthesia Machine - Service Manual-2Document50 pagesMindray Wato EX-65 Anaesthesia Machine - Service Manual-2Rene GonzalesNo ratings yet
- Stephen Hobbs - Thoracic Imaging - A Core Review-Lippincott Williams & Wilkins (2015)Document564 pagesStephen Hobbs - Thoracic Imaging - A Core Review-Lippincott Williams & Wilkins (2015)hüseyin vururNo ratings yet
- NCP For Impaired Gas ExchangeDocument2 pagesNCP For Impaired Gas ExchangeSweetie Star94% (16)
- Time Chart: Data Action ResponseDocument2 pagesTime Chart: Data Action ResponseAziil Liiza100% (2)
- Chest Fisioterapy in BronchiektasisDocument11 pagesChest Fisioterapy in BronchiektasisKhalila DiantiNo ratings yet
- NCP EmphysemaDocument9 pagesNCP Emphysemahermesdave188% (8)
- Medsurg QuizDocument11 pagesMedsurg Quizpoleene de leonNo ratings yet
- Chest PDFDocument95 pagesChest PDFsherief maroufNo ratings yet
- NCP Impaired Gas ExchangeDocument4 pagesNCP Impaired Gas ExchangeKen Simon100% (1)
- Nursing Care Plan: Short TermDocument2 pagesNursing Care Plan: Short TermKristine Young100% (1)
- NAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXDocument2 pagesNAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXTyn TynNo ratings yet
- Vital Signs Taken As FollowsDocument10 pagesVital Signs Taken As FollowsKyle AndrewNo ratings yet
- NCP Difficulties in BreathingDocument4 pagesNCP Difficulties in BreathingKingJayson Pacman06No ratings yet
- Case Presentaion Pe (FinalDocument29 pagesCase Presentaion Pe (FinalFatema AkhterNo ratings yet
- NCP DR WardDocument5 pagesNCP DR WardLyza MateoNo ratings yet
- Vi. Nursing Care PlanDocument3 pagesVi. Nursing Care PlanJopaii TanakaNo ratings yet
- NURSING CARE PLAN Alvarez - Impaired Gas ExchangeDocument2 pagesNURSING CARE PLAN Alvarez - Impaired Gas ExchangeNader AbdurasadNo ratings yet
- Assessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveDocument6 pagesAssessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveIngrid Eunice ConcordiaNo ratings yet
- Patient Anita NCPDocument15 pagesPatient Anita NCPJoshoua MalanaNo ratings yet
- NCP 3Document2 pagesNCP 3Krisianne Mae Lorenzo FranciscoNo ratings yet
- Assessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationDocument20 pagesAssessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationKen BaxNo ratings yet
- NCP For Hodgkins DiseaseDocument6 pagesNCP For Hodgkins DiseaseROMER LOZADANo ratings yet
- NCP Acute BrochitisDocument5 pagesNCP Acute BrochitisFrancine kimberlyNo ratings yet
- Emphysema NCPDocument5 pagesEmphysema NCPAbegail Bautista DoriaNo ratings yet
- Icu 2Document9 pagesIcu 2GemilleDaphneAndradaNo ratings yet
- University of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisDocument3 pagesUniversity of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisLyn MhoreNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Assessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationDocument13 pagesAssessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationKen BaxNo ratings yet
- Icu 2Document9 pagesIcu 2GemilleDaphneAndradaNo ratings yet
- NCPDocument3 pagesNCPMichael TokongNo ratings yet
- Archives Review Article 2019Document7 pagesArchives Review Article 2019Harpreet SinghNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- Pulmonary Edema: Topic OutlineDocument2 pagesPulmonary Edema: Topic OutlineKdamnz100% (1)
- Nursing Care Plan (Pedia)Document5 pagesNursing Care Plan (Pedia)JA BerzabalNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationJustine Mae A. LoriaNo ratings yet
- Group 3 FundaDocument2 pagesGroup 3 FundaKyla RamonesNo ratings yet
- Final NCP (Jannel)Document6 pagesFinal NCP (Jannel)Zed P. EstalillaNo ratings yet
- NCP 2Document7 pagesNCP 2Kerks Von Gladiel NapaoNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveDocument3 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveSherlyn KirisakiNo ratings yet
- Assessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoDocument5 pagesAssessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoMaria Francheska OsiNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument4 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal ChoudharyNo ratings yet
- Congestive Cardiac FailureDocument22 pagesCongestive Cardiac FailureSampada GajbhiyeNo ratings yet
- NCP-Drug Study 2Document4 pagesNCP-Drug Study 2hsiriaNo ratings yet
- NCP.2F 2B 1Document5 pagesNCP.2F 2B 1JustineNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care PlanNERISSA CABRIADASNo ratings yet
- Air Gets Inside The Chest CavityDocument2 pagesAir Gets Inside The Chest CavityLore Anne Mhae SantosNo ratings yet
- Date Ordered Date Performed Date Changed or D/C General Description Indications or Purposes Client'S Response TO THE TreatmentDocument13 pagesDate Ordered Date Performed Date Changed or D/C General Description Indications or Purposes Client'S Response TO THE Treatmentjep03No ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument9 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluationclydell joyce masiarNo ratings yet
- Name: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaDocument3 pagesName: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaMae Therese B. MAGNONo ratings yet
- NCP LDocument2 pagesNCP LkasjdkasNo ratings yet
- Careplan 1Document11 pagesCareplan 1ligaba1559No ratings yet
- Nursing Care PlanDocument1 pageNursing Care PlanMikki lor PuaganNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Nursing Care Plan Client: N. D. Age: 39 Gender: Male Medical Diagnosis: Community Acquired Pneumonia, Moderate Risk, PTBDocument24 pagesNursing Care Plan Client: N. D. Age: 39 Gender: Male Medical Diagnosis: Community Acquired Pneumonia, Moderate Risk, PTBGertrude Araneta JavierNo ratings yet
- Nursing Care Plan Assessment Explanation of The Problem Goals and Objectives Intervention Rationale EvaluationDocument10 pagesNursing Care Plan Assessment Explanation of The Problem Goals and Objectives Intervention Rationale EvaluationGuile RilleraNo ratings yet
- Community Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientDocument4 pagesCommunity Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientKrisianne Mae Lorenzo Francisco100% (1)
- Bernardo, Brylle Nicole - NCPDocument1 pageBernardo, Brylle Nicole - NCPChen BernardoNo ratings yet
- COPD Concept MapDocument1 pageCOPD Concept MapSherree HayesNo ratings yet
- Therapeutic AssignmentDocument4 pagesTherapeutic AssignmentSylvester WasongaNo ratings yet
- NCP PTBDocument4 pagesNCP PTBbryan matiasNo ratings yet
- Laguna State Polytechnic UniversityDocument10 pagesLaguna State Polytechnic UniversityKristine Louise JavierNo ratings yet
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- Gec-Art - Art Appreciation: Week 4Document21 pagesGec-Art - Art Appreciation: Week 4poleene de leonNo ratings yet
- NURSING INFORMATICS Review NotesDocument4 pagesNURSING INFORMATICS Review Notespoleene de leonNo ratings yet
- GEC-RVA: Reading Visual Art and Principles of Design: Week 5 LessonDocument31 pagesGEC-RVA: Reading Visual Art and Principles of Design: Week 5 Lessonpoleene de leonNo ratings yet
- WEEK 1 - Concept of CommunityDocument5 pagesWEEK 1 - Concept of Communitypoleene de leonNo ratings yet
- Drug StudyDocument34 pagesDrug Studypoleene de leonNo ratings yet
- Gec ArtDocument25 pagesGec Artpoleene de leonNo ratings yet
- Gec-Art Art Appreciation: Course Code: Course Title: Course DescriptionsDocument14 pagesGec-Art Art Appreciation: Course Code: Course Title: Course Descriptionspoleene de leonNo ratings yet
- Week 2 GEC ARTDocument23 pagesWeek 2 GEC ARTpoleene de leonNo ratings yet
- (26 29) Process Recording FormatDocument4 pages(26 29) Process Recording Formatpoleene de leonNo ratings yet
- Initial Nursing AssessmentDocument2 pagesInitial Nursing Assessmentpoleene de leonNo ratings yet
- Terms NicuDocument1 pageTerms Nicupoleene de leonNo ratings yet
- Nursing NCP 2Document14 pagesNursing NCP 2poleene de leonNo ratings yet
- Nursing NCP 3Document17 pagesNursing NCP 3poleene de leonNo ratings yet
- Drug Study: NCM 106 Pharmacology: Patient MonitoringDocument2 pagesDrug Study: NCM 106 Pharmacology: Patient Monitoringpoleene de leonNo ratings yet
- Nursing Care Plan: Cues Diagnosis Analysis Planning Intervention Rationale EvaluationDocument1 pageNursing Care Plan: Cues Diagnosis Analysis Planning Intervention Rationale Evaluationpoleene de leonNo ratings yet
- Blood Transfusion (During Procedure)Document1 pageBlood Transfusion (During Procedure)poleene de leonNo ratings yet
- Imogene KingDocument1 pageImogene Kingpoleene de leonNo ratings yet
- DISCHARGE PLAN FormatDocument1 pageDISCHARGE PLAN Formatpoleene de leonNo ratings yet
- Chrislelene-AfterBT ReportDocument1 pageChrislelene-AfterBT Reportpoleene de leonNo ratings yet
- Drug Study: NCM 106 PharmacologyDocument2 pagesDrug Study: NCM 106 Pharmacologypoleene de leonNo ratings yet
- Lesson 1: Introduction To Philosophy Material and Formal Object Lesson 2: Philosophy Meaning of PhilosophyDocument3 pagesLesson 1: Introduction To Philosophy Material and Formal Object Lesson 2: Philosophy Meaning of Philosophypoleene de leonNo ratings yet
- Anti Human Embryo What Is Embryo? "An Embryo Is The Early Stage of Human Development in WhichDocument3 pagesAnti Human Embryo What Is Embryo? "An Embryo Is The Early Stage of Human Development in Whichpoleene de leonNo ratings yet
- Procedures After Blood TransfusionDocument1 pageProcedures After Blood Transfusionpoleene de leonNo ratings yet
- NCM 106 Quiz 1Document4 pagesNCM 106 Quiz 1poleene de leonNo ratings yet
- Clonidine Drug StudyDocument7 pagesClonidine Drug Studypoleene de leonNo ratings yet
- Drug Study: NCM 106 PharmacologyDocument2 pagesDrug Study: NCM 106 Pharmacologypoleene de leon100% (1)
- Drug Study: NCM 106 PharmacologyDocument2 pagesDrug Study: NCM 106 Pharmacologypoleene de leonNo ratings yet
- Nursing Care Plan Cord CareDocument3 pagesNursing Care Plan Cord Carepoleene de leonNo ratings yet
- Components of Labor (4 P's in Labor) : Pelvis of The MotherDocument2 pagesComponents of Labor (4 P's in Labor) : Pelvis of The Motherpoleene de leonNo ratings yet
- PHYSICAL-ASSESSMENT EmeDocument3 pagesPHYSICAL-ASSESSMENT EmeBESA JERIC FLORESNo ratings yet
- Thesis Face Mask ReviewDocument7 pagesThesis Face Mask ReviewBuyingCollegePapersBatonRouge100% (1)
- ByssinosisAsbestosis SilicosisDocument44 pagesByssinosisAsbestosis SilicosisMARK ARQUE LACANARIANo ratings yet
- Material Safety Data Sheet: 1. Identification of The Substance/Preparation and The Company/UndertakingDocument4 pagesMaterial Safety Data Sheet: 1. Identification of The Substance/Preparation and The Company/Undertakingtonio28No ratings yet
- Asanas and DiseaseDocument20 pagesAsanas and Diseasesarathy1231No ratings yet
- Equipment: Administering Oxygen by Way of Endotracheal and Tracheostomy Tubes With A T-Piece (Briggs) AdapterDocument2 pagesEquipment: Administering Oxygen by Way of Endotracheal and Tracheostomy Tubes With A T-Piece (Briggs) AdapterIan TuNo ratings yet
- Case Study PneumoniaDocument45 pagesCase Study PneumoniaYashoda Satpute89% (9)
- Session 3 Pathophysiology of COPD and AsthmaDocument40 pagesSession 3 Pathophysiology of COPD and AsthmaOsamaMazhariNo ratings yet
- Material Safety Data Sheet: F108 EZEFLO F108 SurfactantDocument7 pagesMaterial Safety Data Sheet: F108 EZEFLO F108 Surfactantsajad gohariNo ratings yet
- Resorcinol MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesResorcinol MSDS: Section 1: Chemical Product and Company IdentificationDevi Yulian AfdrianaNo ratings yet
- Chest X-Ray - Pulmonary Disease - Bronchiectasis and Cystic FibrosisDocument1 pageChest X-Ray - Pulmonary Disease - Bronchiectasis and Cystic FibrosisNang KhamNo ratings yet
- 2010 CHEST - CURVES Mnemonic Medical Decision Making CapacityDocument7 pages2010 CHEST - CURVES Mnemonic Medical Decision Making CapacityMarcelo Viana PsiquiatraNo ratings yet
- Laporan Faal Respi 2021 - Kenni KenedyDocument25 pagesLaporan Faal Respi 2021 - Kenni Kenedykenni kenedyNo ratings yet
- NCM 112 Lecture NotesDocument5 pagesNCM 112 Lecture NotesSureen RegularNo ratings yet
- Ipa Sterile N msds-1Document5 pagesIpa Sterile N msds-1Nuri Estiana AnggrainiNo ratings yet
- Approach To SOBDocument25 pagesApproach To SOBabdiyare7134No ratings yet
- Emergency Road Accident TrainingDocument53 pagesEmergency Road Accident TrainingSubho SamantaNo ratings yet
- Asthma 1Document33 pagesAsthma 1Dalitso nkhomaNo ratings yet
- Usa Today: Life May Change For Us All'Document28 pagesUsa Today: Life May Change For Us All'Lucia SobralNo ratings yet
- MSDS - Thinner AAADocument8 pagesMSDS - Thinner AAAShafri ArifinNo ratings yet
- PALS Assessment Quiz AnswersDocument3 pagesPALS Assessment Quiz AnswersRea CantoNo ratings yet
- Nursing Documentation MedaDocument2 pagesNursing Documentation MedaRuby JostNo ratings yet
- Asphalt - MC 800 (Superior) - Superior Refining Company, LLC (Husky Energy)Document11 pagesAsphalt - MC 800 (Superior) - Superior Refining Company, LLC (Husky Energy)Lindsey BondNo ratings yet
- UNIVEX MSDS EN (1) Certifikat Za LjepiloDocument8 pagesUNIVEX MSDS EN (1) Certifikat Za LjepiloBojsan IzjelicaNo ratings yet
- Balloon Breathing How To GuideDocument1 pageBalloon Breathing How To GuideAdriatik MetaNo ratings yet
- DOA - I PrevailDocument1 pageDOA - I PrevailalbertmunozNo ratings yet




















































































































Download as docx, pdf, or txt
You might also like
- NCP 1 N 2Document5 pagesNCP 1 N 2Cuttie Anne GalangNo ratings yet
- Mindray Wato EX-65 Anaesthesia Machine - Service Manual-2Document50 pagesMindray Wato EX-65 Anaesthesia Machine - Service Manual-2Rene GonzalesNo ratings yet
- Stephen Hobbs - Thoracic Imaging - A Core Review-Lippincott Williams & Wilkins (2015)Document564 pagesStephen Hobbs - Thoracic Imaging - A Core Review-Lippincott Williams & Wilkins (2015)hüseyin vururNo ratings yet
- NCP For Impaired Gas ExchangeDocument2 pagesNCP For Impaired Gas ExchangeSweetie Star94% (16)
- Time Chart: Data Action ResponseDocument2 pagesTime Chart: Data Action ResponseAziil Liiza100% (2)
- Chest Fisioterapy in BronchiektasisDocument11 pagesChest Fisioterapy in BronchiektasisKhalila DiantiNo ratings yet
- NCP EmphysemaDocument9 pagesNCP Emphysemahermesdave188% (8)
- Medsurg QuizDocument11 pagesMedsurg Quizpoleene de leonNo ratings yet
- Chest PDFDocument95 pagesChest PDFsherief maroufNo ratings yet
- NCP Impaired Gas ExchangeDocument4 pagesNCP Impaired Gas ExchangeKen Simon100% (1)
- Nursing Care Plan: Short TermDocument2 pagesNursing Care Plan: Short TermKristine Young100% (1)
- NAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXDocument2 pagesNAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXTyn TynNo ratings yet
- Vital Signs Taken As FollowsDocument10 pagesVital Signs Taken As FollowsKyle AndrewNo ratings yet
- NCP Difficulties in BreathingDocument4 pagesNCP Difficulties in BreathingKingJayson Pacman06No ratings yet
- Case Presentaion Pe (FinalDocument29 pagesCase Presentaion Pe (FinalFatema AkhterNo ratings yet
- NCP DR WardDocument5 pagesNCP DR WardLyza MateoNo ratings yet
- Vi. Nursing Care PlanDocument3 pagesVi. Nursing Care PlanJopaii TanakaNo ratings yet
- NURSING CARE PLAN Alvarez - Impaired Gas ExchangeDocument2 pagesNURSING CARE PLAN Alvarez - Impaired Gas ExchangeNader AbdurasadNo ratings yet
- Assessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveDocument6 pagesAssessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveIngrid Eunice ConcordiaNo ratings yet
- Patient Anita NCPDocument15 pagesPatient Anita NCPJoshoua MalanaNo ratings yet
- NCP 3Document2 pagesNCP 3Krisianne Mae Lorenzo FranciscoNo ratings yet
- Assessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationDocument20 pagesAssessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationKen BaxNo ratings yet
- NCP For Hodgkins DiseaseDocument6 pagesNCP For Hodgkins DiseaseROMER LOZADANo ratings yet
- NCP Acute BrochitisDocument5 pagesNCP Acute BrochitisFrancine kimberlyNo ratings yet
- Emphysema NCPDocument5 pagesEmphysema NCPAbegail Bautista DoriaNo ratings yet
- Icu 2Document9 pagesIcu 2GemilleDaphneAndradaNo ratings yet
- University of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisDocument3 pagesUniversity of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisLyn MhoreNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Assessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationDocument13 pagesAssessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationKen BaxNo ratings yet
- Icu 2Document9 pagesIcu 2GemilleDaphneAndradaNo ratings yet
- NCPDocument3 pagesNCPMichael TokongNo ratings yet
- Archives Review Article 2019Document7 pagesArchives Review Article 2019Harpreet SinghNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- Pulmonary Edema: Topic OutlineDocument2 pagesPulmonary Edema: Topic OutlineKdamnz100% (1)
- Nursing Care Plan (Pedia)Document5 pagesNursing Care Plan (Pedia)JA BerzabalNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationJustine Mae A. LoriaNo ratings yet
- Group 3 FundaDocument2 pagesGroup 3 FundaKyla RamonesNo ratings yet
- Final NCP (Jannel)Document6 pagesFinal NCP (Jannel)Zed P. EstalillaNo ratings yet
- NCP 2Document7 pagesNCP 2Kerks Von Gladiel NapaoNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveDocument3 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveSherlyn KirisakiNo ratings yet
- Assessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoDocument5 pagesAssessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoMaria Francheska OsiNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument4 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal ChoudharyNo ratings yet
- Congestive Cardiac FailureDocument22 pagesCongestive Cardiac FailureSampada GajbhiyeNo ratings yet
- NCP-Drug Study 2Document4 pagesNCP-Drug Study 2hsiriaNo ratings yet
- NCP.2F 2B 1Document5 pagesNCP.2F 2B 1JustineNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care PlanNERISSA CABRIADASNo ratings yet
- Air Gets Inside The Chest CavityDocument2 pagesAir Gets Inside The Chest CavityLore Anne Mhae SantosNo ratings yet
- Date Ordered Date Performed Date Changed or D/C General Description Indications or Purposes Client'S Response TO THE TreatmentDocument13 pagesDate Ordered Date Performed Date Changed or D/C General Description Indications or Purposes Client'S Response TO THE Treatmentjep03No ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument9 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluationclydell joyce masiarNo ratings yet
- Name: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaDocument3 pagesName: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaMae Therese B. MAGNONo ratings yet
- NCP LDocument2 pagesNCP LkasjdkasNo ratings yet
- Careplan 1Document11 pagesCareplan 1ligaba1559No ratings yet
- Nursing Care PlanDocument1 pageNursing Care PlanMikki lor PuaganNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Nursing Care Plan Client: N. D. Age: 39 Gender: Male Medical Diagnosis: Community Acquired Pneumonia, Moderate Risk, PTBDocument24 pagesNursing Care Plan Client: N. D. Age: 39 Gender: Male Medical Diagnosis: Community Acquired Pneumonia, Moderate Risk, PTBGertrude Araneta JavierNo ratings yet
- Nursing Care Plan Assessment Explanation of The Problem Goals and Objectives Intervention Rationale EvaluationDocument10 pagesNursing Care Plan Assessment Explanation of The Problem Goals and Objectives Intervention Rationale EvaluationGuile RilleraNo ratings yet
- Community Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientDocument4 pagesCommunity Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientKrisianne Mae Lorenzo Francisco100% (1)
- Bernardo, Brylle Nicole - NCPDocument1 pageBernardo, Brylle Nicole - NCPChen BernardoNo ratings yet
- COPD Concept MapDocument1 pageCOPD Concept MapSherree HayesNo ratings yet
- Therapeutic AssignmentDocument4 pagesTherapeutic AssignmentSylvester WasongaNo ratings yet
- NCP PTBDocument4 pagesNCP PTBbryan matiasNo ratings yet
- Laguna State Polytechnic UniversityDocument10 pagesLaguna State Polytechnic UniversityKristine Louise JavierNo ratings yet
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- Gec-Art - Art Appreciation: Week 4Document21 pagesGec-Art - Art Appreciation: Week 4poleene de leonNo ratings yet
- NURSING INFORMATICS Review NotesDocument4 pagesNURSING INFORMATICS Review Notespoleene de leonNo ratings yet
- GEC-RVA: Reading Visual Art and Principles of Design: Week 5 LessonDocument31 pagesGEC-RVA: Reading Visual Art and Principles of Design: Week 5 Lessonpoleene de leonNo ratings yet
- WEEK 1 - Concept of CommunityDocument5 pagesWEEK 1 - Concept of Communitypoleene de leonNo ratings yet
- Drug StudyDocument34 pagesDrug Studypoleene de leonNo ratings yet
- Gec ArtDocument25 pagesGec Artpoleene de leonNo ratings yet
- Gec-Art Art Appreciation: Course Code: Course Title: Course DescriptionsDocument14 pagesGec-Art Art Appreciation: Course Code: Course Title: Course Descriptionspoleene de leonNo ratings yet
- Week 2 GEC ARTDocument23 pagesWeek 2 GEC ARTpoleene de leonNo ratings yet
- (26 29) Process Recording FormatDocument4 pages(26 29) Process Recording Formatpoleene de leonNo ratings yet
- Initial Nursing AssessmentDocument2 pagesInitial Nursing Assessmentpoleene de leonNo ratings yet
- Terms NicuDocument1 pageTerms Nicupoleene de leonNo ratings yet
- Nursing NCP 2Document14 pagesNursing NCP 2poleene de leonNo ratings yet
- Nursing NCP 3Document17 pagesNursing NCP 3poleene de leonNo ratings yet
- Drug Study: NCM 106 Pharmacology: Patient MonitoringDocument2 pagesDrug Study: NCM 106 Pharmacology: Patient Monitoringpoleene de leonNo ratings yet
- Nursing Care Plan: Cues Diagnosis Analysis Planning Intervention Rationale EvaluationDocument1 pageNursing Care Plan: Cues Diagnosis Analysis Planning Intervention Rationale Evaluationpoleene de leonNo ratings yet
- Blood Transfusion (During Procedure)Document1 pageBlood Transfusion (During Procedure)poleene de leonNo ratings yet
- Imogene KingDocument1 pageImogene Kingpoleene de leonNo ratings yet
- DISCHARGE PLAN FormatDocument1 pageDISCHARGE PLAN Formatpoleene de leonNo ratings yet
- Chrislelene-AfterBT ReportDocument1 pageChrislelene-AfterBT Reportpoleene de leonNo ratings yet
- Drug Study: NCM 106 PharmacologyDocument2 pagesDrug Study: NCM 106 Pharmacologypoleene de leonNo ratings yet
- Lesson 1: Introduction To Philosophy Material and Formal Object Lesson 2: Philosophy Meaning of PhilosophyDocument3 pagesLesson 1: Introduction To Philosophy Material and Formal Object Lesson 2: Philosophy Meaning of Philosophypoleene de leonNo ratings yet
- Anti Human Embryo What Is Embryo? "An Embryo Is The Early Stage of Human Development in WhichDocument3 pagesAnti Human Embryo What Is Embryo? "An Embryo Is The Early Stage of Human Development in Whichpoleene de leonNo ratings yet
- Procedures After Blood TransfusionDocument1 pageProcedures After Blood Transfusionpoleene de leonNo ratings yet
- NCM 106 Quiz 1Document4 pagesNCM 106 Quiz 1poleene de leonNo ratings yet
- Clonidine Drug StudyDocument7 pagesClonidine Drug Studypoleene de leonNo ratings yet
- Drug Study: NCM 106 PharmacologyDocument2 pagesDrug Study: NCM 106 Pharmacologypoleene de leon100% (1)
- Drug Study: NCM 106 PharmacologyDocument2 pagesDrug Study: NCM 106 Pharmacologypoleene de leonNo ratings yet
- Nursing Care Plan Cord CareDocument3 pagesNursing Care Plan Cord Carepoleene de leonNo ratings yet
- Components of Labor (4 P's in Labor) : Pelvis of The MotherDocument2 pagesComponents of Labor (4 P's in Labor) : Pelvis of The Motherpoleene de leonNo ratings yet
- PHYSICAL-ASSESSMENT EmeDocument3 pagesPHYSICAL-ASSESSMENT EmeBESA JERIC FLORESNo ratings yet
- Thesis Face Mask ReviewDocument7 pagesThesis Face Mask ReviewBuyingCollegePapersBatonRouge100% (1)
- ByssinosisAsbestosis SilicosisDocument44 pagesByssinosisAsbestosis SilicosisMARK ARQUE LACANARIANo ratings yet
- Material Safety Data Sheet: 1. Identification of The Substance/Preparation and The Company/UndertakingDocument4 pagesMaterial Safety Data Sheet: 1. Identification of The Substance/Preparation and The Company/Undertakingtonio28No ratings yet
- Asanas and DiseaseDocument20 pagesAsanas and Diseasesarathy1231No ratings yet
- Equipment: Administering Oxygen by Way of Endotracheal and Tracheostomy Tubes With A T-Piece (Briggs) AdapterDocument2 pagesEquipment: Administering Oxygen by Way of Endotracheal and Tracheostomy Tubes With A T-Piece (Briggs) AdapterIan TuNo ratings yet
- Case Study PneumoniaDocument45 pagesCase Study PneumoniaYashoda Satpute89% (9)
- Session 3 Pathophysiology of COPD and AsthmaDocument40 pagesSession 3 Pathophysiology of COPD and AsthmaOsamaMazhariNo ratings yet
- Material Safety Data Sheet: F108 EZEFLO F108 SurfactantDocument7 pagesMaterial Safety Data Sheet: F108 EZEFLO F108 Surfactantsajad gohariNo ratings yet
- Resorcinol MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesResorcinol MSDS: Section 1: Chemical Product and Company IdentificationDevi Yulian AfdrianaNo ratings yet
- Chest X-Ray - Pulmonary Disease - Bronchiectasis and Cystic FibrosisDocument1 pageChest X-Ray - Pulmonary Disease - Bronchiectasis and Cystic FibrosisNang KhamNo ratings yet
- 2010 CHEST - CURVES Mnemonic Medical Decision Making CapacityDocument7 pages2010 CHEST - CURVES Mnemonic Medical Decision Making CapacityMarcelo Viana PsiquiatraNo ratings yet
- Laporan Faal Respi 2021 - Kenni KenedyDocument25 pagesLaporan Faal Respi 2021 - Kenni Kenedykenni kenedyNo ratings yet
- NCM 112 Lecture NotesDocument5 pagesNCM 112 Lecture NotesSureen RegularNo ratings yet
- Ipa Sterile N msds-1Document5 pagesIpa Sterile N msds-1Nuri Estiana AnggrainiNo ratings yet
- Approach To SOBDocument25 pagesApproach To SOBabdiyare7134No ratings yet
- Emergency Road Accident TrainingDocument53 pagesEmergency Road Accident TrainingSubho SamantaNo ratings yet
- Asthma 1Document33 pagesAsthma 1Dalitso nkhomaNo ratings yet
- Usa Today: Life May Change For Us All'Document28 pagesUsa Today: Life May Change For Us All'Lucia SobralNo ratings yet
- MSDS - Thinner AAADocument8 pagesMSDS - Thinner AAAShafri ArifinNo ratings yet
- PALS Assessment Quiz AnswersDocument3 pagesPALS Assessment Quiz AnswersRea CantoNo ratings yet
- Nursing Documentation MedaDocument2 pagesNursing Documentation MedaRuby JostNo ratings yet
- Asphalt - MC 800 (Superior) - Superior Refining Company, LLC (Husky Energy)Document11 pagesAsphalt - MC 800 (Superior) - Superior Refining Company, LLC (Husky Energy)Lindsey BondNo ratings yet
- UNIVEX MSDS EN (1) Certifikat Za LjepiloDocument8 pagesUNIVEX MSDS EN (1) Certifikat Za LjepiloBojsan IzjelicaNo ratings yet
- Balloon Breathing How To GuideDocument1 pageBalloon Breathing How To GuideAdriatik MetaNo ratings yet
- DOA - I PrevailDocument1 pageDOA - I PrevailalbertmunozNo ratings yet