Download as pdf or txt
You might also like
- The Shyness Social AncietyDocument138 pagesThe Shyness Social AncietySin Seut92% (12)
- Imagery-Enhanced CBT For Social Anxiety Disorder (PDFDrive)Document298 pagesImagery-Enhanced CBT For Social Anxiety Disorder (PDFDrive)Tátrai Henrietta100% (1)
- Anders - Unknown - A Crash Course in Connection TheoryDocument23 pagesAnders - Unknown - A Crash Course in Connection TheoryPablo StafforiniNo ratings yet
- Out of Bounds Volleyball Club Sponsorship PROPOSAL 2019-2020Document11 pagesOut of Bounds Volleyball Club Sponsorship PROPOSAL 2019-2020Apostle Tarirai ChadebahNo ratings yet
- Let's Talk About Talk! Moving Beyond A Flawed Assumption To Meaningful CommunicationDocument58 pagesLet's Talk About Talk! Moving Beyond A Flawed Assumption To Meaningful CommunicationautismoneNo ratings yet
- Forrest Gump PPPDocument20 pagesForrest Gump PPPm1i2r3e4l5a60% (1)
- Attention Deficit and Learning DisablilesDocument36 pagesAttention Deficit and Learning DisablilesNatearia ThrowerNo ratings yet
- FRQ6PracticeNB KEYDocument1 pageFRQ6PracticeNB KEYAna ChicasNo ratings yet
- AVID Interactive Notebooks and MathematicsDocument22 pagesAVID Interactive Notebooks and MathematicsAna ChicasNo ratings yet
- Dear SelfDocument6 pagesDear Selfeglantina alishollariNo ratings yet
- Henry17 'S Guide To Women: An Integrity-Based Approach To Winning The Approval of 9.5s+Document42 pagesHenry17 'S Guide To Women: An Integrity-Based Approach To Winning The Approval of 9.5s+Adam KozakNo ratings yet
- Applying Social Role Valorization TheoryDocument8 pagesApplying Social Role Valorization Theoryapi-322528455No ratings yet
- YDS Çıkmış Sorular 2020 - EylülDocument18 pagesYDS Çıkmış Sorular 2020 - EylülHasan Cagatay BulutNo ratings yet
- Identification and Treatment of Childhood Stuttering: J. Scott YarussDocument23 pagesIdentification and Treatment of Childhood Stuttering: J. Scott YarussasloocltNo ratings yet
- Learning Disabilities (Final)Document42 pagesLearning Disabilities (Final)darshika.vyas100% (1)
- 2296 Shipon-Blum ElisaDocument96 pages2296 Shipon-Blum Elisadenisse gaboNo ratings yet
- Developmental Psychology (Psy 254) Final Review Session: Clarice Robenalt & Michelle Deklyen January 19. 2015Document62 pagesDevelopmental Psychology (Psy 254) Final Review Session: Clarice Robenalt & Michelle Deklyen January 19. 2015happygrape2No ratings yet
- Manohar Scholastic BackwardnessDocument5 pagesManohar Scholastic Backwardnessapi-228136529No ratings yet
- Apa Itu Masalah PembelajaranDocument59 pagesApa Itu Masalah PembelajaranNazhiff AzizanNo ratings yet
- Students With Deafness and Hearing Loss 1Document30 pagesStudents With Deafness and Hearing Loss 1api-512270694No ratings yet
- Dyslexia PresentationDocument49 pagesDyslexia PresentationEagle gamingNo ratings yet
- Speech and Language: Meeting The Needs of All Children Georgina GosdenDocument27 pagesSpeech and Language: Meeting The Needs of All Children Georgina GosdenholidayaccountNo ratings yet
- Encyclopedia of School Psychology Communication DisordersDocument7 pagesEncyclopedia of School Psychology Communication DisordersMohamed BelhadefNo ratings yet
- Cammy Report, Ed7Document19 pagesCammy Report, Ed7Cammy Ethanei Hugo AribNo ratings yet
- Day One Moving Forward With DyslexiaDocument35 pagesDay One Moving Forward With DyslexiajeavilaNo ratings yet
- Changes in dsm5Document24 pagesChanges in dsm5hayaNo ratings yet
- F.5 Selective Mutism Powerpoint 2016Document32 pagesF.5 Selective Mutism Powerpoint 2016Ptrc Lbr LpNo ratings yet
- Selective Mutism For School Psychs and SLPs April 2024Document31 pagesSelective Mutism For School Psychs and SLPs April 2024KerriNo ratings yet
- LoralinDocument22 pagesLoralinapi-272661253No ratings yet
- Lang, Cul and IdentityDocument17 pagesLang, Cul and IdentityM MNo ratings yet
- PSYC0022 Dyslexia 2022Document41 pagesPSYC0022 Dyslexia 2022Yan Yiu Rachel ChanNo ratings yet
- Early Education 2021T1 - UNDYC - L5 - EMI MoodleDocument21 pagesEarly Education 2021T1 - UNDYC - L5 - EMI Moodleiamrockrock7407No ratings yet
- 3 5326 Characteristics Matrix - InputDocument6 pages3 5326 Characteristics Matrix - Inputapi-313154885No ratings yet
- Local Media7324198132320898389Document20 pagesLocal Media7324198132320898389ere chanNo ratings yet
- Learning DisabilitiesDocument32 pagesLearning DisabilitiesGul E RanaNo ratings yet
- Communication DisorderDocument18 pagesCommunication DisorderSamuelNo ratings yet
- English Language Teaching Methodology (Psychosocial)Document12 pagesEnglish Language Teaching Methodology (Psychosocial)Kucing HensemNo ratings yet
- SPED (Finals)Document23 pagesSPED (Finals)jed.berdosNo ratings yet
- SPED (Midterms)Document12 pagesSPED (Midterms)jed.berdosNo ratings yet
- Educ 101 - M3 & M4 Language DevelopmentDocument51 pagesEduc 101 - M3 & M4 Language DevelopmentHannah Esey Aquino PaquinNo ratings yet
- Dyslexia BookletDocument18 pagesDyslexia BookletMelissa MartinezNo ratings yet
- Assessing Language Pragmatics: Who, What and How: Peter A. de Villiers Jill G. de Villiers Smith CollegeDocument75 pagesAssessing Language Pragmatics: Who, What and How: Peter A. de Villiers Jill G. de Villiers Smith Collegeahmed4dodiNo ratings yet
- CHAPTER 5 - Learning Differences and Learning NeedsDocument50 pagesCHAPTER 5 - Learning Differences and Learning Needsnfathonah2100% (1)
- Chapter 4 (Woolfolk) Learner Differences Adn Learning Needs - Anindya YuniarDocument37 pagesChapter 4 (Woolfolk) Learner Differences Adn Learning Needs - Anindya YuniarAnindya YuniarNo ratings yet
- Workshop With Teachers KPISDocument16 pagesWorkshop With Teachers KPISMitali BarotNo ratings yet
- Selective Mutism:: Assessment and InterventionDocument13 pagesSelective Mutism:: Assessment and InterventionIbtisam Marohombsar AlontoNo ratings yet
- Speechdelayravi 180410141626Document32 pagesSpeechdelayravi 180410141626GuruNo ratings yet
- GROUP 2 - Learning DisabilitiesDocument20 pagesGROUP 2 - Learning DisabilitieserikhaiboreresNo ratings yet
- Social-Emotional Outcomes For Children With SLI: A Newsletter Dedicated To Speech & Language in School-Age ChildrenDocument5 pagesSocial-Emotional Outcomes For Children With SLI: A Newsletter Dedicated To Speech & Language in School-Age ChildrenPaul AsturbiarisNo ratings yet
- Beyond Med MGMT UCSD FellowsDocument91 pagesBeyond Med MGMT UCSD FellowscirclestretchNo ratings yet
- Mental Retardation: of AgeDocument8 pagesMental Retardation: of AgeMaria Krzandra OngNo ratings yet
- PSYC0022 Dyslexia 2023Document41 pagesPSYC0022 Dyslexia 2023Yan Yiu Rachel ChanNo ratings yet
- Community Paeds, Language-SKermondDocument50 pagesCommunity Paeds, Language-SKermondUsamah HussainNo ratings yet
- AutismDocument11 pagesAutismAditi MangalNo ratings yet
- Child and AdolescentDocument89 pagesChild and AdolescentLarry CalivoNo ratings yet
- Child and Adolecent ReportDocument12 pagesChild and Adolecent ReportMaryGraceVelascoFuentesNo ratings yet
- Lecture 11 Cognitive Develoopment 1 06122023 084128amDocument29 pagesLecture 11 Cognitive Develoopment 1 06122023 084128amgdppilot123No ratings yet
- ELD 211 - Lecture 2 - 20-02-2023Document14 pagesELD 211 - Lecture 2 - 20-02-2023bradeylinders110No ratings yet
- Language Development: DR Sue KermondDocument45 pagesLanguage Development: DR Sue KermondUsamah HussainNo ratings yet
- Supporting Students with Communication Disorders. A Collaborative Approach: A Resource for Speech-Language Pathologists, Parents and EducatorsFrom EverandSupporting Students with Communication Disorders. A Collaborative Approach: A Resource for Speech-Language Pathologists, Parents and EducatorsNo ratings yet
- ACTIVITY 3 (Eced 6) (Tamayo, Julia)Document20 pagesACTIVITY 3 (Eced 6) (Tamayo, Julia)Julia TamayoNo ratings yet
- Common Childhood Mental Health DisordersDocument42 pagesCommon Childhood Mental Health DisordersMsm BeihoNo ratings yet
- 7 Critical Period - 2024Document33 pages7 Critical Period - 2024Grace LiNo ratings yet
- Normal Non - Fluency, Primary Stuttering and Secondary StutteringDocument21 pagesNormal Non - Fluency, Primary Stuttering and Secondary StutteringK PNo ratings yet
- Speech TherapyDocument10 pagesSpeech TherapyMhay Anne PerezNo ratings yet
- Abnormal Cognitive DevelopmentDocument12 pagesAbnormal Cognitive DevelopmentMikefijiNo ratings yet
- Getting Your Needs Met As A Student With Asperger's DisorderDocument2 pagesGetting Your Needs Met As A Student With Asperger's DisorderAnonymous Pj6OdjNo ratings yet
- AutismDocument2 pagesAutismapi-314847014No ratings yet
- Learning Disabilities: By: Fiona Bridges, Shante Walker, John Hunter, Amanda SpencerDocument13 pagesLearning Disabilities: By: Fiona Bridges, Shante Walker, John Hunter, Amanda Spencerapi-480715417No ratings yet
- Dyslexia - Tanvi Hingankar, Dr. Nilesh RathiDocument50 pagesDyslexia - Tanvi Hingankar, Dr. Nilesh RathiDr. Tanvi HingankarNo ratings yet
- Prep and Admin SummaryDocument3 pagesPrep and Admin SummaryAna ChicasNo ratings yet
- UDLLookForsHandoutwithChartDocument2 pagesUDLLookForsHandoutwithChartAna ChicasNo ratings yet
- Standing OrdersDocument3 pagesStanding OrdersAna ChicasNo ratings yet
- Notification of Exposure Guide FinalDocument25 pagesNotification of Exposure Guide FinalAna ChicasNo ratings yet
- DreamsDocument3 pagesDreamsAna ChicasNo ratings yet
- Everything You (Might) Need For Know For DevelopmentDocument2 pagesEverything You (Might) Need For Know For DevelopmentAna ChicasNo ratings yet
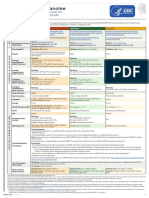
- Covid19 Vaccine Quick Reference Guide PosterDocument1 pageCovid19 Vaccine Quick Reference Guide PosterAna ChicasNo ratings yet
- Statistics Gymnastics WorksheetDocument2 pagesStatistics Gymnastics WorksheetAna ChicasNo ratings yet
- Dream AnalysisDocument1 pageDream AnalysisAna ChicasNo ratings yet
- Operant Conditioning PracticeDocument2 pagesOperant Conditioning PracticeAna ChicasNo ratings yet
- Jenga Questions - LearningDocument6 pagesJenga Questions - LearningAna ChicasNo ratings yet
- AP Psychology Name - Unit V: States of Consciousness Per.Document2 pagesAP Psychology Name - Unit V: States of Consciousness Per.Ana ChicasNo ratings yet
- The Mammalian Brain Starts Eating ItselfDocument1 pageThe Mammalian Brain Starts Eating ItselfAna ChicasNo ratings yet
- Support Materials PDFDocument18 pagesSupport Materials PDFAna ChicasNo ratings yet
- Sensation: Your Window To The World Perception: Interpreting What Comes in Your WindowDocument26 pagesSensation: Your Window To The World Perception: Interpreting What Comes in Your WindowAna ChicasNo ratings yet
- Principles of Learning Visual ReviewDocument2 pagesPrinciples of Learning Visual ReviewAna ChicasNo ratings yet
- PFA SchoolCrisis PDFDocument16 pagesPFA SchoolCrisis PDFAna ChicasNo ratings yet
- Unit Six - FRQ PracticeDocument2 pagesUnit Six - FRQ PracticeAna ChicasNo ratings yet
- The Broken DreamDocument37 pagesThe Broken DreamAna ChicasNo ratings yet
- Flowchart of Training TechniquesDocument1 pageFlowchart of Training TechniquesAna ChicasNo ratings yet
- Flowchart of Schedules of ReinforcementDocument1 pageFlowchart of Schedules of ReinforcementAna ChicasNo ratings yet
- Adele Diamond Close Interrelation of Motor Development and Cognitive Development Cerebellum and Prefrontal CortexDocument14 pagesAdele Diamond Close Interrelation of Motor Development and Cognitive Development Cerebellum and Prefrontal CortexAna ChicasNo ratings yet
- PsychFirstAidSchools PDFDocument186 pagesPsychFirstAidSchools PDFAna ChicasNo ratings yet
- Algebra 2 Summer Student Enrichment PacketDocument26 pagesAlgebra 2 Summer Student Enrichment PacketAna ChicasNo ratings yet
- Cesario Johnson Eisthen IN PRESS CDPS Your Brain Is Not An OnionDocument24 pagesCesario Johnson Eisthen IN PRESS CDPS Your Brain Is Not An OnionAna ChicasNo ratings yet
- Optional Break Packet Parent Letter-EnglishDocument3 pagesOptional Break Packet Parent Letter-EnglishAna ChicasNo ratings yet
- Algebra I Summer Student Enrichment PacketDocument15 pagesAlgebra I Summer Student Enrichment PacketAna ChicasNo ratings yet
- Chapter 2 - Personality, Attitudes, and Work BehaviorsDocument6 pagesChapter 2 - Personality, Attitudes, and Work BehaviorsJUN GERONANo ratings yet
- Thesis Group 5 10aDocument85 pagesThesis Group 5 10aWilky BelmesNo ratings yet
- Big Five Personality TraitsDocument39 pagesBig Five Personality TraitsndmudhosiNo ratings yet
- Revista Latinoamericana de Psicología 0120-0534: Issn: Direccion - Rlp@konradlorenz - Edu.coDocument19 pagesRevista Latinoamericana de Psicología 0120-0534: Issn: Direccion - Rlp@konradlorenz - Edu.coMelina ZapataNo ratings yet
- The Peasant and His BodyDocument22 pagesThe Peasant and His BodyJ CooperNo ratings yet
- Chapter Ii - 2018966pbiDocument20 pagesChapter Ii - 2018966pbiRena SeiNo ratings yet
- Truity BigFiveReportDocument14 pagesTruity BigFiveReportDusanNo ratings yet
- Matura - Reading Comprehension (PRV Jazik)Document5 pagesMatura - Reading Comprehension (PRV Jazik)Emilija PavlovaNo ratings yet
- LedesmaIsabelFaith - Health Care Plan For The PreschoolerDocument9 pagesLedesmaIsabelFaith - Health Care Plan For The Preschoolerxxarrowloverzxxdes23No ratings yet
- Behavior Guidance For The Pediatric Dental Patient: Latest RevisionDocument19 pagesBehavior Guidance For The Pediatric Dental Patient: Latest RevisionJonathan Delgadillo VillarroelNo ratings yet
- CHAPTER 2 Update 2Document4 pagesCHAPTER 2 Update 2yana suriaNo ratings yet
- Theory SpeakingDocument22 pagesTheory SpeakingAjeng Aulia RezQitaaNo ratings yet
- Factors Affecting The Confidence of Grade 7 Students in University of La Salette High School in Speaking EnglishDocument15 pagesFactors Affecting The Confidence of Grade 7 Students in University of La Salette High School in Speaking EnglishDick Jefferson Ocampo PatingNo ratings yet
- Cause Effect EssayDocument17 pagesCause Effect EssayLe Thi Nhu Quynh0% (1)
- Unit - 3 NotesDocument23 pagesUnit - 3 NotesPřàñíťh KümâřNo ratings yet
- QUOTESDocument3 pagesQUOTESFuck YouNo ratings yet
- Musical Achievement and The Self-ConceptDocument9 pagesMusical Achievement and The Self-ConceptInês SacaduraNo ratings yet
- 19.12.23 Final Final Final Final Final ThesisDocument80 pages19.12.23 Final Final Final Final Final ThesisNguyễn Mai HươngNo ratings yet
- Recognizing Young Children's Expressive Styles of Emotions (2-6 YearsDocument8 pagesRecognizing Young Children's Expressive Styles of Emotions (2-6 YearsTrianaNo ratings yet
- Advocating For Shy Students1Document1 pageAdvocating For Shy Students1api-434808297No ratings yet
- Body Image and Self Esteem Among Isra' University StudentsDocument9 pagesBody Image and Self Esteem Among Isra' University Studentssia ruhelaNo ratings yet
- The Bold and The BashfulDocument12 pagesThe Bold and The BashfulHestia StatNo ratings yet