
The Roles of Occupational Therapy, Physical Therapy, and Speech/Language Pathology in Primary Care
The Roles of Occupational Therapy, Physical Therapy, and Speech/Language Pathology in Primary Care
You might also like
- Occupational Therapy Practice Framework: Domain and Process Fourth Edition (2020)Document87 pagesOccupational Therapy Practice Framework: Domain and Process Fourth Edition (2020)Susana Ahumada100% (1)
- Health Career Internet Scavenger Hunt STUDENT FILLABLE PDF 9 - 4 - 2020Document2 pagesHealth Career Internet Scavenger Hunt STUDENT FILLABLE PDF 9 - 4 - 2020Logan Richardson42% (12)
- 2015-01-01 Norms For The Health Cadre - Sri LankaDocument83 pages2015-01-01 Norms For The Health Cadre - Sri LankaDoctors News86% (7)
- Geriatric Health Care Team Autosaved 1Document68 pagesGeriatric Health Care Team Autosaved 1Rose Antonette Benito0% (1)
- Efficacy of Myofascial ReleaseDocument64 pagesEfficacy of Myofascial ReleaseJéssica ByronNo ratings yet
- Evidence-Based Practice in Pediatric Physical Therapy by BarryDocument14 pagesEvidence-Based Practice in Pediatric Physical Therapy by BarryFe Tus100% (1)
- Cognitive Remediation Therapy For Anorexia Nervosa Kate TchanturaDocument156 pagesCognitive Remediation Therapy For Anorexia Nervosa Kate TchanturaIndriNo ratings yet
- Conceptual Foundations of Occupational Therapy 4th EditionDocument332 pagesConceptual Foundations of Occupational Therapy 4th Editionxprakash50% (2)
- PAPER WORKPaediatricsDocument22 pagesPAPER WORKPaediatricsIzzati OthmanNo ratings yet
- Problem and It'S Background: Senior Centers Are AnDocument44 pagesProblem and It'S Background: Senior Centers Are Anrosencrantz_05No ratings yet
- TeamworkDocument37 pagesTeamworkNurnadia OmerNo ratings yet
- Ot 1Document4 pagesOt 1secret101No ratings yet
- Caring For Older People With Dementia: Clinical FocusDocument4 pagesCaring For Older People With Dementia: Clinical FocusOluwakemmieOlamideNo ratings yet
- Community Paediatrics 2015Document4 pagesCommunity Paediatrics 2015Sudhir PaulNo ratings yet
- Research Paper Topics Related To Occupational TherapyDocument8 pagesResearch Paper Topics Related To Occupational Therapykkxtkqund100% (1)
- Post Partum DepressionDocument17 pagesPost Partum Depressionrisda aulia putriNo ratings yet
- Diagnosis and Treatment Planning For Implant-Supported Fixed ProsthesisDocument6 pagesDiagnosis and Treatment Planning For Implant-Supported Fixed ProsthesisJANINE PASIONNo ratings yet
- Research Paper Occupational TherapyDocument8 pagesResearch Paper Occupational Therapygz8reqdc100% (1)
- Presented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical TherapyDocument27 pagesPresented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical Therapysaba ramzanNo ratings yet
- CognitiveDocument19 pagesCognitiveLaila MajenumNo ratings yet
- Dementia CareDocument23 pagesDementia Careprajc100% (1)
- Nursing Care PlanDocument16 pagesNursing Care PlanJennifer Post100% (3)
- Physical Therapy Clinical ManagementDocument24 pagesPhysical Therapy Clinical ManagementClaudia MicuNo ratings yet
- Physical Therapy Clinical Management.9 PDFDocument24 pagesPhysical Therapy Clinical Management.9 PDFClaudia MicuNo ratings yet
- NEUK 1464 (Revised) 1 (Updated)Document21 pagesNEUK 1464 (Revised) 1 (Updated)Sameen ShafaatNo ratings yet
- Cahpter 1 Health Care Professional: MasrulDocument7 pagesCahpter 1 Health Care Professional: Masrulvera syahrinisyaNo ratings yet
- Cognitive Impairment Evaluation and ManagementDocument19 pagesCognitive Impairment Evaluation and ManagementSAMUEL MARIN FUQUENENo ratings yet
- Palliative Care in Nephrology: The Work and The Workforce: Table 1Document7 pagesPalliative Care in Nephrology: The Work and The Workforce: Table 1Kev Jose Ruiz RojasNo ratings yet
- Occupational Therapist Career Research PaperDocument7 pagesOccupational Therapist Career Research Papernjxkgnwhf100% (1)
- OCCUP1Document6 pagesOCCUP1MartinNo ratings yet
- BibliopocDocument4 pagesBibliopocKarlo ReyesNo ratings yet
- Geriatric Nursing: Ma - Alicia Grace S. Kaimo, RN, ManDocument15 pagesGeriatric Nursing: Ma - Alicia Grace S. Kaimo, RN, ManYongNo ratings yet
- Practice GuidelineDocument3 pagesPractice Guidelineclarajimena25No ratings yet
- Final ProjectDocument2 pagesFinal Projectapi-293082830No ratings yet
- Therapeutic Interventions in Cerebral Palsy: Dilip R. PatelDocument5 pagesTherapeutic Interventions in Cerebral Palsy: Dilip R. PatelclikgoNo ratings yet
- NursepractitionerDocument4 pagesNursepractitionerapi-399029638No ratings yet
- Becoming A PTADocument4 pagesBecoming A PTAKrisha Mabel TabijeNo ratings yet
- Interviewing and Counseling The Dizzy Patient With Focus On Quality of LifeDocument9 pagesInterviewing and Counseling The Dizzy Patient With Focus On Quality of LifeCribea AdmNo ratings yet
- GERIATRICE HEALTH CARE TEAM-FinalDocument6 pagesGERIATRICE HEALTH CARE TEAM-Finalcamile buhangin100% (2)
- Clinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentDocument18 pagesClinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentΜαρία ΧανιωτάκηNo ratings yet
- For People With: Ractical Ral Are Developmental DisabilitiesDocument8 pagesFor People With: Ractical Ral Are Developmental DisabilitiesCristian AlberoniNo ratings yet
- Specialty Care Program AutismDocument8 pagesSpecialty Care Program AutismElian Y. Sanchez-RiveraNo ratings yet
- Geriatricrehabilitation: Gait in The Elderly, Fall Prevention and Parkinson DiseaseDocument17 pagesGeriatricrehabilitation: Gait in The Elderly, Fall Prevention and Parkinson DiseaseSandra Milena Cortes SotoNo ratings yet
- Health Team: Prepared By: Mr. J.C. FrankDocument27 pagesHealth Team: Prepared By: Mr. J.C. FrankHardeep KaurNo ratings yet
- OT For CPDocument15 pagesOT For CPYusrina RahmaNo ratings yet
- Cognitive Impairment EvaluationDocument20 pagesCognitive Impairment Evaluationdiana librerosNo ratings yet
- Other Health StaffDocument11 pagesOther Health StaffShanthal MercedesNo ratings yet
- Butler Darrah 2001Document13 pagesButler Darrah 2001Adnan Faris NaufalNo ratings yet
- Complementario 1Document8 pagesComplementario 1Camila OpazoNo ratings yet
- Health TeamDocument5 pagesHealth TeamFahim AhmedNo ratings yet
- 1.1, 1.2, 1.3, 1.5 Paediatric Nursing Presentation - 1-1Document54 pages1.1, 1.2, 1.3, 1.5 Paediatric Nursing Presentation - 1-1Christina YounasNo ratings yet
- Practical Oral Care For People With Autism 2012Document6 pagesPractical Oral Care For People With Autism 2012Amanda AmaroNo ratings yet
- N207 Theory Analysis and EvaluationDocument8 pagesN207 Theory Analysis and Evaluationpfprn100% (1)
- Geriatric Care TeamDocument29 pagesGeriatric Care TeamMarianne Joyce ManzoNo ratings yet
- DBT in ASDDocument9 pagesDBT in ASDCarregan AlvarezNo ratings yet
- OT Process and The 4 Levels of InterventionDocument3 pagesOT Process and The 4 Levels of InterventionMuhammad MukhlisNo ratings yet
- Module 5Document8 pagesModule 5tithi royNo ratings yet
- Unit 11. Advocacy Programs Relevant To The Care of OlderDocument13 pagesUnit 11. Advocacy Programs Relevant To The Care of OlderRichmon Joseph SantosNo ratings yet
- Therapeutic Interventions in The Treatment of Dissociative DisordersDocument18 pagesTherapeutic Interventions in The Treatment of Dissociative DisordersCarla MesquitaNo ratings yet
- Parchem 2018 A Multidisciplinary Approach To Equipment Use in Pediatric Patient Mobilization.Document10 pagesParchem 2018 A Multidisciplinary Approach To Equipment Use in Pediatric Patient Mobilization.Evelyn_D_az_Ha_8434No ratings yet
- Running Head: (GAGTAN, ANDREI RAPHAEL, L.)Document8 pagesRunning Head: (GAGTAN, ANDREI RAPHAEL, L.)Edmarkmoises ValdezNo ratings yet
- 200-CQDN-666574-ND - Job Description and Person SpecificationDocument6 pages200-CQDN-666574-ND - Job Description and Person Specificationsachin_sawant1985No ratings yet
- DocumentDocument11 pagesDocumentVvjjgxgjjNo ratings yet
- Nursing_Profile_2018Document22 pagesNursing_Profile_2018todotonteriasNo ratings yet
- Student Notes Professional Reasoning Na 2023Document39 pagesStudent Notes Professional Reasoning Na 2023mkhal700No ratings yet
- OtizmchapterDocument46 pagesOtizmchaptergokulraja850No ratings yet
- Almaz Mamaru Counseling Psychologist (BA, MA) Department of Psychiatry, Bahardar UniversityDocument39 pagesAlmaz Mamaru Counseling Psychologist (BA, MA) Department of Psychiatry, Bahardar UniversityAklile TsegaNo ratings yet
- 5f7c606e8ca92 - 11 Physical Education English Medium Chapter 4Document9 pages5f7c606e8ca92 - 11 Physical Education English Medium Chapter 4Practically UselessNo ratings yet
- The Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityDocument7 pagesThe Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityIJAR JOURNALNo ratings yet
- Lily Grebe Resume 10Document3 pagesLily Grebe Resume 10api-482765948No ratings yet
- UntitledDocument98 pagesUntitledixixNo ratings yet
- OCP 100 Course SyllabusDocument6 pagesOCP 100 Course SyllabusMegat LokmanNo ratings yet
- Training and Practice in Horticultural TherapyDocument149 pagesTraining and Practice in Horticultural TherapyKritikou1547No ratings yet
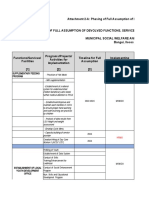
- MSWDO Capdev Form G1 FINALDocument50 pagesMSWDO Capdev Form G1 FINALbai yhang de la cruz100% (1)
- Occupational Problems and Barriers Reported by Individuals With ObesityDocument10 pagesOccupational Problems and Barriers Reported by Individuals With ObesityGraciela SeveriniNo ratings yet
- Sarah (Yosra) Azzam: EducationDocument3 pagesSarah (Yosra) Azzam: Educationapi-505318564No ratings yet
- ShannonjoyceresumeDocument2 pagesShannonjoyceresumeapi-303566481No ratings yet
- Curriculum Vita 2-3-16Document5 pagesCurriculum Vita 2-3-16api-308459832No ratings yet
- OT in Foster Care TransitionDocument10 pagesOT in Foster Care Transitionnoah87No ratings yet
- Occupational TherapyDocument2 pagesOccupational Therapyleen00170% (1)
- 23-05-2018 011346916 - Intervention Modalities - Chapter 16Document26 pages23-05-2018 011346916 - Intervention Modalities - Chapter 16Bisan RatuishNo ratings yet
- Hoppe and Matthews Cat Poster1Document1 pageHoppe and Matthews Cat Poster1api-238169773No ratings yet
- Suggestionfinal-OT Validation DocumentDocument91 pagesSuggestionfinal-OT Validation DocumentAdonis GaleosNo ratings yet
- Unit 1. Changing Trends & Career in Physical Education - Class-11Document6 pagesUnit 1. Changing Trends & Career in Physical Education - Class-11money d luffyNo ratings yet
- Occupational Therapy Dissertation Literature ReviewDocument4 pagesOccupational Therapy Dissertation Literature ReviewPsychologyPaperWritingServiceUKNo ratings yet
- Tic Poster FinalDocument1 pageTic Poster Finalapi-337168518No ratings yet
- Occupational Therapy: SATHISH Rajamani. M.SC (N) Lecturer AmconDocument20 pagesOccupational Therapy: SATHISH Rajamani. M.SC (N) Lecturer AmconSathish RajamaniNo ratings yet
- Chapter 4 F2fDocument28 pagesChapter 4 F2fManisha TidkeNo ratings yet
- An Occupational Perspective On Leadership, Theoratical and Practical Dimentions, 3e Sandra Dunbar-Smalley, Kristin WinstonDocument32 pagesAn Occupational Perspective On Leadership, Theoratical and Practical Dimentions, 3e Sandra Dunbar-Smalley, Kristin WinstonDing Bo50% (2)























































































Download as pdf or txt
You might also like
- Occupational Therapy Practice Framework: Domain and Process Fourth Edition (2020)Document87 pagesOccupational Therapy Practice Framework: Domain and Process Fourth Edition (2020)Susana Ahumada100% (1)
- Health Career Internet Scavenger Hunt STUDENT FILLABLE PDF 9 - 4 - 2020Document2 pagesHealth Career Internet Scavenger Hunt STUDENT FILLABLE PDF 9 - 4 - 2020Logan Richardson42% (12)
- 2015-01-01 Norms For The Health Cadre - Sri LankaDocument83 pages2015-01-01 Norms For The Health Cadre - Sri LankaDoctors News86% (7)
- Geriatric Health Care Team Autosaved 1Document68 pagesGeriatric Health Care Team Autosaved 1Rose Antonette Benito0% (1)
- Efficacy of Myofascial ReleaseDocument64 pagesEfficacy of Myofascial ReleaseJéssica ByronNo ratings yet
- Evidence-Based Practice in Pediatric Physical Therapy by BarryDocument14 pagesEvidence-Based Practice in Pediatric Physical Therapy by BarryFe Tus100% (1)
- Cognitive Remediation Therapy For Anorexia Nervosa Kate TchanturaDocument156 pagesCognitive Remediation Therapy For Anorexia Nervosa Kate TchanturaIndriNo ratings yet
- Conceptual Foundations of Occupational Therapy 4th EditionDocument332 pagesConceptual Foundations of Occupational Therapy 4th Editionxprakash50% (2)
- PAPER WORKPaediatricsDocument22 pagesPAPER WORKPaediatricsIzzati OthmanNo ratings yet
- Problem and It'S Background: Senior Centers Are AnDocument44 pagesProblem and It'S Background: Senior Centers Are Anrosencrantz_05No ratings yet
- TeamworkDocument37 pagesTeamworkNurnadia OmerNo ratings yet
- Ot 1Document4 pagesOt 1secret101No ratings yet
- Caring For Older People With Dementia: Clinical FocusDocument4 pagesCaring For Older People With Dementia: Clinical FocusOluwakemmieOlamideNo ratings yet
- Community Paediatrics 2015Document4 pagesCommunity Paediatrics 2015Sudhir PaulNo ratings yet
- Research Paper Topics Related To Occupational TherapyDocument8 pagesResearch Paper Topics Related To Occupational Therapykkxtkqund100% (1)
- Post Partum DepressionDocument17 pagesPost Partum Depressionrisda aulia putriNo ratings yet
- Diagnosis and Treatment Planning For Implant-Supported Fixed ProsthesisDocument6 pagesDiagnosis and Treatment Planning For Implant-Supported Fixed ProsthesisJANINE PASIONNo ratings yet
- Research Paper Occupational TherapyDocument8 pagesResearch Paper Occupational Therapygz8reqdc100% (1)
- Presented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical TherapyDocument27 pagesPresented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical Therapysaba ramzanNo ratings yet
- CognitiveDocument19 pagesCognitiveLaila MajenumNo ratings yet
- Dementia CareDocument23 pagesDementia Careprajc100% (1)
- Nursing Care PlanDocument16 pagesNursing Care PlanJennifer Post100% (3)
- Physical Therapy Clinical ManagementDocument24 pagesPhysical Therapy Clinical ManagementClaudia MicuNo ratings yet
- Physical Therapy Clinical Management.9 PDFDocument24 pagesPhysical Therapy Clinical Management.9 PDFClaudia MicuNo ratings yet
- NEUK 1464 (Revised) 1 (Updated)Document21 pagesNEUK 1464 (Revised) 1 (Updated)Sameen ShafaatNo ratings yet
- Cahpter 1 Health Care Professional: MasrulDocument7 pagesCahpter 1 Health Care Professional: Masrulvera syahrinisyaNo ratings yet
- Cognitive Impairment Evaluation and ManagementDocument19 pagesCognitive Impairment Evaluation and ManagementSAMUEL MARIN FUQUENENo ratings yet
- Palliative Care in Nephrology: The Work and The Workforce: Table 1Document7 pagesPalliative Care in Nephrology: The Work and The Workforce: Table 1Kev Jose Ruiz RojasNo ratings yet
- Occupational Therapist Career Research PaperDocument7 pagesOccupational Therapist Career Research Papernjxkgnwhf100% (1)
- OCCUP1Document6 pagesOCCUP1MartinNo ratings yet
- BibliopocDocument4 pagesBibliopocKarlo ReyesNo ratings yet
- Geriatric Nursing: Ma - Alicia Grace S. Kaimo, RN, ManDocument15 pagesGeriatric Nursing: Ma - Alicia Grace S. Kaimo, RN, ManYongNo ratings yet
- Practice GuidelineDocument3 pagesPractice Guidelineclarajimena25No ratings yet
- Final ProjectDocument2 pagesFinal Projectapi-293082830No ratings yet
- Therapeutic Interventions in Cerebral Palsy: Dilip R. PatelDocument5 pagesTherapeutic Interventions in Cerebral Palsy: Dilip R. PatelclikgoNo ratings yet
- NursepractitionerDocument4 pagesNursepractitionerapi-399029638No ratings yet
- Becoming A PTADocument4 pagesBecoming A PTAKrisha Mabel TabijeNo ratings yet
- Interviewing and Counseling The Dizzy Patient With Focus On Quality of LifeDocument9 pagesInterviewing and Counseling The Dizzy Patient With Focus On Quality of LifeCribea AdmNo ratings yet
- GERIATRICE HEALTH CARE TEAM-FinalDocument6 pagesGERIATRICE HEALTH CARE TEAM-Finalcamile buhangin100% (2)
- Clinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentDocument18 pagesClinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentΜαρία ΧανιωτάκηNo ratings yet
- For People With: Ractical Ral Are Developmental DisabilitiesDocument8 pagesFor People With: Ractical Ral Are Developmental DisabilitiesCristian AlberoniNo ratings yet
- Specialty Care Program AutismDocument8 pagesSpecialty Care Program AutismElian Y. Sanchez-RiveraNo ratings yet
- Geriatricrehabilitation: Gait in The Elderly, Fall Prevention and Parkinson DiseaseDocument17 pagesGeriatricrehabilitation: Gait in The Elderly, Fall Prevention and Parkinson DiseaseSandra Milena Cortes SotoNo ratings yet
- Health Team: Prepared By: Mr. J.C. FrankDocument27 pagesHealth Team: Prepared By: Mr. J.C. FrankHardeep KaurNo ratings yet
- OT For CPDocument15 pagesOT For CPYusrina RahmaNo ratings yet
- Cognitive Impairment EvaluationDocument20 pagesCognitive Impairment Evaluationdiana librerosNo ratings yet
- Other Health StaffDocument11 pagesOther Health StaffShanthal MercedesNo ratings yet
- Butler Darrah 2001Document13 pagesButler Darrah 2001Adnan Faris NaufalNo ratings yet
- Complementario 1Document8 pagesComplementario 1Camila OpazoNo ratings yet
- Health TeamDocument5 pagesHealth TeamFahim AhmedNo ratings yet
- 1.1, 1.2, 1.3, 1.5 Paediatric Nursing Presentation - 1-1Document54 pages1.1, 1.2, 1.3, 1.5 Paediatric Nursing Presentation - 1-1Christina YounasNo ratings yet
- Practical Oral Care For People With Autism 2012Document6 pagesPractical Oral Care For People With Autism 2012Amanda AmaroNo ratings yet
- N207 Theory Analysis and EvaluationDocument8 pagesN207 Theory Analysis and Evaluationpfprn100% (1)
- Geriatric Care TeamDocument29 pagesGeriatric Care TeamMarianne Joyce ManzoNo ratings yet
- DBT in ASDDocument9 pagesDBT in ASDCarregan AlvarezNo ratings yet
- OT Process and The 4 Levels of InterventionDocument3 pagesOT Process and The 4 Levels of InterventionMuhammad MukhlisNo ratings yet
- Module 5Document8 pagesModule 5tithi royNo ratings yet
- Unit 11. Advocacy Programs Relevant To The Care of OlderDocument13 pagesUnit 11. Advocacy Programs Relevant To The Care of OlderRichmon Joseph SantosNo ratings yet
- Therapeutic Interventions in The Treatment of Dissociative DisordersDocument18 pagesTherapeutic Interventions in The Treatment of Dissociative DisordersCarla MesquitaNo ratings yet
- Parchem 2018 A Multidisciplinary Approach To Equipment Use in Pediatric Patient Mobilization.Document10 pagesParchem 2018 A Multidisciplinary Approach To Equipment Use in Pediatric Patient Mobilization.Evelyn_D_az_Ha_8434No ratings yet
- Running Head: (GAGTAN, ANDREI RAPHAEL, L.)Document8 pagesRunning Head: (GAGTAN, ANDREI RAPHAEL, L.)Edmarkmoises ValdezNo ratings yet
- 200-CQDN-666574-ND - Job Description and Person SpecificationDocument6 pages200-CQDN-666574-ND - Job Description and Person Specificationsachin_sawant1985No ratings yet
- DocumentDocument11 pagesDocumentVvjjgxgjjNo ratings yet
- Nursing_Profile_2018Document22 pagesNursing_Profile_2018todotonteriasNo ratings yet
- Student Notes Professional Reasoning Na 2023Document39 pagesStudent Notes Professional Reasoning Na 2023mkhal700No ratings yet
- OtizmchapterDocument46 pagesOtizmchaptergokulraja850No ratings yet
- Almaz Mamaru Counseling Psychologist (BA, MA) Department of Psychiatry, Bahardar UniversityDocument39 pagesAlmaz Mamaru Counseling Psychologist (BA, MA) Department of Psychiatry, Bahardar UniversityAklile TsegaNo ratings yet
- 5f7c606e8ca92 - 11 Physical Education English Medium Chapter 4Document9 pages5f7c606e8ca92 - 11 Physical Education English Medium Chapter 4Practically UselessNo ratings yet
- The Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityDocument7 pagesThe Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityIJAR JOURNALNo ratings yet
- Lily Grebe Resume 10Document3 pagesLily Grebe Resume 10api-482765948No ratings yet
- UntitledDocument98 pagesUntitledixixNo ratings yet
- OCP 100 Course SyllabusDocument6 pagesOCP 100 Course SyllabusMegat LokmanNo ratings yet
- Training and Practice in Horticultural TherapyDocument149 pagesTraining and Practice in Horticultural TherapyKritikou1547No ratings yet
- MSWDO Capdev Form G1 FINALDocument50 pagesMSWDO Capdev Form G1 FINALbai yhang de la cruz100% (1)
- Occupational Problems and Barriers Reported by Individuals With ObesityDocument10 pagesOccupational Problems and Barriers Reported by Individuals With ObesityGraciela SeveriniNo ratings yet
- Sarah (Yosra) Azzam: EducationDocument3 pagesSarah (Yosra) Azzam: Educationapi-505318564No ratings yet
- ShannonjoyceresumeDocument2 pagesShannonjoyceresumeapi-303566481No ratings yet
- Curriculum Vita 2-3-16Document5 pagesCurriculum Vita 2-3-16api-308459832No ratings yet
- OT in Foster Care TransitionDocument10 pagesOT in Foster Care Transitionnoah87No ratings yet
- Occupational TherapyDocument2 pagesOccupational Therapyleen00170% (1)
- 23-05-2018 011346916 - Intervention Modalities - Chapter 16Document26 pages23-05-2018 011346916 - Intervention Modalities - Chapter 16Bisan RatuishNo ratings yet
- Hoppe and Matthews Cat Poster1Document1 pageHoppe and Matthews Cat Poster1api-238169773No ratings yet
- Suggestionfinal-OT Validation DocumentDocument91 pagesSuggestionfinal-OT Validation DocumentAdonis GaleosNo ratings yet
- Unit 1. Changing Trends & Career in Physical Education - Class-11Document6 pagesUnit 1. Changing Trends & Career in Physical Education - Class-11money d luffyNo ratings yet
- Occupational Therapy Dissertation Literature ReviewDocument4 pagesOccupational Therapy Dissertation Literature ReviewPsychologyPaperWritingServiceUKNo ratings yet
- Tic Poster FinalDocument1 pageTic Poster Finalapi-337168518No ratings yet
- Occupational Therapy: SATHISH Rajamani. M.SC (N) Lecturer AmconDocument20 pagesOccupational Therapy: SATHISH Rajamani. M.SC (N) Lecturer AmconSathish RajamaniNo ratings yet
- Chapter 4 F2fDocument28 pagesChapter 4 F2fManisha TidkeNo ratings yet
- An Occupational Perspective On Leadership, Theoratical and Practical Dimentions, 3e Sandra Dunbar-Smalley, Kristin WinstonDocument32 pagesAn Occupational Perspective On Leadership, Theoratical and Practical Dimentions, 3e Sandra Dunbar-Smalley, Kristin WinstonDing Bo50% (2)