Download as pdf or txt
You might also like
- Background: Reviews/Evaluations Antihistamines, H Receptor Antagonist Class ReviewDocument10 pagesBackground: Reviews/Evaluations Antihistamines, H Receptor Antagonist Class ReviewCah LilinNo ratings yet
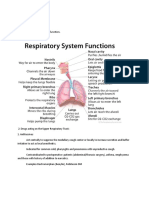
- Parmacology Respirasi: DR - Saiful BatubaraDocument24 pagesParmacology Respirasi: DR - Saiful BatubaraEryanda DinataNo ratings yet
- Antihistamines: A Brief ReviewDocument5 pagesAntihistamines: A Brief Reviewfkuii2009No ratings yet
- Antihistamines 20 August2021Document32 pagesAntihistamines 20 August2021bharatstudyNo ratings yet
- Antihistamines and Allergy: Katrina L RandallDocument4 pagesAntihistamines and Allergy: Katrina L RandalldhilahNo ratings yet
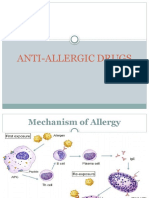
- Anti Allergic DrugsDocument30 pagesAnti Allergic DrugsNur Habib Al-BangkawiNo ratings yet
- AntihistaminesDocument83 pagesAntihistaminesKishore ChandkiNo ratings yet
- Histamine and Antihistamines. NotesDocument5 pagesHistamine and Antihistamines. NotesSubha2000100% (1)
- Antihistamin MeylersDocument1 pageAntihistamin MeylersfikaNo ratings yet
- MGDocument12 pagesMGelektron2010No ratings yet
- Histamine, Serotonin and Ergot AlkaloidsDocument36 pagesHistamine, Serotonin and Ergot AlkaloidsSteph Taylor Reyes RadanNo ratings yet
- Antihistamines - Classification Generation I ExamplesDocument4 pagesAntihistamines - Classification Generation I ExamplesjamesNo ratings yet
- AntihistamineDocument16 pagesAntihistamine30068No ratings yet
- Histamine, Serotonin and Ergot AlkaloidsDocument36 pagesHistamine, Serotonin and Ergot AlkaloidsSteph Taylor Reyes Radan100% (3)
- Janine Vega BSM 3 Phama Midterm ActivityDocument8 pagesJanine Vega BSM 3 Phama Midterm ActivityJanine VegaNo ratings yet
- 8 - Anti Allergic DrugsDocument8 pages8 - Anti Allergic DrugsMoataz TrabehNo ratings yet
- Anti Allergic DrugsDocument18 pagesAnti Allergic Drugsaamer niaziNo ratings yet
- Lecture 2 Histmaine Antagonists (UNR)Document27 pagesLecture 2 Histmaine Antagonists (UNR)Aiman MeerNo ratings yet
- Antihistamines in Children and Adolescents: A Practical UpdateDocument10 pagesAntihistamines in Children and Adolescents: A Practical Updateahmed fareedNo ratings yet
- Antihistamine BlockersDocument12 pagesAntihistamine Blockersyra capiliNo ratings yet
- Anti-Histamines Agents PDFDocument18 pagesAnti-Histamines Agents PDFBintoo SharmaNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document21 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Sadam ArigaNo ratings yet
- Antihistamínicos en PediatríaDocument10 pagesAntihistamínicos en PediatríaAdrianRuizNo ratings yet
- Bab IiDocument5 pagesBab IiRahman JrNo ratings yet
- Unit 7 Autacoids: StructureDocument9 pagesUnit 7 Autacoids: StructureSwapnilPagareNo ratings yet
- CristineBSM 3 Phama Midterm ActivityDocument7 pagesCristineBSM 3 Phama Midterm ActivityJanine VegaNo ratings yet
- Antiallergic Drugs, Drugs For Immune SistemDocument38 pagesAntiallergic Drugs, Drugs For Immune SistemTawhid ZihadNo ratings yet
- Drugs For Allergic Rhinitis Cough and ColdDocument26 pagesDrugs For Allergic Rhinitis Cough and ColdChandana Sri LalamNo ratings yet
- Drugs On RespiratoryDocument17 pagesDrugs On RespiratoryIrwan M. IskoberNo ratings yet
- Jelie Rose BSM 3 Phama Midterm ActivityDocument8 pagesJelie Rose BSM 3 Phama Midterm ActivityJanine VegaNo ratings yet
- Antihistamines 61926Document6 pagesAntihistamines 61926Evelina NastasNo ratings yet
- Lo 4 Sk1 Rhinitis AlergiDocument4 pagesLo 4 Sk1 Rhinitis AlergiFullyNo ratings yet
- Pakistan Journal of Pharmaceutical ResearchDocument6 pagesPakistan Journal of Pharmaceutical ResearchnabiNo ratings yet
- Histamine Antagonists: Dr. Anil Kumar SaxenaDocument17 pagesHistamine Antagonists: Dr. Anil Kumar SaxenaLuqman Al-Bashir FauziNo ratings yet
- Drug of Therapy Allergy DiseaseDocument32 pagesDrug of Therapy Allergy DiseaseIndahYuliiarniPutriNongtjiNo ratings yet
- H2 AntagonistDocument50 pagesH2 AntagonistMosbally YassinNo ratings yet
- Histamine and Antihistamine Drugs2011Document8 pagesHistamine and Antihistamine Drugs2011Yunan Syahban MaskatNo ratings yet
- AntihistaminesDocument4 pagesAntihistaminessharvabhasin0% (1)
- Allergic Rhinitis: Postgraduate MedicineDocument10 pagesAllergic Rhinitis: Postgraduate Medicineazwin lubisNo ratings yet
- AutacoidsDocument103 pagesAutacoidsKamran Ali100% (2)
- Acfrogcmuqv1z T0qaucxvbfwtfin2xu Xkrzp4ddeso7qwbd Fha38sq6mihfw2aozwxn5r0mxgmgmkvemhr46tntlwea3quddq9w2pmvyn6by5wqcyi7ge8gmmnzlzhis 1dzejbeghuvr9bapDocument7 pagesAcfrogcmuqv1z T0qaucxvbfwtfin2xu Xkrzp4ddeso7qwbd Fha38sq6mihfw2aozwxn5r0mxgmgmkvemhr46tntlwea3quddq9w2pmvyn6by5wqcyi7ge8gmmnzlzhis 1dzejbeghuvr9bapFareed KhanNo ratings yet
- Autacoid (Suryosutanto, DR)Document35 pagesAutacoid (Suryosutanto, DR)Dedy SantosoNo ratings yet
- Antihistamines 101 Munich 06-05Document15 pagesAntihistamines 101 Munich 06-05pentruNo ratings yet
- ASCIA Allergic Rhinitis Treatment Plan 2020Document1 pageASCIA Allergic Rhinitis Treatment Plan 2020BigPharma HealtcareNo ratings yet
- AntihistaminesDocument2 pagesAntihistaminesmercywicherNo ratings yet
- AntihistaminesDocument4 pagesAntihistaminesEvans Oktora RolindriNo ratings yet
- Antihistamines Case StudyDocument5 pagesAntihistamines Case StudySpaynkterNo ratings yet
- Histamine: Moderator: Dr. Pooja Shukla Resident: Fariha Fatima JR-2Document45 pagesHistamine: Moderator: Dr. Pooja Shukla Resident: Fariha Fatima JR-2;'SiLeNt';No ratings yet
- AntihistaminesDocument17 pagesAntihistaminesreza_adrian_2No ratings yet
- The Use of Antihistamines in Children 2016 Paediatrics and Child HealthDocument4 pagesThe Use of Antihistamines in Children 2016 Paediatrics and Child Healthgeorgi.annaNo ratings yet
- Pharmacology of AntihistaminesDocument11 pagesPharmacology of AntihistaminesAnggoro Adi WibowoNo ratings yet
- Antihistamin PDFDocument7 pagesAntihistamin PDFKarina Mega W100% (1)
- Summary & Study Guide - Mind over Meds: When to Let Your Body Heal on Its OwnFrom EverandSummary & Study Guide - Mind over Meds: When to Let Your Body Heal on Its OwnNo ratings yet
- Histamine Intolerance: The Comprehensive Guide for Healthcare ProfessionalsFrom EverandHistamine Intolerance: The Comprehensive Guide for Healthcare ProfessionalsNo ratings yet
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]From EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Rating: 4 out of 5 stars4/5 (1)
- The Best Practice Is The Lowest Effective Dose Your Third Psychiatric Consultation: Diet, Exercise, and Sleep Trump Medications Medication is the Last Option Your Fourth Psychiatric ConsultationFrom EverandThe Best Practice Is The Lowest Effective Dose Your Third Psychiatric Consultation: Diet, Exercise, and Sleep Trump Medications Medication is the Last Option Your Fourth Psychiatric ConsultationNo ratings yet
- Fast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlFrom EverandFast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlNo ratings yet
- Bala Lecture Changing Trends in SinusitisDocument26 pagesBala Lecture Changing Trends in SinusitisBalakrishnan DoraisamiNo ratings yet
- Common ENT 1 Hearing LossDocument24 pagesCommon ENT 1 Hearing LossBalakrishnan DoraisamiNo ratings yet
- The Unique 24 x7 Aero Digestive Foreign Body Service at Institute of Child Health - Some Instructive AnecdotesDocument3 pagesThe Unique 24 x7 Aero Digestive Foreign Body Service at Institute of Child Health - Some Instructive AnecdotesBalakrishnan DoraisamiNo ratings yet
- Care of Voice 20170105 1 DBDocument42 pagesCare of Voice 20170105 1 DBBalakrishnan DoraisamiNo ratings yet
- Electro Surgery PPT 5 SlidesDocument5 pagesElectro Surgery PPT 5 SlidesBalakrishnan DoraisamiNo ratings yet
- FB Airway Anecdotal Article Full 14102013Document5 pagesFB Airway Anecdotal Article Full 14102013Balakrishnan DoraisamiNo ratings yet
- Chennai Clinical CentreDocument53 pagesChennai Clinical CentreBalakrishnan DoraisamiNo ratings yet
- WCI2015 F0 Algorithm Prarthana Gladis Bala Author ManuscriptDocument5 pagesWCI2015 F0 Algorithm Prarthana Gladis Bala Author ManuscriptBalakrishnan DoraisamiNo ratings yet
- Dental LectDocument69 pagesDental LectBalakrishnan DoraisamiNo ratings yet
- Acute Otitis Media: D.BalakrishnanDocument44 pagesAcute Otitis Media: D.BalakrishnanBalakrishnan DoraisamiNo ratings yet
- How To Impress Someone at First MeetingDocument1 pageHow To Impress Someone at First MeetingMohammad Fahim HossainNo ratings yet
- Cadence Vol 23Document38 pagesCadence Vol 23api-3709957No ratings yet
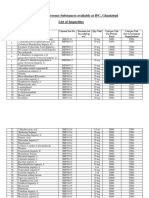
- List of IP Reference Substances Available at IPC, Ghaziabad List of ImpuritiesDocument4 pagesList of IP Reference Substances Available at IPC, Ghaziabad List of ImpuritiesUrva VasavadaNo ratings yet
- Current Status, Research Trends, and ChallengesDocument23 pagesCurrent Status, Research Trends, and Challengesqgi-tanyaNo ratings yet
- Ipad - Apple Technician Guide (2011)Document116 pagesIpad - Apple Technician Guide (2011)Jonathan Long100% (1)
- Sun ScopeDocument3 pagesSun ScopeJimNo ratings yet
- Chapter 2-Computer Security Attacks and ThreatsDocument40 pagesChapter 2-Computer Security Attacks and ThreatsYohannes DerejeNo ratings yet
- English Chapter 5Document20 pagesEnglish Chapter 5Kumar sankar SNo ratings yet
- Power-Linker Training Centre: GroupDocument1 pagePower-Linker Training Centre: GroupSunil SinghNo ratings yet
- Worlds Beyond Our Ice Wall Isoa4Document10 pagesWorlds Beyond Our Ice Wall Isoa4hujankopiairNo ratings yet
- Microsoft For Startups Deck 19Document20 pagesMicrosoft For Startups Deck 19Rajni Kant Sinha100% (1)
- Evaluation Rating Sheet For Charts Poster Drill Flash Card and ManipulativesDocument3 pagesEvaluation Rating Sheet For Charts Poster Drill Flash Card and ManipulativesMaricris Bagnes SaludNo ratings yet
- Chilliwack To Surrey Interurban Final ReportDocument84 pagesChilliwack To Surrey Interurban Final ReportSurrey/North Delta LeaderNo ratings yet
- 3544 Im 21455-30Document58 pages3544 Im 21455-30grosselloNo ratings yet
- FCS195 - Essay 2 GuidelinesDocument2 pagesFCS195 - Essay 2 GuidelinesaaaaanksNo ratings yet
- Social MediaDocument4 pagesSocial MediaJeff_Yu_5215No ratings yet
- (EE-335) - Electric Power Generation, Transmission, and Distribution-Fall2021Document8 pages(EE-335) - Electric Power Generation, Transmission, and Distribution-Fall2021Abeer SohailNo ratings yet
- Neurological Development From Birth To Six YearsDocument143 pagesNeurological Development From Birth To Six YearsWaleska SakibNo ratings yet
- Decribing Connections Between Historical EventsDocument4 pagesDecribing Connections Between Historical Eventsapi-334916201No ratings yet
- Country Profile Malawi 2014 PDFDocument12 pagesCountry Profile Malawi 2014 PDFJack MalambeNo ratings yet
- SS Ind A21 BVX002 - Approval of Permanent Joining Procedure and PersonnelDocument1 pageSS Ind A21 BVX002 - Approval of Permanent Joining Procedure and PersonnelTuTuy AnNo ratings yet
- Alexandre SettlementHistoryNazareth 2020Document69 pagesAlexandre SettlementHistoryNazareth 2020Guillermo UribeNo ratings yet
- Hobsbawm and Ranger - The Invention of TraditionDocument330 pagesHobsbawm and Ranger - The Invention of TraditionIván Parada Hernández75% (4)
- Marketing Management Course OutlineDocument6 pagesMarketing Management Course OutlineChandrakant VadluruNo ratings yet
- SM-J700H Schematic PartlistDocument9 pagesSM-J700H Schematic PartlistAlan AhmedNo ratings yet
- IEEE Standards Style ManualDocument70 pagesIEEE Standards Style ManualDiego Agudelo ContrerasNo ratings yet
- Level 6 Advanced - A Room With A ViewDocument117 pagesLevel 6 Advanced - A Room With A View01.wawiwawi100% (1)
- Fiber Optic Cable Blowing MachinesDocument7 pagesFiber Optic Cable Blowing MachinesDiar FatahNo ratings yet
- Department of Electronics and Communication Engineering: Subject: Vlsi Signal ProcessingDocument8 pagesDepartment of Electronics and Communication Engineering: Subject: Vlsi Signal ProcessingRaja PirianNo ratings yet
- Anterior Chamber Angle Assessment Technique - CH 17Document20 pagesAnterior Chamber Angle Assessment Technique - CH 17riveliNo ratings yet




















































![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-2-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)