Download as pdf or txt
You might also like
- Case Study On LBWDocument43 pagesCase Study On LBWOmotosho Alex50% (2)
- ACOG - External Cephalic Version PDFDocument10 pagesACOG - External Cephalic Version PDFPat CabanitNo ratings yet
- 单绒毛膜双胞胎妊娠的结果并伴有III型选择性宫内生长受限Ultrasound Obstet GynecolDocument8 pages单绒毛膜双胞胎妊娠的结果并伴有III型选择性宫内生长受限Ultrasound Obstet GynecolchenziendrNo ratings yet
- ECPM2016 ABSTRACTBOOKTheJournalofMaternal-FetalNeonatalMedicine PDFDocument314 pagesECPM2016 ABSTRACTBOOKTheJournalofMaternal-FetalNeonatalMedicine PDFDiana-Elena ComandasuNo ratings yet
- Fibroid TumorsDocument5 pagesFibroid TumorscacingpandoraNo ratings yet
- UOG - 2019 - Curado - Early and Late Onset Selective Fetal Growth Restriction in MonochorionicDocument6 pagesUOG - 2019 - Curado - Early and Late Onset Selective Fetal Growth Restriction in MonochorionicnehamohindrooNo ratings yet
- Risk Factors and Outcomes of Umbilical Cord Prolapse: Evaluation of 94 CasesDocument3 pagesRisk Factors and Outcomes of Umbilical Cord Prolapse: Evaluation of 94 CasesElva Diany SyamsudinNo ratings yet
- Intrauterine Growth Restriction IUGR Etiology andDocument11 pagesIntrauterine Growth Restriction IUGR Etiology andRona Maulidia BakhitaNo ratings yet
- AUB DR Irfani IskakDocument11 pagesAUB DR Irfani IskakSaskiaaNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticlefeyzarezarNo ratings yet
- Iugr PDFDocument2 pagesIugr PDFjackyploesNo ratings yet
- Optimizing The Definition of Intrauterine Growth Restriction: The Multicenter Prospective PORTO StudyDocument6 pagesOptimizing The Definition of Intrauterine Growth Restriction: The Multicenter Prospective PORTO StudyfujimeisterNo ratings yet
- Crecimiento y Desarrollo FetalDocument16 pagesCrecimiento y Desarrollo Fetalalejandra mejia jimenezNo ratings yet
- Aydin 2017Document7 pagesAydin 2017Berry BancinNo ratings yet
- FMT 4 3 3Document5 pagesFMT 4 3 3kimsrfforensicmedicineNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument4 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologytiaranindyNo ratings yet
- Iugr FGRDocument10 pagesIugr FGRGilang Hadi FNo ratings yet
- Intrauterine Growth Restriction IUGR Etiology andDocument11 pagesIntrauterine Growth Restriction IUGR Etiology andFlavia Angelina SatopohNo ratings yet
- Prevalence of Congenital Anomalies in Neonates and Associated Risk Factors in A Tertiary Care Hospital in Eastern IndiaDocument7 pagesPrevalence of Congenital Anomalies in Neonates and Associated Risk Factors in A Tertiary Care Hospital in Eastern Indiameylisa putri ayunandaNo ratings yet
- Significance of Abnormal Umbilical Artery Doppler Studies in Normally Grown FetusesDocument7 pagesSignificance of Abnormal Umbilical Artery Doppler Studies in Normally Grown FetusesObsgin Januari17No ratings yet
- The Genetics and Clinical Outcomes in 151 Cases OfDocument7 pagesThe Genetics and Clinical Outcomes in 151 Cases Ofzeni okta wiyantiNo ratings yet
- This Is From Web. Credits To The OwnerDocument40 pagesThis Is From Web. Credits To The OwnerYanna Habib-MangotaraNo ratings yet
- Autopsia Fetal 2do TrimestreDocument8 pagesAutopsia Fetal 2do Trimestrecamila seguelNo ratings yet
- Eke2019 PDFDocument1 pageEke2019 PDFWijitha VarenniNo ratings yet
- 单绒毛膜双胞胎怀孕的胎儿死亡预测,并伴有III型选择性胎儿生长受限制Ultrasound Obstet GynecolDocument8 pages单绒毛膜双胞胎怀孕的胎儿死亡预测,并伴有III型选择性胎儿生长受限制Ultrasound Obstet GynecolchenziendrNo ratings yet
- Am J Perinatol 2023 - Latency Period After Preterm Premature Rupture of Membranes, Singletons Versus TwinsDocument6 pagesAm J Perinatol 2023 - Latency Period After Preterm Premature Rupture of Membranes, Singletons Versus TwinsCharlie CharcapeNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: BackgroundHartanto LieNo ratings yet
- NIH Public Access: Author ManuscriptDocument21 pagesNIH Public Access: Author ManuscriptanyNo ratings yet
- Diagnosis of IUGR: Traditional Biometry: Elizabeth Platz, MD, and Roger Newman, MDDocument8 pagesDiagnosis of IUGR: Traditional Biometry: Elizabeth Platz, MD, and Roger Newman, MDBella DirkNo ratings yet
- Prediction of Recurrent Preeclampsia Using First-Trimester Uterine Artery DopplerDocument6 pagesPrediction of Recurrent Preeclampsia Using First-Trimester Uterine Artery Dopplerganesh reddyNo ratings yet
- Original ArticleDocument8 pagesOriginal ArticleFelicia DympnaNo ratings yet
- Deense Studie PDFDocument12 pagesDeense Studie PDFBas HermansNo ratings yet
- Karami 2018Document13 pagesKarami 2018sbm3.enggNo ratings yet
- Preterm Birth Analysis of Risk Factors and Neonatal OutcomeDocument5 pagesPreterm Birth Analysis of Risk Factors and Neonatal Outcomehinduja reddipilliNo ratings yet
- Screening For Fetal Growth Restriction Using Ultrasound and The Sflt1/Plgf Ratio in Nulliparous Women: A Prospective Cohort StudyDocument13 pagesScreening For Fetal Growth Restriction Using Ultrasound and The Sflt1/Plgf Ratio in Nulliparous Women: A Prospective Cohort StudynicolasdlcaNo ratings yet
- Rustico 2016Document23 pagesRustico 2016Andrea Ponce AmesNo ratings yet
- Natural History of Fetal Position During Pregnancy.11Document6 pagesNatural History of Fetal Position During Pregnancy.11PutriNo ratings yet
- Aogs 14255Document6 pagesAogs 14255Christian YzaguirreNo ratings yet
- Del 153Document6 pagesDel 153Fan AccountNo ratings yet
- Thyroid and Pregnancy OutcomeDocument9 pagesThyroid and Pregnancy OutcomeCindy KestyNo ratings yet
- Jum 15063Document9 pagesJum 15063Nam NguyenNo ratings yet
- Acta Obstet Gynecol Scand - 2004 - Olofsson - Low Umbilical Artery Vascular Flow Resistance and Fetal OutcomeDocument3 pagesActa Obstet Gynecol Scand - 2004 - Olofsson - Low Umbilical Artery Vascular Flow Resistance and Fetal OutcomeSiti AminathinNo ratings yet
- Genetics and Epigenetics of Infertility and Treatments On OutcomesDocument16 pagesGenetics and Epigenetics of Infertility and Treatments On OutcomesCamii Cv100% (1)
- Levonorgestrel vs. Copper Intrauterine en AnticoncepciónDocument10 pagesLevonorgestrel vs. Copper Intrauterine en AnticoncepciónJose Alejandro Bedoya SanchezNo ratings yet
- Prevalence of Congenital Malformation Among Neonates Born After The Use of Progesterone For Luteal Support During IVF and ICSI CyclesDocument7 pagesPrevalence of Congenital Malformation Among Neonates Born After The Use of Progesterone For Luteal Support During IVF and ICSI Cycleseditorial.boardNo ratings yet
- Nama: Winda Eriyanti NIM: 113063C1-14070 Kelas/Semester: B/VIDocument3 pagesNama: Winda Eriyanti NIM: 113063C1-14070 Kelas/Semester: B/VIPuspa ThenurseofsiagaNo ratings yet
- $116 SMFM AbstractsDocument1 page$116 SMFM AbstractsSheila Regina TizaNo ratings yet
- Risk Factors For Neonatal Asphyxia Occurrence at General Hospital Dr. M. Soewandhie, SurabayaDocument6 pagesRisk Factors For Neonatal Asphyxia Occurrence at General Hospital Dr. M. Soewandhie, SurabayaFatimah FadilahNo ratings yet
- Fracture of The Clavicle in The Newborn Following Normal Labor and DeliveryDocument6 pagesFracture of The Clavicle in The Newborn Following Normal Labor and DeliveryAlberto OrtizNo ratings yet
- Jurnal Ultrasound 1Document6 pagesJurnal Ultrasound 1weniNo ratings yet
- A Case Control Study of Risk Factors and Neonatal Outcomes of Preterm BirthDocument5 pagesA Case Control Study of Risk Factors and Neonatal Outcomes of Preterm BirthSarahí SosaNo ratings yet
- Inductin of LaborDocument5 pagesInductin of LaborGema Akbar WakhidanaNo ratings yet
- Consequences of Prenatal Ultrasound Diagnosis: A Preliminary Report On Neonates With Congenital MalformationsDocument8 pagesConsequences of Prenatal Ultrasound Diagnosis: A Preliminary Report On Neonates With Congenital MalformationsSafinaz InazNo ratings yet
- BJOG - 2019 - Adanikin - Maternal Near Miss and Death Associated With Abortive Pregnancy Outcome A Secondary Analysis ofDocument8 pagesBJOG - 2019 - Adanikin - Maternal Near Miss and Death Associated With Abortive Pregnancy Outcome A Secondary Analysis ofafrinaNo ratings yet
- Do Assisted Conception Twins Have An Increased Risk For AnencephalyDocument6 pagesDo Assisted Conception Twins Have An Increased Risk For AnencephalyTiffanyNo ratings yet
- Less Is More Modern NeonatologyDocument11 pagesLess Is More Modern NeonatologyEN BUNo ratings yet
- Use of Injection Solcoseryl For The Treatment of OligohydramniosDocument7 pagesUse of Injection Solcoseryl For The Treatment of OligohydramniosJosselle Sempio CalientaNo ratings yet
- Assessment of Fresh Vs Macerated As Acurate Markers of Time Since IUFD in Low-Income CountriesDocument5 pagesAssessment of Fresh Vs Macerated As Acurate Markers of Time Since IUFD in Low-Income CountriesDenys PutraNo ratings yet
- Screening For Fetal Chromosomal AbdnormalitiesDocument22 pagesScreening For Fetal Chromosomal AbdnormalitiesAlejandra MurilloNo ratings yet
- Jsafog 9 323 PDFDocument4 pagesJsafog 9 323 PDFSul FadlyNo ratings yet
- Treatment Strategy for Unexplained Infertility and Recurrent MiscarriageFrom EverandTreatment Strategy for Unexplained Infertility and Recurrent MiscarriageKeiji KurodaNo ratings yet
- Endometrial Gene Expression: An Emerging Paradigm for Reproductive DisordersFrom EverandEndometrial Gene Expression: An Emerging Paradigm for Reproductive DisordersJoanne Kwak-KimNo ratings yet
- Cryotherapy Versus Cold Coagulation For Treating Cervical Precancerous LesionsDocument5 pagesCryotherapy Versus Cold Coagulation For Treating Cervical Precancerous LesionsMeycha Da FhonsaNo ratings yet
- 14 06 sIUGR Florence 2 PDFDocument19 pages14 06 sIUGR Florence 2 PDFMeycha Da FhonsaNo ratings yet
- Risk Factors of Neonatal Sepsis: A Preliminary Study in Dr. Soetomo HospitalDocument4 pagesRisk Factors of Neonatal Sepsis: A Preliminary Study in Dr. Soetomo HospitalMeycha Da FhonsaNo ratings yet
- Penetrating Skull Fracture by A Wooden Object: Management Dilemmas and Literature ReviewDocument4 pagesPenetrating Skull Fracture by A Wooden Object: Management Dilemmas and Literature ReviewMeycha Da FhonsaNo ratings yet
- Distal AnDocument99 pagesDistal AnMeycha Da FhonsaNo ratings yet
- Study Questions 3Document12 pagesStudy Questions 3CGNo ratings yet
- E-ISSN: 2347-8640 P-ISSN: 2454-2660, Issue JETIR, (JULY September 2016)Document9 pagesE-ISSN: 2347-8640 P-ISSN: 2454-2660, Issue JETIR, (JULY September 2016)VaishaliNo ratings yet
- The Uses and Limitations of The Fetal Biophysical Profile.Document18 pagesThe Uses and Limitations of The Fetal Biophysical Profile.Diego Ortecho100% (1)
- Termini Latinu ValodaDocument4 pagesTermini Latinu ValodaJulianna Muceniece0% (1)
- Post-Partum Hemorrhage Pathophysiology PaperDocument5 pagesPost-Partum Hemorrhage Pathophysiology Paperapi-399619969No ratings yet
- AbortionDocument32 pagesAbortionKirandeep Parmar100% (1)
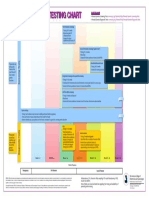
- Prenatal Genetic Testing ChartDocument1 pagePrenatal Genetic Testing ChartMorningDewNo ratings yet
- Human Services, Public Health Integration Report 2021Document17 pagesHuman Services, Public Health Integration Report 2021inforumdocsNo ratings yet
- Ebr MacalolotDocument4 pagesEbr Macalolotquen.chuaNo ratings yet
- The Impact of Teenage Pregnancy On Maternal, Fetal and Neonatal OutcomesDocument8 pagesThe Impact of Teenage Pregnancy On Maternal, Fetal and Neonatal Outcomesjacque najeraNo ratings yet
- HydramniosDocument30 pagesHydramniosRahul BaruahNo ratings yet
- Module 1 Framework For Maternal and Child Health NursingDocument7 pagesModule 1 Framework For Maternal and Child Health NursingCha SahiddanNo ratings yet
- The Initial Prenatal Assessment and Routine Prenatal CareDocument16 pagesThe Initial Prenatal Assessment and Routine Prenatal Carelacminhhien100% (1)
- Overview of Ultrasound Examination in Obstetrics and Gynecology - UpToDateDocument27 pagesOverview of Ultrasound Examination in Obstetrics and Gynecology - UpToDateRopiNo ratings yet
- Case Study OligoDocument7 pagesCase Study OligomutiaNo ratings yet
- Cwu O&g 1 PPROMDocument13 pagesCwu O&g 1 PPROMFaris Mohd Nasir100% (1)
- Prof. Dr. Farhana Dewan, Dr. Mariha Alam Chowdhury, Dr. Khairun NessaDocument6 pagesProf. Dr. Farhana Dewan, Dr. Mariha Alam Chowdhury, Dr. Khairun Nessasumaiya zaforNo ratings yet
- Lesson Plan Umbilcal CordDocument10 pagesLesson Plan Umbilcal CordJyoti Prem UttamNo ratings yet
- Ateneo de Zamboanga University: College of Nursing Level 2Document7 pagesAteneo de Zamboanga University: College of Nursing Level 2Sheryhan Tahir BayleNo ratings yet
- Specialties 250 SBAs For FinalsDocument292 pagesSpecialties 250 SBAs For FinalsSiddharth BasettiNo ratings yet
- Rcog PpromDocument7 pagesRcog PpromDevi SyamNo ratings yet
- Maternal and Child Health NSG SummaryDocument2 pagesMaternal and Child Health NSG SummaryAshley Jane MacapayadNo ratings yet
- Caesarean SectionDocument23 pagesCaesarean SectionIdiAmadouNo ratings yet
- Breech PresentationDocument46 pagesBreech PresentationushaNo ratings yet
- Bayesian Analysis of Infant Mortality in Oyo State, NigeriaDocument6 pagesBayesian Analysis of Infant Mortality in Oyo State, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Determinan Maternal Kejadian Preeklampsia (Studi Kasus Di Kabupaten Tegal, Jawa Tengah) Natiqotul Fatkhiyah, Kodiyah, MasturohDocument9 pagesDeterminan Maternal Kejadian Preeklampsia (Studi Kasus Di Kabupaten Tegal, Jawa Tengah) Natiqotul Fatkhiyah, Kodiyah, Masturohpulo lestariNo ratings yet
- Occipito Posterior (PositionDocument44 pagesOccipito Posterior (PositionArambam Aruna100% (6)
- OBST ACOG Practice Bulletin No 101 Ultrasonography in PregnancyDocument11 pagesOBST ACOG Practice Bulletin No 101 Ultrasonography in PregnancyEduardo Agustín Vargas CamposNo ratings yet