Download as pdf or txt
You might also like
- CSCS Study GuideDocument50 pagesCSCS Study GuideMatt Siniscalchi100% (6)
- Excitable Tissues: DR Joseph WabwireDocument38 pagesExcitable Tissues: DR Joseph WabwireJoseph WabwireNo ratings yet
- Sabers HandbookDocument35 pagesSabers HandbookMohammadSAL-Rawashdeh100% (1)
- Opleidingen Voor Personal Trainers - Deel 1 OVERLOAD WORLDWIDEDocument27 pagesOpleidingen Voor Personal Trainers - Deel 1 OVERLOAD WORLDWIDEOverload WorldwideNo ratings yet
- Wim Hof Method PDFDocument4 pagesWim Hof Method PDFAnonymous HsAAhXFnGp100% (12)
- Pediatric Assessment Triangle EditDocument31 pagesPediatric Assessment Triangle EditAlbert Gunawan100% (1)
- Cardiology Ekg BoardDocument87 pagesCardiology Ekg BoardPutri WijayaNo ratings yet
- Physiology and Pharmacology of The Renal Pelvis andDocument88 pagesPhysiology and Pharmacology of The Renal Pelvis andmauricio paracheNo ratings yet
- Vascular Smooth MuscleDocument45 pagesVascular Smooth MuscleFatima Zahra Saddouk100% (1)
- Activity-Dependent Structural and Functional Plasticity of Astrocyte-Neuron InteractionsDocument20 pagesActivity-Dependent Structural and Functional Plasticity of Astrocyte-Neuron InteractionsAmar JitjNo ratings yet
- Skeletal Muscle Physiology PDFDocument6 pagesSkeletal Muscle Physiology PDFAstri Ggamjong Xiao LuNo ratings yet
- Steps Involved in Neurotransmission Pharmacology PPT1Document23 pagesSteps Involved in Neurotransmission Pharmacology PPT1S BiswajitNo ratings yet
- Renal Pelvis and UreterDocument4 pagesRenal Pelvis and UreterFasie DragosNo ratings yet
- Ureter Do RatoDocument6 pagesUreter Do Ratonilberto2No ratings yet
- SGD 4 - Skeletal Muscle PhysiologyDocument3 pagesSGD 4 - Skeletal Muscle PhysiologyKriska Noelle0% (1)
- Nervous SystemDocument34 pagesNervous SystemKoimahNo ratings yet
- Neurocytology I - The Structure of The NeuronDocument46 pagesNeurocytology I - The Structure of The NeuronMaharshi MajmundarNo ratings yet
- SynapsesDocument6 pagesSynapsesJeff ParkNo ratings yet
- Molecular Mechanisms of Neurotransmitter ReleaseDocument21 pagesMolecular Mechanisms of Neurotransmitter ReleaseNusrat JahanNo ratings yet
- BIO3420.2010.5Muscle Part 2 06oct10 2Document27 pagesBIO3420.2010.5Muscle Part 2 06oct10 2aemilianneNo ratings yet
- Overview of PhysiologyDocument35 pagesOverview of Physiologyمعاذ عبد الكريم البازليNo ratings yet
- Smooth Muscle Contraction and Relaxation Advances in Physiology Education PDFDocument1 pageSmooth Muscle Contraction and Relaxation Advances in Physiology Education PDFBrizo BNo ratings yet
- Physiology Linda Costanzo 6th 1Document50 pagesPhysiology Linda Costanzo 6th 1Moonnime BlueNo ratings yet
- Mock Exam Feedback HPP 2021Document47 pagesMock Exam Feedback HPP 2021yusm2312No ratings yet
- Key of SEQs Heart, Nerve and Muscle Revision TestDocument11 pagesKey of SEQs Heart, Nerve and Muscle Revision TestMudassar Roomi100% (2)
- Fizobioqimia FinalDocument12 pagesFizobioqimia FinalTamar PertiaNo ratings yet
- Kennedy 1989Document4 pagesKennedy 1989Eduardo TarangoNo ratings yet
- Autonomic Nervous SystemDocument19 pagesAutonomic Nervous SystemAnuvabNo ratings yet
- Principles of Cardiac ElectrophysiologyDocument98 pagesPrinciples of Cardiac ElectrophysiologyAbnet WondimuNo ratings yet
- Cellular Biology of EpileptogenesisDocument10 pagesCellular Biology of EpileptogenesisandreacamachogonNo ratings yet
- Action Potential in NeuronsDocument109 pagesAction Potential in NeuronsAdmin0% (1)
- Synapses and Synaptic TransmissionDocument19 pagesSynapses and Synaptic TransmissionSabinaNo ratings yet
- Neuromuscular JunctionDocument10 pagesNeuromuscular JunctionAfeefuddin ShaikhNo ratings yet
- Lecture 7 Nervous System 1 - STRUCTURE FUNCTIONDocument28 pagesLecture 7 Nervous System 1 - STRUCTURE FUNCTIONhafiz patahNo ratings yet
- Pathological and Chemical Effectors of The Erythrocyte Calcium Pumping Protein: A Review.Document15 pagesPathological and Chemical Effectors of The Erythrocyte Calcium Pumping Protein: A Review.Clement BewajiNo ratings yet
- Synapse and Muscle Physiology: Lecturer - I. Savinkova, PHD Department of PhysiologyDocument50 pagesSynapse and Muscle Physiology: Lecturer - I. Savinkova, PHD Department of PhysiologyИринаNo ratings yet
- Potential Action of Muscle SkeletalDocument19 pagesPotential Action of Muscle SkeletalAyuNo ratings yet
- Chapter 3 and 4 - Muscles and NerveDocument19 pagesChapter 3 and 4 - Muscles and Nervetahira UroojNo ratings yet
- Mechanisms of Muscle Fatigue in Intense ExerciseDocument12 pagesMechanisms of Muscle Fatigue in Intense ExerciseCharisNo ratings yet
- MUSCLESDocument3 pagesMUSCLESalihusseinNo ratings yet
- Tell Them What You're Going To Tell Them. Tell Them. Tell Them What You Just Told Them. AristotleDocument17 pagesTell Them What You're Going To Tell Them. Tell Them. Tell Them What You Just Told Them. AristotleSafiya JamesNo ratings yet
- Topic 15 Nervous Coordination AO1 QuizDocument8 pagesTopic 15 Nervous Coordination AO1 QuizatemisgoddesofhuntNo ratings yet
- M - PH: The Relationship Between Length and Active Force of A Skeletal MuscleDocument11 pagesM - PH: The Relationship Between Length and Active Force of A Skeletal MuscleFlowerNo ratings yet
- MSS Module Year One 2024Document43 pagesMSS Module Year One 2024Thaw Tar Noe WaiNo ratings yet
- Synaptic Transmission: Communication Between NeuronsDocument48 pagesSynaptic Transmission: Communication Between NeuronsEarl Adam LambacoNo ratings yet
- 2022 Set-EXCITABLE TISSUES Membrane Potential & NeuronsDocument53 pages2022 Set-EXCITABLE TISSUES Membrane Potential & NeuronsSamuel BenjaminNo ratings yet
- SynapsesDocument46 pagesSynapseshan abuur ahmedNo ratings yet
- Action PotenialDocument21 pagesAction PotenialSanjay MaharjanNo ratings yet
- M HypothalamusDocument15 pagesM HypothalamusSrilakshmi SridharanNo ratings yet
- Nervous SystemDocument27 pagesNervous SystemamuyawtheophilusNo ratings yet
- Essay On Physiology (Excitable)Document33 pagesEssay On Physiology (Excitable)Emmanuel IshiomaNo ratings yet
- Ptm13 KajianBio SINAPSDocument37 pagesPtm13 KajianBio SINAPSAmin Khusnadiyah aminkhusnadiyah.2020No ratings yet
- Bio 336 Physio Exam 1 EssaysDocument3 pagesBio 336 Physio Exam 1 EssayssheilaNo ratings yet
- Neuromuscular PhysiologyDocument44 pagesNeuromuscular PhysiologyAnkita NigamNo ratings yet
- Nervous SystemDocument23 pagesNervous SystemMartyn PereiraNo ratings yet
- NP2 PDFDocument27 pagesNP2 PDFRajat AgrawalNo ratings yet
- Cellular Physiology of Nerve and Muscle - 2024Document84 pagesCellular Physiology of Nerve and Muscle - 2024Bilgehan BölekNo ratings yet
- S1 OtotDocument46 pagesS1 OtotJauhar FirdausNo ratings yet
- Irfan Mir Physiology Usmle Step 1Document37 pagesIrfan Mir Physiology Usmle Step 1sammieahemdNo ratings yet
- Characteristic of Cardiac Muscle Cells - CVSK4Document36 pagesCharacteristic of Cardiac Muscle Cells - CVSK4Lydia KosasihNo ratings yet
- Synaptic Signalling PDFDocument8 pagesSynaptic Signalling PDFHyunji KimNo ratings yet
- The Raas: Renin ReleaseDocument4 pagesThe Raas: Renin ReleaseAziil LiizaNo ratings yet
- 1 Phys Sept 13 READINGAction - Potentials - Handout - 202122Document11 pages1 Phys Sept 13 READINGAction - Potentials - Handout - 202122n-gorNo ratings yet
- 15 Control and CoordinationDocument6 pages15 Control and CoordinationKevin XingNo ratings yet
- 2017 Residancy Exam JUHDocument8 pages2017 Residancy Exam JUHMohammadSAL-RawashdehNo ratings yet
- Sylfonylurea: Class Generic Trade Store NotesDocument4 pagesSylfonylurea: Class Generic Trade Store NotesMohammadSAL-RawashdehNo ratings yet
- ملخص عن حب الشبابDocument10 pagesملخص عن حب الشبابMohammadSAL-RawashdehNo ratings yet
- كتاب اسئلة جميلDocument401 pagesكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- (Mebooksfree Net) Oxf&tex&uro&sur&1stDocument1,201 pages(Mebooksfree Net) Oxf&tex&uro&sur&1stMohammadSAL-Rawashdeh100% (2)
- Urology Sample MCQ Exam eDocument5 pagesUrology Sample MCQ Exam eMohammadSAL-RawashdehNo ratings yet
- (Mebooksfree Net) Pri&pra&uro&sal&2&vol&set&2ndDocument1,235 pages(Mebooksfree Net) Pri&pra&uro&sal&2&vol&set&2ndMohammadSAL-Rawashdeh100% (1)
- Head & Neck Cancers: Prof. Igor Y. Galaychuk, MDDocument43 pagesHead & Neck Cancers: Prof. Igor Y. Galaychuk, MDMohammadSAL-RawashdehNo ratings yet
- كتاب اسئلة جميلDocument401 pagesكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- 6 - 7 - 8 Peritoneum, Pancreas, AppendixDocument134 pages6 - 7 - 8 Peritoneum, Pancreas, AppendixMohammadSAL-RawashdehNo ratings yet
- Atlas 4 دائرة معارف طبية Reduced PDFDocument316 pagesAtlas 4 دائرة معارف طبية Reduced PDFMohammadSAL-RawashdehNo ratings yet
- Malignant Melanoma and Skin Cancer: Igor Y. Galaychuk, MD, DSCDocument53 pagesMalignant Melanoma and Skin Cancer: Igor Y. Galaychuk, MD, DSCMohammadSAL-RawashdehNo ratings yet
- Oral Cancer: Oral Cancer Is A Subtype of Head and Neck Cancer, Is Any Cancerous Tissue Growth Located in The Oral CavityDocument38 pagesOral Cancer: Oral Cancer Is A Subtype of Head and Neck Cancer, Is Any Cancerous Tissue Growth Located in The Oral CavityMohammadSAL-RawashdehNo ratings yet
- Human Immunodeficiency Virus (HIV) : Mohammad Al-Rawashdeh 54-5th CourseDocument39 pagesHuman Immunodeficiency Virus (HIV) : Mohammad Al-Rawashdeh 54-5th CourseMohammadSAL-RawashdehNo ratings yet
- The Neuromuscular Junction: Page 1. Introduction Page 2. GoalsDocument3 pagesThe Neuromuscular Junction: Page 1. Introduction Page 2. GoalsSteve EstebanNo ratings yet
- Action Potential ConductionDocument9 pagesAction Potential ConductiondvoyevodNo ratings yet
- Test Bank For Guyton and Hall Textbook of Medical Physiology 13th Edition by John e Hall 005 2Document10 pagesTest Bank For Guyton and Hall Textbook of Medical Physiology 13th Edition by John e Hall 005 2courtneyriveraefjpadcmyx100% (24)
- Acls Algorithms Com ChecklistDocument1 pageAcls Algorithms Com ChecklistAlexandre CastroNo ratings yet
- Cardiovascular System: (Review)Document42 pagesCardiovascular System: (Review)Leichel AlbertoNo ratings yet
- Head-To-Toe Checklist: Beautiful Nursing LLCDocument4 pagesHead-To-Toe Checklist: Beautiful Nursing LLCcarlyNo ratings yet
- MKSAP Questions: Intern ReportDocument37 pagesMKSAP Questions: Intern Reportfidelurtecho4881No ratings yet
- Anatomy Reviewer Nervous SystemDocument4 pagesAnatomy Reviewer Nervous SystemCristinNo ratings yet
- "My Neck Feels Stiff and There's Pain Coming From It. Every Time I Move It, It Only Gets Worse." As Stated by TheDocument4 pages"My Neck Feels Stiff and There's Pain Coming From It. Every Time I Move It, It Only Gets Worse." As Stated by TheCassey CuregNo ratings yet
- MetcovazinDocument24 pagesMetcovazinNiko rupokoNo ratings yet
- Unit 13 - Coordination and Response: Cambridge Biology iGCSEDocument58 pagesUnit 13 - Coordination and Response: Cambridge Biology iGCSEMirani R100% (1)
- All Life Begins With A Single - .: A) Organ B) Microbe C) Tissue D) CellDocument18 pagesAll Life Begins With A Single - .: A) Organ B) Microbe C) Tissue D) CellRonalynAlonsabeBernadasNo ratings yet
- How To Keep Awake Without CoffeeDocument2 pagesHow To Keep Awake Without CoffeeCharmaine AlipayoNo ratings yet
- Acls EcgDocument4 pagesAcls EcgScribdTranslationsNo ratings yet
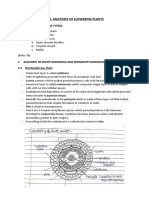
- CH6 - Anatomy of Flowering Plants - NotesDocument4 pagesCH6 - Anatomy of Flowering Plants - NotesanuminiatureNo ratings yet
- Program Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaDocument3 pagesProgram Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaHelsa EldatarinaNo ratings yet
- 2.1. Factors Affecting PhotosynthesisDocument12 pages2.1. Factors Affecting PhotosynthesisGabriel Alejandro Garcia OrregoNo ratings yet
- Sha and Self-HealingDocument18 pagesSha and Self-HealingprasadmvkNo ratings yet
- Bio1 Q2 M5 RevisedDocument13 pagesBio1 Q2 M5 RevisedgrizNo ratings yet
- Pat Physical Readiness QuestionareDocument1 pagePat Physical Readiness Questionarejohn jaycoh veranoNo ratings yet
- Circulatory WksDocument6 pagesCirculatory WksPak RisNo ratings yet
- The Kidneys and Regulation of Water and Inorganic Ions: Multiple Choice QuestionsDocument48 pagesThe Kidneys and Regulation of Water and Inorganic Ions: Multiple Choice QuestionswanderagroNo ratings yet
- Notes in Anesthesiology Dr. Azam's.... : Flow Charts, Diagrams & Important TablesDocument363 pagesNotes in Anesthesiology Dr. Azam's.... : Flow Charts, Diagrams & Important TablesThisa ArsNo ratings yet
- Fluid Status and Fluid Responsiveness PDFDocument8 pagesFluid Status and Fluid Responsiveness PDFGiselle BaiãoNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateTimo EpsiNo ratings yet
- Free Anatomy Homework HelpDocument7 pagesFree Anatomy Homework Helpbcdanetif100% (1)