Download as docx, pdf, or txt
You might also like
- Newborn Disorders - : Small For Gestational Age (Sga) NewbornDocument11 pagesNewborn Disorders - : Small For Gestational Age (Sga) Newborncayla mae carlos100% (1)
- Cancer Pathophysiology To Be EditedDocument5 pagesCancer Pathophysiology To Be EditedEyySiEffVeeNo ratings yet
- Action PlanDocument4 pagesAction PlanJosette Mae Atanacio67% (3)
- Action PlanDocument4 pagesAction PlanJosette Mae Atanacio100% (4)
- The Types of Hemorrhoidectomy Procedures IncludeDocument9 pagesThe Types of Hemorrhoidectomy Procedures IncludeKim SunooNo ratings yet
- Stress - The Different Kinds of StressDocument4 pagesStress - The Different Kinds of StressbogdanNo ratings yet
- Disorder Description Causes Signs and Symptoms Management: PretermDocument14 pagesDisorder Description Causes Signs and Symptoms Management: PretermKim SunooNo ratings yet
- High Risk Newborn ModuleDocument6 pagesHigh Risk Newborn ModuleRastie MendozaNo ratings yet
- ? - PEDIA PRELIMS Lessons 1 and 2Document8 pages? - PEDIA PRELIMS Lessons 1 and 2ysabel.mendozaNo ratings yet
- Newborn ConditionsDocument80 pagesNewborn ConditionsrigasanaorayNo ratings yet
- 1 - A Sem 9 Osce Discussion Set Mey 1Document21 pages1 - A Sem 9 Osce Discussion Set Mey 1Phoebe ThumNo ratings yet
- High-Risk Pregnancies and The Fetus Part 1 FinalDocument48 pagesHigh-Risk Pregnancies and The Fetus Part 1 FinalJill PardoNo ratings yet
- Cornell's Note 4Document5 pagesCornell's Note 4Angel BriboneriaNo ratings yet
- PT LaborDocument32 pagesPT LaborAlthea MandalNo ratings yet
- Summary of Endocrine DisordersDocument2 pagesSummary of Endocrine DisordersKrysny MontebonNo ratings yet
- NCP - Acute PainDocument4 pagesNCP - Acute PainCharmin AlegreNo ratings yet
- Drug StudyDocument4 pagesDrug StudyYVETTE CLAIRE BORRESNo ratings yet
- Kaitlin NCPDocument6 pagesKaitlin NCPJovel CortezNo ratings yet
- FGR Perinatal & Postnatal AspectsDocument48 pagesFGR Perinatal & Postnatal Aspectssalaamclinic20No ratings yet
- OBII - 16 Postterm Pregnancy - PDF Version 1Document6 pagesOBII - 16 Postterm Pregnancy - PDF Version 1Felina CabadingNo ratings yet
- Preterm Labor and Postterm PregnancyDocument33 pagesPreterm Labor and Postterm PregnancySteven IrvingNo ratings yet
- Role of Nutrition For Fetal Brain - Synergy of Certified Food v5Document19 pagesRole of Nutrition For Fetal Brain - Synergy of Certified Food v5Mediception ScienceNo ratings yet
- Nursing Notes 2nd YrDocument9 pagesNursing Notes 2nd YrMai CarbonNo ratings yet
- REVIEW Pituitary Changes and Disorders During PregnancyDocument3 pagesREVIEW Pituitary Changes and Disorders During PregnancyhantswNo ratings yet
- Module No. Date: Topic:: Cues/Questions/ Keywords Notes Preterm InfantDocument10 pagesModule No. Date: Topic:: Cues/Questions/ Keywords Notes Preterm Infantanon ymousNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care Planlala byuNo ratings yet
- Incidence of Hypoglycemia in Newborn Infants Classified by Birthweight and Gest AgeDocument10 pagesIncidence of Hypoglycemia in Newborn Infants Classified by Birthweight and Gest AgeEN Feb 22 UINo ratings yet
- Obstetrics - Fetal Growth DisorderDocument4 pagesObstetrics - Fetal Growth DisorderJonathanNo ratings yet
- 6 - Newborn DisordersDocument7 pages6 - Newborn DisordersCheng BautistaNo ratings yet
- Failure To ThriveDocument2 pagesFailure To ThrivePrabhat DevNo ratings yet
- Complication On Labor and DeliveryDocument5 pagesComplication On Labor and DeliveryMeryville JacildoNo ratings yet
- Group Q Poster 2Document1 pageGroup Q Poster 2api-622608694No ratings yet
- American Academy of Pediatrics: Term NewbornDocument10 pagesAmerican Academy of Pediatrics: Term NewbornDaniel EspinozaNo ratings yet
- IUGRDocument35 pagesIUGROlesea Morari CusnirNo ratings yet
- Intrauterine Growth Restriction (IUGR)Document29 pagesIntrauterine Growth Restriction (IUGR)Lana LocoNo ratings yet
- 125 - Fetal Biophysical ProfileDocument5 pages125 - Fetal Biophysical ProfileYuly Andrea Marquez CastañedaNo ratings yet
- University of Saint Louis: Tuguegarao City, Cagayan 3500Document4 pagesUniversity of Saint Louis: Tuguegarao City, Cagayan 3500JM RomiasNo ratings yet
- Module 7 Assignment Cortez and Salalila PDFDocument9 pagesModule 7 Assignment Cortez and Salalila PDFjennielunay00No ratings yet
- Drug Study Format 1Document3 pagesDrug Study Format 1Janeenne Fe Nicole SilvanoNo ratings yet
- Nursing Care of A Postpartal Woman and FamilyDocument44 pagesNursing Care of A Postpartal Woman and FamilyEvelyn Medina100% (1)
- Neonates Maternal Drugs Which May Adversely Affect The Newborn BabyDocument9 pagesNeonates Maternal Drugs Which May Adversely Affect The Newborn BabyAnonymousNo ratings yet
- Bondoc Drug StudyDocument3 pagesBondoc Drug StudyJan Dale BondocNo ratings yet
- Preterm LaborDocument1 pagePreterm LaborGabbi KimNo ratings yet
- Modul PBL 1 Kelompok 9aDocument34 pagesModul PBL 1 Kelompok 9aWahyuni NurdinNo ratings yet
- Intrauterine Growth in Length AND Head Circumference AS Estimated From Births AT Gestational Ages From 26 TO 42 WeeksDocument8 pagesIntrauterine Growth in Length AND Head Circumference AS Estimated From Births AT Gestational Ages From 26 TO 42 WeeksSanthosh RamasamyNo ratings yet
- Peds Exam BWDocument9 pagesPeds Exam BWaria tristayanthiNo ratings yet
- Usg Webinar Bioprofil Bayi PrintDocument36 pagesUsg Webinar Bioprofil Bayi PrintElfan WinotoNo ratings yet
- Dr. Anil Kumar Nahak 02 Argo/Phd/12 Department of Animal Reproduction, Gynaecology & Obstetrics, C.V.SC.& A.H., Ouat, BBSRDocument40 pagesDr. Anil Kumar Nahak 02 Argo/Phd/12 Department of Animal Reproduction, Gynaecology & Obstetrics, C.V.SC.& A.H., Ouat, BBSRKrushna krupa PradhanNo ratings yet
- Drug StudyDocument1 pageDrug StudyEliza PejanNo ratings yet
- NF - DR - Concept Map - Hyperemesis GravidarumDocument1 pageNF - DR - Concept Map - Hyperemesis GravidarumKyra Bianca R. FamacionNo ratings yet
- Obstetrics - MCQ - 3rd - BHMS - (Old, New, 2015)Document25 pagesObstetrics - MCQ - 3rd - BHMS - (Old, New, 2015)Anil kadamNo ratings yet
- OBII - 15 Preterm Labor and BirthDocument8 pagesOBII - 15 Preterm Labor and BirthFelina CabadingNo ratings yet
- 1 s2.0 S1751721419302301 MainDocument7 pages1 s2.0 S1751721419302301 MainLilik AnggrainiNo ratings yet
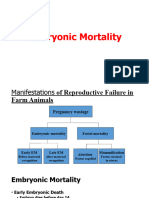
- 4th Embryonic MortalityDocument22 pages4th Embryonic MortalityjamalashrafNo ratings yet
- Postterm PregnancyDocument2 pagesPostterm PregnancyicNo ratings yet
- Comprehensive Management of Premature Baby - DR ArisDocument10 pagesComprehensive Management of Premature Baby - DR Arislimgekun63No ratings yet
- NCM 109 Problems With Power DraftDocument3 pagesNCM 109 Problems With Power DraftJP Porras AliNo ratings yet
- Intrauterine Growth Restriction: Diagnosis and ManagementDocument7 pagesIntrauterine Growth Restriction: Diagnosis and ManagementLarasati Gilang Fuzi AstutiNo ratings yet
- Resource Unit On Fetal AssessmentDocument17 pagesResource Unit On Fetal AssessmentPat Isidore SequijorNo ratings yet
- Taking History and Physical Examination in YouthDocument99 pagesTaking History and Physical Examination in Youthlinda ratna watiNo ratings yet
- Cjas2012-066 - Review Mammary Development in SwineDocument8 pagesCjas2012-066 - Review Mammary Development in Swineabdelaziz CHELIGHOUMNo ratings yet
- Your Developing Baby, Conception to Birth: Witnessing the Miraculous 9-Month JourneyFrom EverandYour Developing Baby, Conception to Birth: Witnessing the Miraculous 9-Month JourneyNo ratings yet
- PrimidoneDocument6 pagesPrimidoneKim SunooNo ratings yet
- AspirinDocument3 pagesAspirinKim SunooNo ratings yet
- Short-Term Basis To Treat Insomnia To Relieve Anxiety, Including Anxiety Before Surgery. PreanestheticDocument4 pagesShort-Term Basis To Treat Insomnia To Relieve Anxiety, Including Anxiety Before Surgery. PreanestheticKim SunooNo ratings yet
- Lesson 1.2Document2 pagesLesson 1.2Kim SunooNo ratings yet
- Generic Name: Brand Name: Route: Frequency: Before:: AE: HemorrhageDocument2 pagesGeneric Name: Brand Name: Route: Frequency: Before:: AE: HemorrhageKim SunooNo ratings yet
- Module 1 AssessmentDocument2 pagesModule 1 AssessmentKim SunooNo ratings yet
- Module - : Activity Sheet No. 1Document2 pagesModule - : Activity Sheet No. 1Kim SunooNo ratings yet
- Essay: How Values Brought Us To SuccessDocument1 pageEssay: How Values Brought Us To SuccessKim Sunoo67% (9)
- Module 1 AssessmentDocument1 pageModule 1 AssessmentKim SunooNo ratings yet
- Calixtro, LJ Contact Dermatitis NarrativeDocument2 pagesCalixtro, LJ Contact Dermatitis NarrativeKim SunooNo ratings yet
- Establishing Trustworthiness in Qualitative StudyDocument2 pagesEstablishing Trustworthiness in Qualitative StudyKim SunooNo ratings yet
- NuCM 116 MS PERIOPERATIVE MARCH 22-23 DISCUSSIONDocument17 pagesNuCM 116 MS PERIOPERATIVE MARCH 22-23 DISCUSSIONKim SunooNo ratings yet
- 1 and 11.1 ABDOMINAL LAYERS AND CESAREAN SECTIONDocument14 pages1 and 11.1 ABDOMINAL LAYERS AND CESAREAN SECTIONKim Sunoo100% (1)
- Calixtro, LJ Bacterial Infections Narrative PathophysiologyDocument14 pagesCalixtro, LJ Bacterial Infections Narrative PathophysiologyKim SunooNo ratings yet
- Calixtro, LJ Viral Infections Narrative PathophysiologyDocument29 pagesCalixtro, LJ Viral Infections Narrative PathophysiologyKim SunooNo ratings yet
- Calixtro and Bandolon Final Research ProposalDocument33 pagesCalixtro and Bandolon Final Research ProposalKim SunooNo ratings yet
- Nucm 111 Professor Date: College of NursingDocument1 pageNucm 111 Professor Date: College of NursingKim SunooNo ratings yet
- Experience of Pregnant Women in Ormoc City The Undersigned Are 3Rd YearDocument2 pagesExperience of Pregnant Women in Ormoc City The Undersigned Are 3Rd YearKim SunooNo ratings yet
- Calixtro, LJ Hypermagnesemia NarrativeDocument2 pagesCalixtro, LJ Hypermagnesemia NarrativeKim SunooNo ratings yet
- A2QVP2 TrainingDocument9 pagesA2QVP2 Trainingdanny wangNo ratings yet
- Edux110 SimDocument307 pagesEdux110 SimElijahNo ratings yet
- Turbojet EnginesDocument22 pagesTurbojet EnginesAldo SamuelNo ratings yet
- BlowOut - Relief Well OperationsDocument27 pagesBlowOut - Relief Well OperationsRandiAndhikaNo ratings yet
- Contemporary PAR Lesson 4Document23 pagesContemporary PAR Lesson 4.....No ratings yet
- Lesson 02 PDFDocument13 pagesLesson 02 PDFJeremy TohNo ratings yet
- Soal OkeDocument12 pagesSoal OkefredyNo ratings yet
- En02 PDFDocument20 pagesEn02 PDFIon VasilescuNo ratings yet
- Voltage Stability Enhancement in Power System Using STATCOM Based On Specific Coefficient Algorithm (SCA)Document7 pagesVoltage Stability Enhancement in Power System Using STATCOM Based On Specific Coefficient Algorithm (SCA)ElafanNo ratings yet
- PPAP Workbook SupplierDocument25 pagesPPAP Workbook SupplierJuan VillaNo ratings yet
- PCI EO MEG Pemex 2013 PDFDocument38 pagesPCI EO MEG Pemex 2013 PDFepesanoNo ratings yet
- Energy System EngineeringDocument116 pagesEnergy System EngineeringAila DarNo ratings yet
- FarmMachineryEquipment I ManualDocument51 pagesFarmMachineryEquipment I ManualBea SmithNo ratings yet
- Stresses in Finite Anisotropic Plate Weakened by Rectangular HoleDocument8 pagesStresses in Finite Anisotropic Plate Weakened by Rectangular Holemihir.chauhanNo ratings yet
- VIPER22ADocument21 pagesVIPER22AanawintaNo ratings yet
- Paano Magsimula NG Bangus Cage Business Part 1-2Document3 pagesPaano Magsimula NG Bangus Cage Business Part 1-2Uchiha SenjuNo ratings yet
- Electric Potential Potential Difference and Electric PotentialDocument16 pagesElectric Potential Potential Difference and Electric Potentialaliahmed123589No ratings yet
- Mulcher TSS: User Maintenance Manual - Spare PartsDocument35 pagesMulcher TSS: User Maintenance Manual - Spare PartsSerdar FildisNo ratings yet
- Dawson A J.design of Inland Wat.1950.TRANSDocument26 pagesDawson A J.design of Inland Wat.1950.TRANSKelvin XuNo ratings yet
- Princeton 112 Plus Service ManualDocument8 pagesPrinceton 112 Plus Service ManualDavid OliveiraNo ratings yet
- Momiji North Bend MenuDocument8 pagesMomiji North Bend MenuAndy MoeNo ratings yet
- Lung Sounds Auscultation - 1Document3 pagesLung Sounds Auscultation - 1George BarajazNo ratings yet
- 2017 - Electronic Control of Linear-To-circular Polarization Conversion Using A Reconfigurable MetasurfaceDocument6 pages2017 - Electronic Control of Linear-To-circular Polarization Conversion Using A Reconfigurable Metasurfaceab4azizNo ratings yet
- GO Price - escalation.GO - Ms.124.2007Document3 pagesGO Price - escalation.GO - Ms.124.2007hussainNo ratings yet
- Total Width of The ACP PanelDocument8 pagesTotal Width of The ACP PanelARYA100% (1)
- PRC General Edu A 2007Document48 pagesPRC General Edu A 2007Dhena H Rasul SabdulaNo ratings yet
- According To 2021-22 Syllabus: Icse XDocument23 pagesAccording To 2021-22 Syllabus: Icse X39-Varshit TandekarNo ratings yet
- AOSS321 L11 021209 Static StabilityDocument50 pagesAOSS321 L11 021209 Static StabilityKattia AFNo ratings yet
- EEE40003 Digital Signal and Image Processing: LAB 3: Discrete LTI SystemsDocument13 pagesEEE40003 Digital Signal and Image Processing: LAB 3: Discrete LTI SystemsKai JieNo ratings yet