
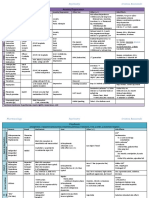
Antidepressants Comparison Guide Most Commonly Prescribed: Recommend Generics
Antidepressants Comparison Guide Most Commonly Prescribed: Recommend Generics
You might also like
- Birmingham Paper 3 PDFDocument587 pagesBirmingham Paper 3 PDFKashani DrShoaibNo ratings yet
- A Primer of AnesthesiaDocument279 pagesA Primer of AnesthesiaLiliana Năstase50% (4)
- DictationDocument6 pagesDictationlizNo ratings yet
- Dosage and Pharmacology of Antipsychotics - UpToDate ...Document4 pagesDosage and Pharmacology of Antipsychotics - UpToDate ...Dragutin PetrićNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Generics Antidepressants Comparison Chart PDFDocument2 pagesGenerics Antidepressants Comparison Chart PDFYazirNo ratings yet
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocument29 pagesPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNo ratings yet
- Psych Meds 2Document2 pagesPsych Meds 2Cole SchaferNo ratings yet
- Treatment Resistant OCD .Document55 pagesTreatment Resistant OCD .Dr viren SolankiNo ratings yet
- Transcranial Magnetic Stimulation (TMS) - AskDocument42 pagesTranscranial Magnetic Stimulation (TMS) - AskPersonal growthNo ratings yet
- Antipsychotic DrugsDocument54 pagesAntipsychotic DrugsJackNo ratings yet
- Antidepressants and AntipsychoticsDocument50 pagesAntidepressants and AntipsychoticsPintu Bhushan MitraNo ratings yet
- Current Clinical Strategies: Handbook of Psychiatric DrugsDocument72 pagesCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116No ratings yet
- Ketamine-Assisted Psychotherapy:: A Practical Guide For Medical ProvidersDocument40 pagesKetamine-Assisted Psychotherapy:: A Practical Guide For Medical ProvidersMannu MoguritoNo ratings yet
- Crisis Evaluation of The Perinatal Woman PPT. Ouellette MDDocument42 pagesCrisis Evaluation of The Perinatal Woman PPT. Ouellette MDmanjuskkNo ratings yet
- Short Guide To Psychiatric DrugsDocument17 pagesShort Guide To Psychiatric Drugsjaume1010No ratings yet
- B /G C U I R: Anti-PsychoticsDocument2 pagesB /G C U I R: Anti-PsychoticsErsy Sakti ilhamNo ratings yet
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 pagesAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonNo ratings yet
- Module 4: Motivational InterviewingDocument17 pagesModule 4: Motivational InterviewingNarges AlaieNo ratings yet
- Dual Diagnosis - Clinical and Therapeutic Aspects (Maremmani 03)Document92 pagesDual Diagnosis - Clinical and Therapeutic Aspects (Maremmani 03)antonelloveltriNo ratings yet
- Psychopharmacology NewestDocument43 pagesPsychopharmacology NewestRegina PunNo ratings yet
- Perinatal Mood and Anxiety Disorders: What Are They?Document2 pagesPerinatal Mood and Anxiety Disorders: What Are They?Maranda BartschiNo ratings yet
- Psychiatry Capstone 43020 Agitation PsychopharmacologyDocument20 pagesPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470No ratings yet
- Dowden Health Media: For Personal Use OnlyDocument8 pagesDowden Health Media: For Personal Use OnlyfernandoNo ratings yet
- APA - DSM5 - Severity Measure For Panic Disorder Adult PDFDocument3 pagesAPA - DSM5 - Severity Measure For Panic Disorder Adult PDFMelissandreNo ratings yet
- Anidepressant Drugs: Pratik KhanalDocument37 pagesAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- Quick Guide To Common Antidepressants-AdultsDocument7 pagesQuick Guide To Common Antidepressants-AdultsNicolás LescanoNo ratings yet
- Clinical Significance of A Proposed Developmental Trauma Disorder Diagnosis - Results of An International Survey of Clinicians - 2020 11 09 232956Document14 pagesClinical Significance of A Proposed Developmental Trauma Disorder Diagnosis - Results of An International Survey of Clinicians - 2020 11 09 232956abelim01100% (1)
- Biological Aspects of OCD SeminarDocument60 pagesBiological Aspects of OCD Seminarneha mattikoppaNo ratings yet
- Psych DrugsDocument3 pagesPsych DrugsSwarna BanikNo ratings yet
- Assessment in Forensic PsychiatryDocument32 pagesAssessment in Forensic PsychiatryRahelAdmasuNo ratings yet
- BenzodiazepinesDocument20 pagesBenzodiazepinesfarmasi_hmNo ratings yet
- Psychiatry Made EasyDocument14 pagesPsychiatry Made EasyD. W. S JayarathnaNo ratings yet
- Neuroanatomy For The Psychiatrist: Textbook of PsychiatryDocument37 pagesNeuroanatomy For The Psychiatrist: Textbook of Psychiatrykrysdana22No ratings yet
- Psychiatric Visit1 - AaronVer3Document1 pagePsychiatric Visit1 - AaronVer3api-3764308No ratings yet
- Update On The Efficacy of Pharmacotherapy For Social Anxiety Disorder: A Meta-AnalysisDocument12 pagesUpdate On The Efficacy of Pharmacotherapy For Social Anxiety Disorder: A Meta-AnalysisAnaaaerobios100% (1)
- PDF - Why Dont We Prescribe MAOIsDocument11 pagesPDF - Why Dont We Prescribe MAOIsSarwar Baig100% (1)
- Drugsofabuse 190812163055 PDFDocument28 pagesDrugsofabuse 190812163055 PDFMargarita AmascualNo ratings yet
- Negative Symptoms in SchizophreniaDocument15 pagesNegative Symptoms in Schizophreniasyahrizon thomasNo ratings yet
- The Effect of Venlafaxine Compared With Other Antidepressants and Placebo in The Treatment of Major DepressionDocument14 pagesThe Effect of Venlafaxine Compared With Other Antidepressants and Placebo in The Treatment of Major DepressionHakim Skoli100% (1)
- ANXIETY DISORDERS & TREATMENTS - Part 4s Feb 2020-1Document66 pagesANXIETY DISORDERS & TREATMENTS - Part 4s Feb 2020-1AnoobisNo ratings yet
- 504 - Pediatric Psychopharmacology - General PrinciplesDocument54 pages504 - Pediatric Psychopharmacology - General PrinciplesAlvaro HuidobroNo ratings yet
- Philippine College of Health Sciences Pharmacology 1Document5 pagesPhilippine College of Health Sciences Pharmacology 1Ric BarrosNo ratings yet
- Comprehensive Psychiatric EvaluationDocument5 pagesComprehensive Psychiatric EvaluationfrankieNo ratings yet
- Tauma Into To MUS Trauma 2014Document26 pagesTauma Into To MUS Trauma 2014Victor ChanNo ratings yet
- Sleep Disorders in Children and Adolescents: Deepti Shenoi MDDocument50 pagesSleep Disorders in Children and Adolescents: Deepti Shenoi MDCitra Sukri Sugesti100% (1)
- Drug List PsychopharmDocument23 pagesDrug List PsychopharmGeorge HananiaNo ratings yet
- Gilman, Ken, Kenneth, Peter - Advances Pertaining To The Pharmacology and Interactions of Irreversible Nonselective Monoamine Oxidase InhibitorsDocument9 pagesGilman, Ken, Kenneth, Peter - Advances Pertaining To The Pharmacology and Interactions of Irreversible Nonselective Monoamine Oxidase Inhibitors朗博Cuauhtlatoa100% (1)
- Anxiety/Depression: S AlprazolamDocument2 pagesAnxiety/Depression: S AlprazolamleesaNo ratings yet
- Workplace Violence PreventionDocument12 pagesWorkplace Violence PreventionAnuraj SrivastavaNo ratings yet
- Young MRSDocument2 pagesYoung MRSAnonymous KgUtPlkjNo ratings yet
- AntidepressantsDocument59 pagesAntidepressantsanon_189054600100% (2)
- Methylphenidate Side Effect Profile Is Influenced by Genetic Variation in The Attention-Deficit/Hyperactivity Disorder-Associated CES1 GeneDocument10 pagesMethylphenidate Side Effect Profile Is Influenced by Genetic Variation in The Attention-Deficit/Hyperactivity Disorder-Associated CES1 GeneMerari Lugo Ocaña100% (1)
- Antipsychotic DrugsDocument47 pagesAntipsychotic DrugsIkram UddinNo ratings yet
- Antidepressant Switching TableDocument1 pageAntidepressant Switching TableSimone BelfioriNo ratings yet
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
- Treatment Modalities For Mood DisordersDocument55 pagesTreatment Modalities For Mood DisordersGlory MimiNo ratings yet
- An Evidenced-/based Approach To Treatment - Resistant Schizophrenia FlaumDocument73 pagesAn Evidenced-/based Approach To Treatment - Resistant Schizophrenia FlaumElaNo ratings yet
- Psychiatry of Intellectual Disability: A Practical ManualFrom EverandPsychiatry of Intellectual Disability: A Practical ManualJulie P. GentileRating: 3 out of 5 stars3/5 (1)
- Gonococcal Infection in The Newborn - UpToDateDocument13 pagesGonococcal Infection in The Newborn - UpToDateCarina ColtuneacNo ratings yet
- 04 02 2021 Engagement Sur L Honneur Plus de 11 Ans Version AnglaiseDocument1 page04 02 2021 Engagement Sur L Honneur Plus de 11 Ans Version AnglaiseCarina ColtuneacNo ratings yet
- New Zealand Data Sheet: 1. Product NameDocument23 pagesNew Zealand Data Sheet: 1. Product NameCarina ColtuneacNo ratings yet
- Zoloft Article 30 Referral Annex I II III IV - enDocument52 pagesZoloft Article 30 Referral Annex I II III IV - enCarina ColtuneacNo ratings yet
- Medication Information For Parents and Teachers: Sertraline-ZoloftDocument8 pagesMedication Information For Parents and Teachers: Sertraline-ZoloftCarina ColtuneacNo ratings yet
- Study Guide Pueblo Aka Anasazi CultureDocument5 pagesStudy Guide Pueblo Aka Anasazi CultureCarina ColtuneacNo ratings yet
- Prevalence and Incidence' of Blindness Due To Age-Related Cataract in The Rural Areas of South AfricaDocument2 pagesPrevalence and Incidence' of Blindness Due To Age-Related Cataract in The Rural Areas of South AfricaCarina ColtuneacNo ratings yet
- Reading 1 Starter KitDocument19 pagesReading 1 Starter KitCarina ColtuneacNo ratings yet
- Neonatal Meningitis Due To Clostridium Neonatale: A Case ReportDocument4 pagesNeonatal Meningitis Due To Clostridium Neonatale: A Case ReportCarina ColtuneacNo ratings yet
- Physiologic and Pharmacologic Effects of CorticosteroidsDocument6 pagesPhysiologic and Pharmacologic Effects of CorticosteroidsCarina ColtuneacNo ratings yet
- Alterations in Energy Balance Following Exenatide AdministrationDocument8 pagesAlterations in Energy Balance Following Exenatide AdministrationCarina ColtuneacNo ratings yet
- Hepatorenal Syndrome - Introduction and DiagnosisDocument38 pagesHepatorenal Syndrome - Introduction and DiagnosisbornflaxNo ratings yet
- Local Anesthesia Part-1Document33 pagesLocal Anesthesia Part-1Abdul RazakNo ratings yet
- Biowaiver Monograph For Immediate-Release Solid Oral Dosage Forms: Acetylsalicylic AcidDocument15 pagesBiowaiver Monograph For Immediate-Release Solid Oral Dosage Forms: Acetylsalicylic AcidPasinduAlwisNo ratings yet
- Dha-Fmc Preferred Product List-Apr23Document297 pagesDha-Fmc Preferred Product List-Apr23JOBIN K JNo ratings yet
- MisoprostolDocument5 pagesMisoprostolkristenerika100% (2)
- Bwenger CV Updated 05 2021Document5 pagesBwenger CV Updated 05 2021api-533815355No ratings yet
- Rev Week 3-1hour - Ageing PharmaDocument21 pagesRev Week 3-1hour - Ageing Pharmaashwaaq9999No ratings yet
- Lower Respiratory Tract Infections in ChildrenDocument18 pagesLower Respiratory Tract Infections in ChildrenAmani HamoodNo ratings yet
- PSYCH Chap 15,16,17 & 24Document22 pagesPSYCH Chap 15,16,17 & 24aprilkate banagodosNo ratings yet
- Psychoactive Botanicals in Ritual Religi PDFDocument50 pagesPsychoactive Botanicals in Ritual Religi PDFStanwood CoxNo ratings yet
- 1) Misc: Neuro HY PearlsDocument2 pages1) Misc: Neuro HY Pearlsdsfan86No ratings yet
- General Medicine and Surgery For Dental Practitioners. Part 6 - Cancer, Radiotherapy and ChemotherapyDocument4 pagesGeneral Medicine and Surgery For Dental Practitioners. Part 6 - Cancer, Radiotherapy and ChemotherapyAnastasia AnNo ratings yet
- Mfds April 2016Document26 pagesMfds April 2016Joyce LimNo ratings yet
- Medication and Dosage Considerations in The Prophylaxis and Treatment of High-Atitude - IllnessDocument12 pagesMedication and Dosage Considerations in The Prophylaxis and Treatment of High-Atitude - IllnesslorenzorabbiNo ratings yet
- Written Assessment Information Booklet Website July 2018Document11 pagesWritten Assessment Information Booklet Website July 2018aaditi2mudaliarNo ratings yet
- Suicidio PDFDocument9 pagesSuicidio PDFLUCIAMELENDEZSNo ratings yet
- Advate 2005 EPAR Scientific DiscussionDocument44 pagesAdvate 2005 EPAR Scientific DiscussionbioNo ratings yet
- MCFARLANE - 2016 - ARD - EULAR-recommendations - FibromyalgiaDocument11 pagesMCFARLANE - 2016 - ARD - EULAR-recommendations - FibromyalgiaTata2666No ratings yet
- Nelson Antibioticos NEO 2023Document32 pagesNelson Antibioticos NEO 2023Lina Mariset Delgado GarzonNo ratings yet
- Medicinal Chemistry I Sovan Sarkar 186012111012Document11 pagesMedicinal Chemistry I Sovan Sarkar 186012111012Sovan SarkarNo ratings yet
- 1738 Article Text 32248 2 10 20220629 2Document11 pages1738 Article Text 32248 2 10 20220629 2samanthadoclan10No ratings yet
- How To Cite A Record On A Clinical Trials Register: Table: Examples of Citation Format Registry Example CitationDocument1 pageHow To Cite A Record On A Clinical Trials Register: Table: Examples of Citation Format Registry Example CitationSebastiánRodríguezNo ratings yet
- Full Download Book Signal Transduction Third Edition PDFDocument41 pagesFull Download Book Signal Transduction Third Edition PDFdoris.perrin870100% (29)
- P121.M3.Substance Related DisordersDocument33 pagesP121.M3.Substance Related Disordersgwen awasNo ratings yet
- Modern Management of AcneDocument5 pagesModern Management of Acnediana romeroNo ratings yet
- Drugs That Require Loading Doses Table FinalDocument1 pageDrugs That Require Loading Doses Table Finalandirio7486No ratings yet
- Hiv/Aids in Pregnancy: Hassan I.N, Mmed 4Document44 pagesHiv/Aids in Pregnancy: Hassan I.N, Mmed 4HAMIS MASOUDNo ratings yet
- Hair Loss v0.5 PathwayDocument1 pageHair Loss v0.5 PathwayAdi PurnomoNo ratings yet
- Thrombolytic Therapy For Stroke: Reconstitution and Administration Rtpa ActivaseDocument24 pagesThrombolytic Therapy For Stroke: Reconstitution and Administration Rtpa ActivaseRosalinda S CambriNo ratings yet



































































































Download as pdf or txt
You might also like
- Birmingham Paper 3 PDFDocument587 pagesBirmingham Paper 3 PDFKashani DrShoaibNo ratings yet
- A Primer of AnesthesiaDocument279 pagesA Primer of AnesthesiaLiliana Năstase50% (4)
- DictationDocument6 pagesDictationlizNo ratings yet
- Dosage and Pharmacology of Antipsychotics - UpToDate ...Document4 pagesDosage and Pharmacology of Antipsychotics - UpToDate ...Dragutin PetrićNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Generics Antidepressants Comparison Chart PDFDocument2 pagesGenerics Antidepressants Comparison Chart PDFYazirNo ratings yet
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocument29 pagesPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNo ratings yet
- Psych Meds 2Document2 pagesPsych Meds 2Cole SchaferNo ratings yet
- Treatment Resistant OCD .Document55 pagesTreatment Resistant OCD .Dr viren SolankiNo ratings yet
- Transcranial Magnetic Stimulation (TMS) - AskDocument42 pagesTranscranial Magnetic Stimulation (TMS) - AskPersonal growthNo ratings yet
- Antipsychotic DrugsDocument54 pagesAntipsychotic DrugsJackNo ratings yet
- Antidepressants and AntipsychoticsDocument50 pagesAntidepressants and AntipsychoticsPintu Bhushan MitraNo ratings yet
- Current Clinical Strategies: Handbook of Psychiatric DrugsDocument72 pagesCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116No ratings yet
- Ketamine-Assisted Psychotherapy:: A Practical Guide For Medical ProvidersDocument40 pagesKetamine-Assisted Psychotherapy:: A Practical Guide For Medical ProvidersMannu MoguritoNo ratings yet
- Crisis Evaluation of The Perinatal Woman PPT. Ouellette MDDocument42 pagesCrisis Evaluation of The Perinatal Woman PPT. Ouellette MDmanjuskkNo ratings yet
- Short Guide To Psychiatric DrugsDocument17 pagesShort Guide To Psychiatric Drugsjaume1010No ratings yet
- B /G C U I R: Anti-PsychoticsDocument2 pagesB /G C U I R: Anti-PsychoticsErsy Sakti ilhamNo ratings yet
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 pagesAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonNo ratings yet
- Module 4: Motivational InterviewingDocument17 pagesModule 4: Motivational InterviewingNarges AlaieNo ratings yet
- Dual Diagnosis - Clinical and Therapeutic Aspects (Maremmani 03)Document92 pagesDual Diagnosis - Clinical and Therapeutic Aspects (Maremmani 03)antonelloveltriNo ratings yet
- Psychopharmacology NewestDocument43 pagesPsychopharmacology NewestRegina PunNo ratings yet
- Perinatal Mood and Anxiety Disorders: What Are They?Document2 pagesPerinatal Mood and Anxiety Disorders: What Are They?Maranda BartschiNo ratings yet
- Psychiatry Capstone 43020 Agitation PsychopharmacologyDocument20 pagesPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470No ratings yet
- Dowden Health Media: For Personal Use OnlyDocument8 pagesDowden Health Media: For Personal Use OnlyfernandoNo ratings yet
- APA - DSM5 - Severity Measure For Panic Disorder Adult PDFDocument3 pagesAPA - DSM5 - Severity Measure For Panic Disorder Adult PDFMelissandreNo ratings yet
- Anidepressant Drugs: Pratik KhanalDocument37 pagesAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- Quick Guide To Common Antidepressants-AdultsDocument7 pagesQuick Guide To Common Antidepressants-AdultsNicolás LescanoNo ratings yet
- Clinical Significance of A Proposed Developmental Trauma Disorder Diagnosis - Results of An International Survey of Clinicians - 2020 11 09 232956Document14 pagesClinical Significance of A Proposed Developmental Trauma Disorder Diagnosis - Results of An International Survey of Clinicians - 2020 11 09 232956abelim01100% (1)
- Biological Aspects of OCD SeminarDocument60 pagesBiological Aspects of OCD Seminarneha mattikoppaNo ratings yet
- Psych DrugsDocument3 pagesPsych DrugsSwarna BanikNo ratings yet
- Assessment in Forensic PsychiatryDocument32 pagesAssessment in Forensic PsychiatryRahelAdmasuNo ratings yet
- BenzodiazepinesDocument20 pagesBenzodiazepinesfarmasi_hmNo ratings yet
- Psychiatry Made EasyDocument14 pagesPsychiatry Made EasyD. W. S JayarathnaNo ratings yet
- Neuroanatomy For The Psychiatrist: Textbook of PsychiatryDocument37 pagesNeuroanatomy For The Psychiatrist: Textbook of Psychiatrykrysdana22No ratings yet
- Psychiatric Visit1 - AaronVer3Document1 pagePsychiatric Visit1 - AaronVer3api-3764308No ratings yet
- Update On The Efficacy of Pharmacotherapy For Social Anxiety Disorder: A Meta-AnalysisDocument12 pagesUpdate On The Efficacy of Pharmacotherapy For Social Anxiety Disorder: A Meta-AnalysisAnaaaerobios100% (1)
- PDF - Why Dont We Prescribe MAOIsDocument11 pagesPDF - Why Dont We Prescribe MAOIsSarwar Baig100% (1)
- Drugsofabuse 190812163055 PDFDocument28 pagesDrugsofabuse 190812163055 PDFMargarita AmascualNo ratings yet
- Negative Symptoms in SchizophreniaDocument15 pagesNegative Symptoms in Schizophreniasyahrizon thomasNo ratings yet
- The Effect of Venlafaxine Compared With Other Antidepressants and Placebo in The Treatment of Major DepressionDocument14 pagesThe Effect of Venlafaxine Compared With Other Antidepressants and Placebo in The Treatment of Major DepressionHakim Skoli100% (1)
- ANXIETY DISORDERS & TREATMENTS - Part 4s Feb 2020-1Document66 pagesANXIETY DISORDERS & TREATMENTS - Part 4s Feb 2020-1AnoobisNo ratings yet
- 504 - Pediatric Psychopharmacology - General PrinciplesDocument54 pages504 - Pediatric Psychopharmacology - General PrinciplesAlvaro HuidobroNo ratings yet
- Philippine College of Health Sciences Pharmacology 1Document5 pagesPhilippine College of Health Sciences Pharmacology 1Ric BarrosNo ratings yet
- Comprehensive Psychiatric EvaluationDocument5 pagesComprehensive Psychiatric EvaluationfrankieNo ratings yet
- Tauma Into To MUS Trauma 2014Document26 pagesTauma Into To MUS Trauma 2014Victor ChanNo ratings yet
- Sleep Disorders in Children and Adolescents: Deepti Shenoi MDDocument50 pagesSleep Disorders in Children and Adolescents: Deepti Shenoi MDCitra Sukri Sugesti100% (1)
- Drug List PsychopharmDocument23 pagesDrug List PsychopharmGeorge HananiaNo ratings yet
- Gilman, Ken, Kenneth, Peter - Advances Pertaining To The Pharmacology and Interactions of Irreversible Nonselective Monoamine Oxidase InhibitorsDocument9 pagesGilman, Ken, Kenneth, Peter - Advances Pertaining To The Pharmacology and Interactions of Irreversible Nonselective Monoamine Oxidase Inhibitors朗博Cuauhtlatoa100% (1)
- Anxiety/Depression: S AlprazolamDocument2 pagesAnxiety/Depression: S AlprazolamleesaNo ratings yet
- Workplace Violence PreventionDocument12 pagesWorkplace Violence PreventionAnuraj SrivastavaNo ratings yet
- Young MRSDocument2 pagesYoung MRSAnonymous KgUtPlkjNo ratings yet
- AntidepressantsDocument59 pagesAntidepressantsanon_189054600100% (2)
- Methylphenidate Side Effect Profile Is Influenced by Genetic Variation in The Attention-Deficit/Hyperactivity Disorder-Associated CES1 GeneDocument10 pagesMethylphenidate Side Effect Profile Is Influenced by Genetic Variation in The Attention-Deficit/Hyperactivity Disorder-Associated CES1 GeneMerari Lugo Ocaña100% (1)
- Antipsychotic DrugsDocument47 pagesAntipsychotic DrugsIkram UddinNo ratings yet
- Antidepressant Switching TableDocument1 pageAntidepressant Switching TableSimone BelfioriNo ratings yet
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
- Treatment Modalities For Mood DisordersDocument55 pagesTreatment Modalities For Mood DisordersGlory MimiNo ratings yet
- An Evidenced-/based Approach To Treatment - Resistant Schizophrenia FlaumDocument73 pagesAn Evidenced-/based Approach To Treatment - Resistant Schizophrenia FlaumElaNo ratings yet
- Psychiatry of Intellectual Disability: A Practical ManualFrom EverandPsychiatry of Intellectual Disability: A Practical ManualJulie P. GentileRating: 3 out of 5 stars3/5 (1)
- Gonococcal Infection in The Newborn - UpToDateDocument13 pagesGonococcal Infection in The Newborn - UpToDateCarina ColtuneacNo ratings yet
- 04 02 2021 Engagement Sur L Honneur Plus de 11 Ans Version AnglaiseDocument1 page04 02 2021 Engagement Sur L Honneur Plus de 11 Ans Version AnglaiseCarina ColtuneacNo ratings yet
- New Zealand Data Sheet: 1. Product NameDocument23 pagesNew Zealand Data Sheet: 1. Product NameCarina ColtuneacNo ratings yet
- Zoloft Article 30 Referral Annex I II III IV - enDocument52 pagesZoloft Article 30 Referral Annex I II III IV - enCarina ColtuneacNo ratings yet
- Medication Information For Parents and Teachers: Sertraline-ZoloftDocument8 pagesMedication Information For Parents and Teachers: Sertraline-ZoloftCarina ColtuneacNo ratings yet
- Study Guide Pueblo Aka Anasazi CultureDocument5 pagesStudy Guide Pueblo Aka Anasazi CultureCarina ColtuneacNo ratings yet
- Prevalence and Incidence' of Blindness Due To Age-Related Cataract in The Rural Areas of South AfricaDocument2 pagesPrevalence and Incidence' of Blindness Due To Age-Related Cataract in The Rural Areas of South AfricaCarina ColtuneacNo ratings yet
- Reading 1 Starter KitDocument19 pagesReading 1 Starter KitCarina ColtuneacNo ratings yet
- Neonatal Meningitis Due To Clostridium Neonatale: A Case ReportDocument4 pagesNeonatal Meningitis Due To Clostridium Neonatale: A Case ReportCarina ColtuneacNo ratings yet
- Physiologic and Pharmacologic Effects of CorticosteroidsDocument6 pagesPhysiologic and Pharmacologic Effects of CorticosteroidsCarina ColtuneacNo ratings yet
- Alterations in Energy Balance Following Exenatide AdministrationDocument8 pagesAlterations in Energy Balance Following Exenatide AdministrationCarina ColtuneacNo ratings yet
- Hepatorenal Syndrome - Introduction and DiagnosisDocument38 pagesHepatorenal Syndrome - Introduction and DiagnosisbornflaxNo ratings yet
- Local Anesthesia Part-1Document33 pagesLocal Anesthesia Part-1Abdul RazakNo ratings yet
- Biowaiver Monograph For Immediate-Release Solid Oral Dosage Forms: Acetylsalicylic AcidDocument15 pagesBiowaiver Monograph For Immediate-Release Solid Oral Dosage Forms: Acetylsalicylic AcidPasinduAlwisNo ratings yet
- Dha-Fmc Preferred Product List-Apr23Document297 pagesDha-Fmc Preferred Product List-Apr23JOBIN K JNo ratings yet
- MisoprostolDocument5 pagesMisoprostolkristenerika100% (2)
- Bwenger CV Updated 05 2021Document5 pagesBwenger CV Updated 05 2021api-533815355No ratings yet
- Rev Week 3-1hour - Ageing PharmaDocument21 pagesRev Week 3-1hour - Ageing Pharmaashwaaq9999No ratings yet
- Lower Respiratory Tract Infections in ChildrenDocument18 pagesLower Respiratory Tract Infections in ChildrenAmani HamoodNo ratings yet
- PSYCH Chap 15,16,17 & 24Document22 pagesPSYCH Chap 15,16,17 & 24aprilkate banagodosNo ratings yet
- Psychoactive Botanicals in Ritual Religi PDFDocument50 pagesPsychoactive Botanicals in Ritual Religi PDFStanwood CoxNo ratings yet
- 1) Misc: Neuro HY PearlsDocument2 pages1) Misc: Neuro HY Pearlsdsfan86No ratings yet
- General Medicine and Surgery For Dental Practitioners. Part 6 - Cancer, Radiotherapy and ChemotherapyDocument4 pagesGeneral Medicine and Surgery For Dental Practitioners. Part 6 - Cancer, Radiotherapy and ChemotherapyAnastasia AnNo ratings yet
- Mfds April 2016Document26 pagesMfds April 2016Joyce LimNo ratings yet
- Medication and Dosage Considerations in The Prophylaxis and Treatment of High-Atitude - IllnessDocument12 pagesMedication and Dosage Considerations in The Prophylaxis and Treatment of High-Atitude - IllnesslorenzorabbiNo ratings yet
- Written Assessment Information Booklet Website July 2018Document11 pagesWritten Assessment Information Booklet Website July 2018aaditi2mudaliarNo ratings yet
- Suicidio PDFDocument9 pagesSuicidio PDFLUCIAMELENDEZSNo ratings yet
- Advate 2005 EPAR Scientific DiscussionDocument44 pagesAdvate 2005 EPAR Scientific DiscussionbioNo ratings yet
- MCFARLANE - 2016 - ARD - EULAR-recommendations - FibromyalgiaDocument11 pagesMCFARLANE - 2016 - ARD - EULAR-recommendations - FibromyalgiaTata2666No ratings yet
- Nelson Antibioticos NEO 2023Document32 pagesNelson Antibioticos NEO 2023Lina Mariset Delgado GarzonNo ratings yet
- Medicinal Chemistry I Sovan Sarkar 186012111012Document11 pagesMedicinal Chemistry I Sovan Sarkar 186012111012Sovan SarkarNo ratings yet
- 1738 Article Text 32248 2 10 20220629 2Document11 pages1738 Article Text 32248 2 10 20220629 2samanthadoclan10No ratings yet
- How To Cite A Record On A Clinical Trials Register: Table: Examples of Citation Format Registry Example CitationDocument1 pageHow To Cite A Record On A Clinical Trials Register: Table: Examples of Citation Format Registry Example CitationSebastiánRodríguezNo ratings yet
- Full Download Book Signal Transduction Third Edition PDFDocument41 pagesFull Download Book Signal Transduction Third Edition PDFdoris.perrin870100% (29)
- P121.M3.Substance Related DisordersDocument33 pagesP121.M3.Substance Related Disordersgwen awasNo ratings yet
- Modern Management of AcneDocument5 pagesModern Management of Acnediana romeroNo ratings yet
- Drugs That Require Loading Doses Table FinalDocument1 pageDrugs That Require Loading Doses Table Finalandirio7486No ratings yet
- Hiv/Aids in Pregnancy: Hassan I.N, Mmed 4Document44 pagesHiv/Aids in Pregnancy: Hassan I.N, Mmed 4HAMIS MASOUDNo ratings yet
- Hair Loss v0.5 PathwayDocument1 pageHair Loss v0.5 PathwayAdi PurnomoNo ratings yet
- Thrombolytic Therapy For Stroke: Reconstitution and Administration Rtpa ActivaseDocument24 pagesThrombolytic Therapy For Stroke: Reconstitution and Administration Rtpa ActivaseRosalinda S CambriNo ratings yet