Download as pdf or txt
You might also like
- Gramática AwáDocument422 pagesGramática AwáJaghu San100% (1)
- Diploma de Endodoncia Online 18-19Document7 pagesDiploma de Endodoncia Online 18-19shivaniNo ratings yet
- THE LANCET SERIES - Endocrine-Disrupting Chemicals Implications For HumanDocument16 pagesTHE LANCET SERIES - Endocrine-Disrupting Chemicals Implications For Humandiaspalma.medNo ratings yet
- EditorialDocument2 pagesEditorialsebastoto778No ratings yet
- Environmental Microbiology - 2022 - Ding - Antidepressants Promote The Spread of Antibiotic Resistance Via HorizontallyDocument16 pagesEnvironmental Microbiology - 2022 - Ding - Antidepressants Promote The Spread of Antibiotic Resistance Via HorizontallyDto de Epidemiologia Hosp J R VidalNo ratings yet
- Chemical Contaminants and Human Disease - A Summary of EvidenceDocument3 pagesChemical Contaminants and Human Disease - A Summary of Evidenceravenhotrods64No ratings yet
- Osteoarthritis: Epidemiology, Risk Factors, and PathophysiologyDocument10 pagesOsteoarthritis: Epidemiology, Risk Factors, and PathophysiologyMaryama AflahaNo ratings yet
- Jurnal Low Back PainDocument14 pagesJurnal Low Back PainHerdiana SsfcNo ratings yet
- Occurrence of Carcinoma After Prolonged Exposures To Metals in Electronics Industry: An Evidence-Based Case ReportDocument6 pagesOccurrence of Carcinoma After Prolonged Exposures To Metals in Electronics Industry: An Evidence-Based Case ReportReynardi SutantoNo ratings yet
- The Epidemiology of Low Back Pain: Best Practice & Research. Clinical Rheumatology December 2010Document14 pagesThe Epidemiology of Low Back Pain: Best Practice & Research. Clinical Rheumatology December 2010Eia RodriguezNo ratings yet
- Serum Tumor Necrosis Factor Alpha and Gene Polymorphisms in Rheumatoid Arthritis Patients in Babylon Province, IraqDocument9 pagesSerum Tumor Necrosis Factor Alpha and Gene Polymorphisms in Rheumatoid Arthritis Patients in Babylon Province, IraqDr-Abdulsamie Hassan Alta'eeNo ratings yet
- WFM April2018Document144 pagesWFM April2018Yo MeNo ratings yet
- Beyond Endometriosis Genome-Wide Association Study: From Genomics To Phenomics To The PatientDocument13 pagesBeyond Endometriosis Genome-Wide Association Study: From Genomics To Phenomics To The PatientI ENo ratings yet
- (2016) The Impact of Age On The Female Reproductive System A Pathologists Perspective. Toxicologic Pathology - VidalDocument10 pages(2016) The Impact of Age On The Female Reproductive System A Pathologists Perspective. Toxicologic Pathology - VidalleidyannegoncalvesNo ratings yet
- Parto Prematuro y EPDocument7 pagesParto Prematuro y EPFrancisco Bustamante VelásquezNo ratings yet
- A Survey On Physiotherapist Knowledge in Undersatnding The AssociDocument13 pagesA Survey On Physiotherapist Knowledge in Undersatnding The AssociIlham Meilana PutraNo ratings yet
- HHS Public AccessDocument27 pagesHHS Public AccessItamar e Waneska sem sobrenomeNo ratings yet
- Nihms 1688237Document20 pagesNihms 1688237Mohammed KhalidNo ratings yet
- Fitalatos e Risco de EndometrioseDocument20 pagesFitalatos e Risco de EndometrioseDebyNo ratings yet
- Acute Appendicitis: Modern Understanding of Pathogenesis, Diagnosis, and ManagementDocument11 pagesAcute Appendicitis: Modern Understanding of Pathogenesis, Diagnosis, and ManagementMishel Rodriguez GuzmanNo ratings yet
- JOBE 2016 - Surfactant Treatment For RDS Improves OxygenationDocument4 pagesJOBE 2016 - Surfactant Treatment For RDS Improves OxygenationRafael JustinoNo ratings yet
- NIH Public Access: Acute Lymphoblastic LeukaemiaDocument27 pagesNIH Public Access: Acute Lymphoblastic LeukaemiamfaddhilNo ratings yet
- Journal Obgyne DR - ApDocument6 pagesJournal Obgyne DR - Apoktaviana54No ratings yet
- Biomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueDocument12 pagesBiomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueWahyuning PutriNo ratings yet
- 1 s2.0 S0140673615002755 mainFINALDocument11 pages1 s2.0 S0140673615002755 mainFINALTeju SutejoNo ratings yet
- Lifestyle and Fertility: The Influence of Stress and Quality of Life On Male FertilityDocument11 pagesLifestyle and Fertility: The Influence of Stress and Quality of Life On Male FertilitySantiago CeliNo ratings yet
- Infertilidad MasculinaDocument22 pagesInfertilidad MasculinaAnaNo ratings yet
- Aneroxia NervosaDocument12 pagesAneroxia NervosaaidaNo ratings yet
- Acute Appendicitis: Modern Understanding of Pathogenesis, Diagnosis, and ManagementDocument11 pagesAcute Appendicitis: Modern Understanding of Pathogenesis, Diagnosis, and ManagementDwiNo ratings yet
- Golding, 2007Document25 pagesGolding, 2007DijuNo ratings yet
- Rheumatoid Arthritis PDFDocument8 pagesRheumatoid Arthritis PDFonny hernikNo ratings yet
- Epidemiology and Prevalence of Pelvic Organ Prolapse: ReviewDocument6 pagesEpidemiology and Prevalence of Pelvic Organ Prolapse: ReviewMahida El shafiNo ratings yet
- Langley-Evans-2015-Journal of Human Nutrition and Dietetics PDFDocument14 pagesLangley-Evans-2015-Journal of Human Nutrition and Dietetics PDFPriscila Lemasson DuranteNo ratings yet
- Multiple Sclerosis Lancet 2018Document15 pagesMultiple Sclerosis Lancet 2018Sarah Miryam CoffanoNo ratings yet
- Environmental Enteric Dysfunction and Growth Failure/Stunting in Global Child HealthDocument12 pagesEnvironmental Enteric Dysfunction and Growth Failure/Stunting in Global Child HealthNurul RamadhiniNo ratings yet
- Alzheimer's Disease and Gut MicrobiotaDocument18 pagesAlzheimer's Disease and Gut MicrobiotaMércia FiuzaNo ratings yet
- Esophageal-Diseases 2017 YgastDocument4 pagesEsophageal-Diseases 2017 YgastDayu sandraNo ratings yet
- Sono Chest Estado Arta 2023Document17 pagesSono Chest Estado Arta 2023analisador analsiadorNo ratings yet
- Obesity and Estrogen As Risk Factors For Gastroesophageal Reflux SymptomsDocument7 pagesObesity and Estrogen As Risk Factors For Gastroesophageal Reflux Symptomssalma romnalia ashshofaNo ratings yet
- RA Primer PDFDocument23 pagesRA Primer PDFVanessaNo ratings yet
- Nop2 10 2877Document9 pagesNop2 10 2877Oncología CdsNo ratings yet
- American Association For The Advancement of Science ScienceDocument8 pagesAmerican Association For The Advancement of Science Sciencekatherine monsalveNo ratings yet
- 2013 Proceedings of The Founding Meeting of SF-DOHaDDocument45 pages2013 Proceedings of The Founding Meeting of SF-DOHaDNguyễn Tiến HồngNo ratings yet
- Bland 1984Document28 pagesBland 1984Hellmann Adrian Escobar CNo ratings yet
- J SXMR 2016 02 006Document6 pagesJ SXMR 2016 02 006nmiratNo ratings yet
- Effect of Stressful Life Events On The Onset and Duration of Recurrent Aphthous StomatitisDocument5 pagesEffect of Stressful Life Events On The Onset and Duration of Recurrent Aphthous StomatitisFajar RamadhanNo ratings yet
- The Oral-Systemic Disease Connection PDFDocument2 pagesThe Oral-Systemic Disease Connection PDFJing XueNo ratings yet
- Population Based Cohort Study of Oral Contraceptive Use and Risk of DepressionDocument8 pagesPopulation Based Cohort Study of Oral Contraceptive Use and Risk of Depressionpaola andreaNo ratings yet
- Epidemiology of OsteoarthritisDocument12 pagesEpidemiology of Osteoarthritisdhimas satriaNo ratings yet
- Effects of Psychological Stress On AdverseDocument11 pagesEffects of Psychological Stress On AdverseIntan YNo ratings yet
- Biology 11 01608Document14 pagesBiology 11 01608Siti Zainab Bani PurwanaNo ratings yet
- Mechanisms of Ageing and Development: A.U. Trendelenburg, A.C. Scheuren, P. Potter, R. Müller, I. Bellantuono TDocument10 pagesMechanisms of Ageing and Development: A.U. Trendelenburg, A.C. Scheuren, P. Potter, R. Müller, I. Bellantuono TMIGUEL MORENONo ratings yet
- Bir RellDocument12 pagesBir RellGaudeamus IgiturNo ratings yet
- Nurse Fatigue Literature ReviewDocument7 pagesNurse Fatigue Literature Reviewc5nqw54q100% (1)
- Bale2010 PDFDocument6 pagesBale2010 PDFAshok KumarNo ratings yet
- Seminar: Joana Torres, Saurabh Mehandru, Jean-Frédéric Colombel, Laurent Peyrin-BirouletDocument15 pagesSeminar: Joana Torres, Saurabh Mehandru, Jean-Frédéric Colombel, Laurent Peyrin-BirouletKaren ojedaNo ratings yet
- Bjom 2018 26 5 291Document10 pagesBjom 2018 26 5 291rahmiNo ratings yet
- Breast Cancer Hypothesis: A Single Cause For The Majority of CasesDocument8 pagesBreast Cancer Hypothesis: A Single Cause For The Majority of CasessasmaldinakarNo ratings yet
- Clinical Diagnosis of Endometriosis: A Call To ActionDocument12 pagesClinical Diagnosis of Endometriosis: A Call To ActionEvan DionesiaNo ratings yet
- Laryngopharyngeal Reflux Disease: Integrative ApproachesFrom EverandLaryngopharyngeal Reflux Disease: Integrative ApproachesNausheen JamalNo ratings yet
- Choose The Correct Answer:-: 1-Acute Localized Otitis Externa (Furuncle) Is Caused byDocument2 pagesChoose The Correct Answer:-: 1-Acute Localized Otitis Externa (Furuncle) Is Caused bydiaa skamNo ratings yet
- Choose The Correct AnswerDocument2 pagesChoose The Correct Answerdiaa skamNo ratings yet
- Choose The Correct Answer::-1-Otogenic Brain Abscess NecessitatesDocument2 pagesChoose The Correct Answer::-1-Otogenic Brain Abscess Necessitatesdiaa skamNo ratings yet
- Choose The CORRECT AnswerDocument2 pagesChoose The CORRECT Answerdiaa skamNo ratings yet
- Environmental Toxicology: Arsenic PoisoningDocument1 pageEnvironmental Toxicology: Arsenic Poisoningdiaa skamNo ratings yet
- Choose The CORRECT Answer:-1 - Watery Ear Discharge Is Seen inDocument2 pagesChoose The CORRECT Answer:-1 - Watery Ear Discharge Is Seen indiaa skamNo ratings yet
- Choose The CORRECT AnswerDocument2 pagesChoose The CORRECT Answerdiaa skamNo ratings yet
- Choose The CORRECT Answer:-: ENT Department Time Allowed Name NumberDocument3 pagesChoose The CORRECT Answer:-: ENT Department Time Allowed Name Numberdiaa skamNo ratings yet
- Toxicology and Sudden DeathDocument1 pageToxicology and Sudden Deathdiaa skamNo ratings yet
- ToxocologyDocument1 pageToxocologydiaa skamNo ratings yet
- Common Drugs and PoisonsDocument1 pageCommon Drugs and Poisonsdiaa skamNo ratings yet
- Autoimmune Diseases - MicroDocument30 pagesAutoimmune Diseases - Microdiaa skamNo ratings yet
- Burnett 2019Document15 pagesBurnett 2019diaa skamNo ratings yet
- Clinical Feature: (Pathology Department Book)Document6 pagesClinical Feature: (Pathology Department Book)diaa skamNo ratings yet
- Prenatal Toxoplasma Gondii: EditorialcommentaryDocument3 pagesPrenatal Toxoplasma Gondii: Editorialcommentarydiaa skamNo ratings yet
- From Relatively Benign Disease To Rapidly Progressive and EvenDocument2 pagesFrom Relatively Benign Disease To Rapidly Progressive and Evendiaa skamNo ratings yet
- Effects of Malaria During Pregnancy On Infant Mortality in An Area of Low Malaria TransmissionDocument7 pagesEffects of Malaria During Pregnancy On Infant Mortality in An Area of Low Malaria Transmissiondiaa skamNo ratings yet
- Review Article: Chagas' Disease: Pregnancy and Congenital TransmissionDocument11 pagesReview Article: Chagas' Disease: Pregnancy and Congenital Transmissiondiaa skamNo ratings yet
- Zamecnik 2019Document9 pagesZamecnik 2019diaa skamNo ratings yet
- Toxoplasma Gondii Infection in PregnantDocument5 pagesToxoplasma Gondii Infection in Pregnantdiaa skamNo ratings yet
- (From The Surgical Laboratory of The Peter Bent Brigkara Hospital, and The Laboratory (Or Surgical Research, Harvard Medical Sckool)Document12 pages(From The Surgical Laboratory of The Peter Bent Brigkara Hospital, and The Laboratory (Or Surgical Research, Harvard Medical Sckool)diaa skamNo ratings yet
- Congenital Parasitic Infections A Review PDFDocument16 pagesCongenital Parasitic Infections A Review PDFdiaa skamNo ratings yet
- Acute Otitis Media (English)Document8 pagesAcute Otitis Media (English)diaa skamNo ratings yet
- Etiology of Autoimmune Disease: Past, Present and Future: CommentaryDocument3 pagesEtiology of Autoimmune Disease: Past, Present and Future: Commentarydiaa skamNo ratings yet
- Ent Model MCQ 2007 - 2Document9 pagesEnt Model MCQ 2007 - 2diaa skamNo ratings yet
- LOC Taxed Under ITADocument3 pagesLOC Taxed Under ITARizhatul AizatNo ratings yet
- Chart Patterns: Symmetrical Triangles The Ascending TriangleDocument8 pagesChart Patterns: Symmetrical Triangles The Ascending TriangleGene Stanley100% (1)
- Gagne VS BrunerDocument5 pagesGagne VS Bruner86mmc100% (1)
- Dewalt dw806 Manual PDFDocument28 pagesDewalt dw806 Manual PDFsanprojectNo ratings yet
- Anatomy of The Lymphatic SystemDocument76 pagesAnatomy of The Lymphatic SystemManisha RaoNo ratings yet
- Stat Fax 3300 Chemistry AnalyzerDocument2 pagesStat Fax 3300 Chemistry AnalyzermohamedNo ratings yet
- Module 5 Rle - EvaluationDocument3 pagesModule 5 Rle - EvaluationKyle VargasNo ratings yet
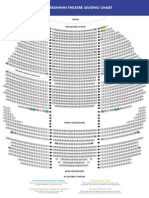
- The Gershwin Theatre Seating Chart: StageDocument1 pageThe Gershwin Theatre Seating Chart: StageCharles DavidsonNo ratings yet
- 459 - So FG13Document5 pages459 - So FG13ronni gunadi sNo ratings yet
- Scavenger Hunt AmsterdamDocument8 pagesScavenger Hunt Amsterdamkarlijn2No ratings yet
- Principles of Learning and Motivation Part 2Document3 pagesPrinciples of Learning and Motivation Part 2Tobs AnchetaNo ratings yet
- Application of IntegralsDocument14 pagesApplication of IntegralsSanjayNo ratings yet
- ComboFix Quarantined FilesDocument1 pageComboFix Quarantined FilesJoseph FoxNo ratings yet
- WITH SOLUTIONS Pipe Connection and Three ReservoirDocument46 pagesWITH SOLUTIONS Pipe Connection and Three ReservoirMark PulongbaritNo ratings yet
- Primary Connections - Heating UpDocument80 pagesPrimary Connections - Heating Upapi-391225671No ratings yet
- QuadriplegiaDocument11 pagesQuadriplegiaDr. Vinod GuptaNo ratings yet
- Gear Windage: A Review: Carol N. EastwickDocument6 pagesGear Windage: A Review: Carol N. EastwickR Prabhu SekarNo ratings yet
- DHS Coast Guard LetterDocument13 pagesDHS Coast Guard LetterThe Hill NewspaperNo ratings yet
- English 4 Q1 WK1Document3 pagesEnglish 4 Q1 WK1Ace B. SilvestreNo ratings yet
- Job Stress QuestionnaireDocument5 pagesJob Stress QuestionnaireRehman KhanNo ratings yet
- Electricity Bill Payment PDF FreeDocument16 pagesElectricity Bill Payment PDF Freekrishna mouliNo ratings yet
- 2008 Bullentin Rel. 2-DataDocument5 pages2008 Bullentin Rel. 2-DataKalai SelvanNo ratings yet
- Department of Applied Physics Applied Physics Question Bank Session - 2012-13Document4 pagesDepartment of Applied Physics Applied Physics Question Bank Session - 2012-13Sajid Ur RehmanNo ratings yet
- Excel Formulas ManualDocument8 pagesExcel Formulas ManualVidya NeemuNo ratings yet
- Iom Biffi Morin Series A B C S en en Us 6089118Document37 pagesIom Biffi Morin Series A B C S en en Us 6089118Anonymous Wu6FDjbNo ratings yet
- Sistemi Embedded AA 2012/2013: SOPC Design FlowDocument9 pagesSistemi Embedded AA 2012/2013: SOPC Design Flowmeseret sisayNo ratings yet
- Varsity KA Class & Exam Routine (Part-01)Document2 pagesVarsity KA Class & Exam Routine (Part-01)Yousuf JamilNo ratings yet
- 1.1 Nanomaterials and NanoparticlesDocument2 pages1.1 Nanomaterials and NanoparticlesDuyen75% (4)
- BELOW KNEE AMPUTATION EditDocument16 pagesBELOW KNEE AMPUTATION EditPutri AyuNo ratings yet