
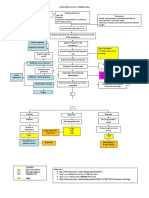
Respiratory 05 - COPD: Definition: Types For Emphysema
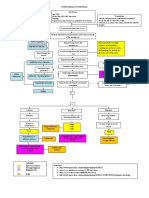
Respiratory 05 - COPD: Definition: Types For Emphysema
You might also like
- NCM 112 N LECTURE MidtermDocument42 pagesNCM 112 N LECTURE MidtermVivien IgnacioNo ratings yet
- ARDS Concept Map - BunayogDocument2 pagesARDS Concept Map - BunayogJacela Annsyle BunayogNo ratings yet
- Copd Case StudyDocument6 pagesCopd Case StudyDivine ParagasNo ratings yet
- Ineffective Airway Clearance Related To BronchospasmDocument2 pagesIneffective Airway Clearance Related To BronchospasmReylan Garcia100% (4)
- Copd MarrowDocument10 pagesCopd MarrowSACHIN JAISWALNo ratings yet
- Obstructive: Pulmonary DiseaseDocument6 pagesObstructive: Pulmonary DiseaseCarmen MargoNo ratings yet
- Centriacinar Panacinar Paraseptal Irregular Emphysema Bullous EmphysemaDocument1 pageCentriacinar Panacinar Paraseptal Irregular Emphysema Bullous EmphysemaMaryam FadahNo ratings yet
- Adventitious Breath SoundsDocument1 pageAdventitious Breath SoundsAbdullah BhattiNo ratings yet
- Chronic Bronchitis and EmphesemaDocument2 pagesChronic Bronchitis and Emphesemanursing concept maps100% (2)
- Niveoli & Ciclohale 21-22Document62 pagesNiveoli & Ciclohale 21-22Aditya RounakNo ratings yet
- Respiratory SysDocument143 pagesRespiratory Sysdiadilshad04No ratings yet
- Chronic CoughDocument6 pagesChronic CoughironNo ratings yet
- Chapter 15 Respiratory SystemDocument3 pagesChapter 15 Respiratory SystemRayumaaa100% (1)
- Pack-Years of Cigarette Smoking Is The Most HighlyDocument5 pagesPack-Years of Cigarette Smoking Is The Most HighlyIsabel CastilloNo ratings yet
- Chronic CoughDocument6 pagesChronic CoughironNo ratings yet
- Covid NCPDocument6 pagesCovid NCPNathalia Cabalse100% (2)
- Medical Surgical Nursing Lecture 234 Pages Pg. 333 566Document189 pagesMedical Surgical Nursing Lecture 234 Pages Pg. 333 566Crystal Ann TadiamonNo ratings yet
- COPDDocument3 pagesCOPDAlmera MananNo ratings yet
- Respiratory SystemDocument9 pagesRespiratory SystemYesha Del RosarioNo ratings yet
- ASTHMA CPD FINAL (Autosaved)Document74 pagesASTHMA CPD FINAL (Autosaved)Affri Dian AdiyatnaNo ratings yet
- Obstructive Airway DiseasesDocument56 pagesObstructive Airway Diseaseskalanakariyawasam99No ratings yet
- Anatomy Final pt.2Document8 pagesAnatomy Final pt.2Gladys Mae S. BañesNo ratings yet
- Asthma MNTDocument8 pagesAsthma MNTMaria YaseenNo ratings yet
- Sputum AnalysisDocument2 pagesSputum AnalysisanonacadsNo ratings yet
- zpms1207 Respiratory-SystemDocument4 pageszpms1207 Respiratory-Systemamysong772No ratings yet
- Copd - Midterm NotesDocument2 pagesCopd - Midterm NotesInday BertaNo ratings yet
- Chapter 15 Respiratory System (2nd Edition)Document54 pagesChapter 15 Respiratory System (2nd Edition)vs7ksgrj8pNo ratings yet
- 50 DiseasesDocument44 pages50 DiseasesJewenson SalvadorNo ratings yet
- Drugs Used in AsthmaDocument12 pagesDrugs Used in AsthmaCarlos Enrique Acasiete TresierraNo ratings yet
- Respiratory MedicineDocument49 pagesRespiratory MedicinemuhamedNo ratings yet
- Pathofisiologi Copd: Iritasi BroncialDocument3 pagesPathofisiologi Copd: Iritasi BroncialDellavia EntaNo ratings yet
- Medical Surgical Nursing Lecture 234 Pages Pg. 333 566Document242 pagesMedical Surgical Nursing Lecture 234 Pages Pg. 333 566ShiraishiNo ratings yet
- Respiratory 1Document28 pagesRespiratory 1Howell MathewNo ratings yet
- Respiratory System: Larynx EpiglottisDocument12 pagesRespiratory System: Larynx Epiglottisangel sychingNo ratings yet
- Ncma 113Document4 pagesNcma 113Wonie booNo ratings yet
- PBQsDocument18 pagesPBQsShashanka PoudelNo ratings yet
- Nursing Care of Clients With Ventilation DisordersDocument11 pagesNursing Care of Clients With Ventilation DisordersVinzii DrtNo ratings yet
- Dont BreathDocument43 pagesDont BreathDhruv GoswamiNo ratings yet
- Name: - I. Tabulate The Differences Between Obstructive Versus Restrictive Lung DiseaseDocument13 pagesName: - I. Tabulate The Differences Between Obstructive Versus Restrictive Lung DiseaseLeandrew MagistradoNo ratings yet
- Respiratory PhysiologyDocument16 pagesRespiratory PhysiologyYsabel Salvador Dychinco100% (1)
- Aljean Altheo L. Artillo BSN-3B 1. What Are The Pathophysiologies of Chronic Obstructive Pulmonary Disease (COPD) ?Document2 pagesAljean Altheo L. Artillo BSN-3B 1. What Are The Pathophysiologies of Chronic Obstructive Pulmonary Disease (COPD) ?Al TheóNo ratings yet
- Anatomi Dan Fisiologi Paru: By: Amelia LorensiaDocument21 pagesAnatomi Dan Fisiologi Paru: By: Amelia LorensiaEjuneeNo ratings yet
- Bullous Lung DiseaseDocument6 pagesBullous Lung DiseaseSrujanaNo ratings yet
- Ast 2Document17 pagesAst 2AbuAbdullah KhanNo ratings yet
- Asthm 2Document34 pagesAsthm 2AbuAbdullah KhanNo ratings yet
- Pa Tho PhysiologyDocument1 pagePa Tho PhysiologyJoanne JelicaNo ratings yet
- Abnormal Chest FindingsDocument5 pagesAbnormal Chest FindingsAbishek Prince100% (1)
- 109 - Obstructive Lung DiseasesDocument8 pages109 - Obstructive Lung DiseasesCharisa Antonette HuelvaNo ratings yet
- 3 2021 05 1012 46 42 AmDocument43 pages3 2021 05 1012 46 42 Amwardahafif00No ratings yet
- 1 Respiratory PDFDocument13 pages1 Respiratory PDFali.j.alhassaniNo ratings yet
- Upper Airway InfectionsDocument5 pagesUpper Airway InfectionsTreesa LouiseNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaAzria John DemetriNo ratings yet
- Patho of COPD and CorP NewDocument5 pagesPatho of COPD and CorP NewInchan Montesines100% (1)
- Chapter 15 Lung Pathology ErnieDocument20 pagesChapter 15 Lung Pathology ErnieZandra Lyn AlundayNo ratings yet
- RespDocument23 pagesRespAyessa D. RosalitaNo ratings yet
- 2 - CopdDocument40 pages2 - CopdFathima MulthazimaNo ratings yet
- Sheet - Respiratory ExaminationDocument11 pagesSheet - Respiratory ExaminationbakesamiNo ratings yet
- Anatomi Dan Fisiologi Paru: By: Amelia LorensiaDocument21 pagesAnatomi Dan Fisiologi Paru: By: Amelia LorensiaPia RohdinaNo ratings yet
- Anatomi Dan Fisiologi Paru: By: Amelia LorensiaDocument21 pagesAnatomi Dan Fisiologi Paru: By: Amelia LorensiaAbiReknantoNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJuneNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Respiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic MutationDocument2 pagesRespiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic Mutationkamil malikNo ratings yet
- Respiratory 02 - Pulmonary Tuberculosis: PathogenesisDocument3 pagesRespiratory 02 - Pulmonary Tuberculosis: Pathogenesiskamil malikNo ratings yet
- Drugs For AsthmaDocument1 pageDrugs For Asthmakamil malikNo ratings yet
- Ehambutol Inhibits Mycobacterial Arabinosyltransferase Streptomcin Binds To 16s rRNA of BacteriaDocument1 pageEhambutol Inhibits Mycobacterial Arabinosyltransferase Streptomcin Binds To 16s rRNA of Bacteriakamil malikNo ratings yet
- Electrical Impedance Tomography: Eduardo L.V. Costa, Raul Gonzalez Lima and Marcelo B.P. AmatoDocument7 pagesElectrical Impedance Tomography: Eduardo L.V. Costa, Raul Gonzalez Lima and Marcelo B.P. Amatojorgeluis.unknownman667No ratings yet
- Doctors Example - 001Document15 pagesDoctors Example - 001Vishal NannaNo ratings yet
- The Asthma-COPD Overlap Syndrome - NEJMDocument1 pageThe Asthma-COPD Overlap Syndrome - NEJMRicardoNo ratings yet
- Trilogy Clinical Manual Addendum: Mouthpiece Ventilation (MPV)Document52 pagesTrilogy Clinical Manual Addendum: Mouthpiece Ventilation (MPV)Rodrigo GutierrezNo ratings yet
- Assessment of Thorax and LungsDocument15 pagesAssessment of Thorax and LungsmakathrinasanchezNo ratings yet
- Respiratory Therapist Skills ChecklistDocument3 pagesRespiratory Therapist Skills Checklisthealth careNo ratings yet
- Things To Know About Life Sustaining Treatment4Document3 pagesThings To Know About Life Sustaining Treatment4DurgaPrasadNo ratings yet
- Novilyn C. Pataray BSN - Ii Acute Epiglottis: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Acute Epiglottis: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- Bronchiolitis Seminar.Document15 pagesBronchiolitis Seminar.Sudha YadavNo ratings yet
- Lung Volumes Lab ReportDocument11 pagesLung Volumes Lab ReportYani ManuelNo ratings yet
- Bellavista 1000 ICU enDocument12 pagesBellavista 1000 ICU enAchmad Bagus Dwi SNo ratings yet
- 07 - Lung Sounds - LearnerDocument2 pages07 - Lung Sounds - LearnerRafaelNo ratings yet
- En NV8 V1.3Document4 pagesEn NV8 V1.3Declan WangNo ratings yet
- 柳奇學姐提供的Mode of Mechanical VentilatorDocument79 pages柳奇學姐提供的Mode of Mechanical Ventilatorapi-25944730100% (10)
- Pneumothorax, Tension and TraumaticDocument24 pagesPneumothorax, Tension and TraumaticSatria WibawaNo ratings yet
- EXAM RRTPracticeQuestionsDocument30 pagesEXAM RRTPracticeQuestionsGustavo OlguinNo ratings yet
- BIO270 Written AssignmentDocument3 pagesBIO270 Written AssignmentMirza KarmilaNo ratings yet
- Convention Modes of Mechanical Ventilation. DR - purwOKODocument53 pagesConvention Modes of Mechanical Ventilation. DR - purwOKOIsnia WahibNo ratings yet
- Respiratory Assessment (IPPA) : Check Tactile FremitusDocument5 pagesRespiratory Assessment (IPPA) : Check Tactile FremitusMabesNo ratings yet
- Pneumothorax (Collapsed Lung) : What Is A Pneumothorax?Document17 pagesPneumothorax (Collapsed Lung) : What Is A Pneumothorax?Hazel EstayanNo ratings yet
- Clinical Aspects of PneumothoraxDocument3 pagesClinical Aspects of PneumothoraxelisabethNo ratings yet
- FEU Review Pre Board Exam 2016 Respi CareDocument11 pagesFEU Review Pre Board Exam 2016 Respi CareDharlyn MungcalNo ratings yet
- Treatment of ARDSDocument15 pagesTreatment of ARDSf3wlNo ratings yet
- Inhalation Injury and Systemic IntoxicationDocument7 pagesInhalation Injury and Systemic IntoxicationDaniel LesmanaNo ratings yet
- Flexible Bronchoscopy 4Th Edition Ko Pen Wang Full Chapter PDFDocument69 pagesFlexible Bronchoscopy 4Th Edition Ko Pen Wang Full Chapter PDFemmarbaf100% (5)
- Respiratory Treatments Poster June2022v1Document2 pagesRespiratory Treatments Poster June2022v1Jade ProvidenceNo ratings yet
- Bronchial AsthmaDocument46 pagesBronchial AsthmaKhor Kee GuanNo ratings yet
- DR Josephine Ojoo Senior Lecturer Maseno University: MBCHB FRCP CCST (Resp) Dip Hiv MedDocument47 pagesDR Josephine Ojoo Senior Lecturer Maseno University: MBCHB FRCP CCST (Resp) Dip Hiv MedMalueth AnguiNo ratings yet




























































































Download as docx, pdf, or txt
You might also like
- NCM 112 N LECTURE MidtermDocument42 pagesNCM 112 N LECTURE MidtermVivien IgnacioNo ratings yet
- ARDS Concept Map - BunayogDocument2 pagesARDS Concept Map - BunayogJacela Annsyle BunayogNo ratings yet
- Copd Case StudyDocument6 pagesCopd Case StudyDivine ParagasNo ratings yet
- Ineffective Airway Clearance Related To BronchospasmDocument2 pagesIneffective Airway Clearance Related To BronchospasmReylan Garcia100% (4)
- Copd MarrowDocument10 pagesCopd MarrowSACHIN JAISWALNo ratings yet
- Obstructive: Pulmonary DiseaseDocument6 pagesObstructive: Pulmonary DiseaseCarmen MargoNo ratings yet
- Centriacinar Panacinar Paraseptal Irregular Emphysema Bullous EmphysemaDocument1 pageCentriacinar Panacinar Paraseptal Irregular Emphysema Bullous EmphysemaMaryam FadahNo ratings yet
- Adventitious Breath SoundsDocument1 pageAdventitious Breath SoundsAbdullah BhattiNo ratings yet
- Chronic Bronchitis and EmphesemaDocument2 pagesChronic Bronchitis and Emphesemanursing concept maps100% (2)
- Niveoli & Ciclohale 21-22Document62 pagesNiveoli & Ciclohale 21-22Aditya RounakNo ratings yet
- Respiratory SysDocument143 pagesRespiratory Sysdiadilshad04No ratings yet
- Chronic CoughDocument6 pagesChronic CoughironNo ratings yet
- Chapter 15 Respiratory SystemDocument3 pagesChapter 15 Respiratory SystemRayumaaa100% (1)
- Pack-Years of Cigarette Smoking Is The Most HighlyDocument5 pagesPack-Years of Cigarette Smoking Is The Most HighlyIsabel CastilloNo ratings yet
- Chronic CoughDocument6 pagesChronic CoughironNo ratings yet
- Covid NCPDocument6 pagesCovid NCPNathalia Cabalse100% (2)
- Medical Surgical Nursing Lecture 234 Pages Pg. 333 566Document189 pagesMedical Surgical Nursing Lecture 234 Pages Pg. 333 566Crystal Ann TadiamonNo ratings yet
- COPDDocument3 pagesCOPDAlmera MananNo ratings yet
- Respiratory SystemDocument9 pagesRespiratory SystemYesha Del RosarioNo ratings yet
- ASTHMA CPD FINAL (Autosaved)Document74 pagesASTHMA CPD FINAL (Autosaved)Affri Dian AdiyatnaNo ratings yet
- Obstructive Airway DiseasesDocument56 pagesObstructive Airway Diseaseskalanakariyawasam99No ratings yet
- Anatomy Final pt.2Document8 pagesAnatomy Final pt.2Gladys Mae S. BañesNo ratings yet
- Asthma MNTDocument8 pagesAsthma MNTMaria YaseenNo ratings yet
- Sputum AnalysisDocument2 pagesSputum AnalysisanonacadsNo ratings yet
- zpms1207 Respiratory-SystemDocument4 pageszpms1207 Respiratory-Systemamysong772No ratings yet
- Copd - Midterm NotesDocument2 pagesCopd - Midterm NotesInday BertaNo ratings yet
- Chapter 15 Respiratory System (2nd Edition)Document54 pagesChapter 15 Respiratory System (2nd Edition)vs7ksgrj8pNo ratings yet
- 50 DiseasesDocument44 pages50 DiseasesJewenson SalvadorNo ratings yet
- Drugs Used in AsthmaDocument12 pagesDrugs Used in AsthmaCarlos Enrique Acasiete TresierraNo ratings yet
- Respiratory MedicineDocument49 pagesRespiratory MedicinemuhamedNo ratings yet
- Pathofisiologi Copd: Iritasi BroncialDocument3 pagesPathofisiologi Copd: Iritasi BroncialDellavia EntaNo ratings yet
- Medical Surgical Nursing Lecture 234 Pages Pg. 333 566Document242 pagesMedical Surgical Nursing Lecture 234 Pages Pg. 333 566ShiraishiNo ratings yet
- Respiratory 1Document28 pagesRespiratory 1Howell MathewNo ratings yet
- Respiratory System: Larynx EpiglottisDocument12 pagesRespiratory System: Larynx Epiglottisangel sychingNo ratings yet
- Ncma 113Document4 pagesNcma 113Wonie booNo ratings yet
- PBQsDocument18 pagesPBQsShashanka PoudelNo ratings yet
- Nursing Care of Clients With Ventilation DisordersDocument11 pagesNursing Care of Clients With Ventilation DisordersVinzii DrtNo ratings yet
- Dont BreathDocument43 pagesDont BreathDhruv GoswamiNo ratings yet
- Name: - I. Tabulate The Differences Between Obstructive Versus Restrictive Lung DiseaseDocument13 pagesName: - I. Tabulate The Differences Between Obstructive Versus Restrictive Lung DiseaseLeandrew MagistradoNo ratings yet
- Respiratory PhysiologyDocument16 pagesRespiratory PhysiologyYsabel Salvador Dychinco100% (1)
- Aljean Altheo L. Artillo BSN-3B 1. What Are The Pathophysiologies of Chronic Obstructive Pulmonary Disease (COPD) ?Document2 pagesAljean Altheo L. Artillo BSN-3B 1. What Are The Pathophysiologies of Chronic Obstructive Pulmonary Disease (COPD) ?Al TheóNo ratings yet
- Anatomi Dan Fisiologi Paru: By: Amelia LorensiaDocument21 pagesAnatomi Dan Fisiologi Paru: By: Amelia LorensiaEjuneeNo ratings yet
- Bullous Lung DiseaseDocument6 pagesBullous Lung DiseaseSrujanaNo ratings yet
- Ast 2Document17 pagesAst 2AbuAbdullah KhanNo ratings yet
- Asthm 2Document34 pagesAsthm 2AbuAbdullah KhanNo ratings yet
- Pa Tho PhysiologyDocument1 pagePa Tho PhysiologyJoanne JelicaNo ratings yet
- Abnormal Chest FindingsDocument5 pagesAbnormal Chest FindingsAbishek Prince100% (1)
- 109 - Obstructive Lung DiseasesDocument8 pages109 - Obstructive Lung DiseasesCharisa Antonette HuelvaNo ratings yet
- 3 2021 05 1012 46 42 AmDocument43 pages3 2021 05 1012 46 42 Amwardahafif00No ratings yet
- 1 Respiratory PDFDocument13 pages1 Respiratory PDFali.j.alhassaniNo ratings yet
- Upper Airway InfectionsDocument5 pagesUpper Airway InfectionsTreesa LouiseNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaAzria John DemetriNo ratings yet
- Patho of COPD and CorP NewDocument5 pagesPatho of COPD and CorP NewInchan Montesines100% (1)
- Chapter 15 Lung Pathology ErnieDocument20 pagesChapter 15 Lung Pathology ErnieZandra Lyn AlundayNo ratings yet
- RespDocument23 pagesRespAyessa D. RosalitaNo ratings yet
- 2 - CopdDocument40 pages2 - CopdFathima MulthazimaNo ratings yet
- Sheet - Respiratory ExaminationDocument11 pagesSheet - Respiratory ExaminationbakesamiNo ratings yet
- Anatomi Dan Fisiologi Paru: By: Amelia LorensiaDocument21 pagesAnatomi Dan Fisiologi Paru: By: Amelia LorensiaPia RohdinaNo ratings yet
- Anatomi Dan Fisiologi Paru: By: Amelia LorensiaDocument21 pagesAnatomi Dan Fisiologi Paru: By: Amelia LorensiaAbiReknantoNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJuneNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Respiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic MutationDocument2 pagesRespiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic Mutationkamil malikNo ratings yet
- Respiratory 02 - Pulmonary Tuberculosis: PathogenesisDocument3 pagesRespiratory 02 - Pulmonary Tuberculosis: Pathogenesiskamil malikNo ratings yet
- Drugs For AsthmaDocument1 pageDrugs For Asthmakamil malikNo ratings yet
- Ehambutol Inhibits Mycobacterial Arabinosyltransferase Streptomcin Binds To 16s rRNA of BacteriaDocument1 pageEhambutol Inhibits Mycobacterial Arabinosyltransferase Streptomcin Binds To 16s rRNA of Bacteriakamil malikNo ratings yet
- Electrical Impedance Tomography: Eduardo L.V. Costa, Raul Gonzalez Lima and Marcelo B.P. AmatoDocument7 pagesElectrical Impedance Tomography: Eduardo L.V. Costa, Raul Gonzalez Lima and Marcelo B.P. Amatojorgeluis.unknownman667No ratings yet
- Doctors Example - 001Document15 pagesDoctors Example - 001Vishal NannaNo ratings yet
- The Asthma-COPD Overlap Syndrome - NEJMDocument1 pageThe Asthma-COPD Overlap Syndrome - NEJMRicardoNo ratings yet
- Trilogy Clinical Manual Addendum: Mouthpiece Ventilation (MPV)Document52 pagesTrilogy Clinical Manual Addendum: Mouthpiece Ventilation (MPV)Rodrigo GutierrezNo ratings yet
- Assessment of Thorax and LungsDocument15 pagesAssessment of Thorax and LungsmakathrinasanchezNo ratings yet
- Respiratory Therapist Skills ChecklistDocument3 pagesRespiratory Therapist Skills Checklisthealth careNo ratings yet
- Things To Know About Life Sustaining Treatment4Document3 pagesThings To Know About Life Sustaining Treatment4DurgaPrasadNo ratings yet
- Novilyn C. Pataray BSN - Ii Acute Epiglottis: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Acute Epiglottis: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- Bronchiolitis Seminar.Document15 pagesBronchiolitis Seminar.Sudha YadavNo ratings yet
- Lung Volumes Lab ReportDocument11 pagesLung Volumes Lab ReportYani ManuelNo ratings yet
- Bellavista 1000 ICU enDocument12 pagesBellavista 1000 ICU enAchmad Bagus Dwi SNo ratings yet
- 07 - Lung Sounds - LearnerDocument2 pages07 - Lung Sounds - LearnerRafaelNo ratings yet
- En NV8 V1.3Document4 pagesEn NV8 V1.3Declan WangNo ratings yet
- 柳奇學姐提供的Mode of Mechanical VentilatorDocument79 pages柳奇學姐提供的Mode of Mechanical Ventilatorapi-25944730100% (10)
- Pneumothorax, Tension and TraumaticDocument24 pagesPneumothorax, Tension and TraumaticSatria WibawaNo ratings yet
- EXAM RRTPracticeQuestionsDocument30 pagesEXAM RRTPracticeQuestionsGustavo OlguinNo ratings yet
- BIO270 Written AssignmentDocument3 pagesBIO270 Written AssignmentMirza KarmilaNo ratings yet
- Convention Modes of Mechanical Ventilation. DR - purwOKODocument53 pagesConvention Modes of Mechanical Ventilation. DR - purwOKOIsnia WahibNo ratings yet
- Respiratory Assessment (IPPA) : Check Tactile FremitusDocument5 pagesRespiratory Assessment (IPPA) : Check Tactile FremitusMabesNo ratings yet
- Pneumothorax (Collapsed Lung) : What Is A Pneumothorax?Document17 pagesPneumothorax (Collapsed Lung) : What Is A Pneumothorax?Hazel EstayanNo ratings yet
- Clinical Aspects of PneumothoraxDocument3 pagesClinical Aspects of PneumothoraxelisabethNo ratings yet
- FEU Review Pre Board Exam 2016 Respi CareDocument11 pagesFEU Review Pre Board Exam 2016 Respi CareDharlyn MungcalNo ratings yet
- Treatment of ARDSDocument15 pagesTreatment of ARDSf3wlNo ratings yet
- Inhalation Injury and Systemic IntoxicationDocument7 pagesInhalation Injury and Systemic IntoxicationDaniel LesmanaNo ratings yet
- Flexible Bronchoscopy 4Th Edition Ko Pen Wang Full Chapter PDFDocument69 pagesFlexible Bronchoscopy 4Th Edition Ko Pen Wang Full Chapter PDFemmarbaf100% (5)
- Respiratory Treatments Poster June2022v1Document2 pagesRespiratory Treatments Poster June2022v1Jade ProvidenceNo ratings yet
- Bronchial AsthmaDocument46 pagesBronchial AsthmaKhor Kee GuanNo ratings yet
- DR Josephine Ojoo Senior Lecturer Maseno University: MBCHB FRCP CCST (Resp) Dip Hiv MedDocument47 pagesDR Josephine Ojoo Senior Lecturer Maseno University: MBCHB FRCP CCST (Resp) Dip Hiv MedMalueth AnguiNo ratings yet