Download as docx, pdf, or txt
You might also like
- NCP For Subarachnoid HemorrhageDocument4 pagesNCP For Subarachnoid HemorrhageJoan Rose Rendon-Hung78% (18)
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- Nursing Care PlanDocument4 pagesNursing Care Planmanu_gutierrez0891% (11)
- Nursing Care Plan For HypertensionDocument4 pagesNursing Care Plan For HypertensionKathleen Dimacali100% (2)
- NCP - Decreased Intracranial Adaptive Capacity R/T Space - Occupying Lesion.Document1 pageNCP - Decreased Intracranial Adaptive Capacity R/T Space - Occupying Lesion.Carl Elexer Cuyugan Ano100% (6)
- Nursing Care Plan For Palliative Care Nursing NotesDocument2 pagesNursing Care Plan For Palliative Care Nursing NotesblaireNo ratings yet
- NCP #1 Ineffective Cerebral Tissue PerfusionDocument4 pagesNCP #1 Ineffective Cerebral Tissue PerfusionsteffiNo ratings yet
- NCP Ineffective Cerebral Tissue Perfusion STROKEDocument3 pagesNCP Ineffective Cerebral Tissue Perfusion STROKEMa. Elaine Carla TatingNo ratings yet
- Hypertension Nursing Care PlanDocument3 pagesHypertension Nursing Care Plangeng gengNo ratings yet
- HALOPERIDOL Drug StudyDocument2 pagesHALOPERIDOL Drug Studyanreilegarde89% (9)
- Nursing Care Plan For HypertensionDocument5 pagesNursing Care Plan For HypertensionJessy MalloNo ratings yet
- Decreased Cardiac Output EclampsiaDocument6 pagesDecreased Cardiac Output EclampsiaNursesLabs.com100% (7)
- Urinary Tract Infection Nursing-Care-PlanDocument3 pagesUrinary Tract Infection Nursing-Care-PlanRnspeakcomNo ratings yet
- Perforations & ManagementDocument163 pagesPerforations & ManagementAPARNA AARATHI SREEKUMARNo ratings yet
- Paul W. Hodges, Jacek Cholewicki and Jaap H Van Dieen (Eds.) - Spinal Control. The Rehabilitation of Back Pain (2012)Document309 pagesPaul W. Hodges, Jacek Cholewicki and Jaap H Van Dieen (Eds.) - Spinal Control. The Rehabilitation of Back Pain (2012)jaime0% (1)
- Case Study 1 NCPDocument3 pagesCase Study 1 NCPJayson SamonteNo ratings yet
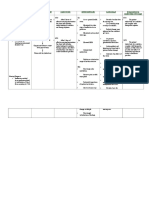
- Assessment Nursing Diagnosis Goals/ Objectives Nursing Interventions Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Goals/ Objectives Nursing Interventions Rationale EvaluationGene Chavez AppleNo ratings yet
- Nanda NCP BasedDocument14 pagesNanda NCP Baseddeliejoyce100% (1)
- Nursing Care Plan: Group 4-Open Wound Head Injury After Debris FallDocument3 pagesNursing Care Plan: Group 4-Open Wound Head Injury After Debris FallNicole Villanueva, BSN - Level 3ANo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermDocument3 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermMicaela CrisostomoNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanMel Izhra N. MargateNo ratings yet
- NS3 Ncp-FdarDocument5 pagesNS3 Ncp-FdarArdiene Shallouvette GamosoNo ratings yet
- Actual Nursing Care Plan #1: Deficient Fluid VolumeDocument7 pagesActual Nursing Care Plan #1: Deficient Fluid VolumeAubrey SungaNo ratings yet
- Risk For Peripheral Neurodysfunction NCPDocument3 pagesRisk For Peripheral Neurodysfunction NCPLeonardo Martin FrivaldoNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveDocument2 pagesNursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveFreisanChenMandumotanNo ratings yet
- CCU NCP Week 2Document4 pagesCCU NCP Week 2April Kate BanagodosNo ratings yet
- NCPDocument6 pagesNCPJane CasiquinNo ratings yet
- Hypertension Nursing Care PlanDocument3 pagesHypertension Nursing Care PlanAsylla PajijiNo ratings yet
- Kami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedDocument4 pagesKami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedKoleen Lhyte T. UYNo ratings yet
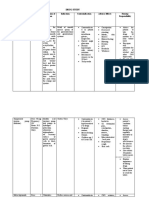
- Data Nursing Diagnos IS Scientific Backgrou ND Goal/Objective Nursing Interventions Rationale EvaluationDocument4 pagesData Nursing Diagnos IS Scientific Backgrou ND Goal/Objective Nursing Interventions Rationale EvaluationDienizs LabiniNo ratings yet
- Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7Document2 pagesIneffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7dana100% (4)
- Postop Actual &potential NCPDocument12 pagesPostop Actual &potential NCPJohn Paul Delos SantosNo ratings yet
- Baldo NCP R.A Case ObDocument2 pagesBaldo NCP R.A Case ObRoxanne BaldoNo ratings yet
- Group 1 - VITALS SIGNS and INTERVENTIONSDocument19 pagesGroup 1 - VITALS SIGNS and INTERVENTIONSTrishNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term: Short TermDocument5 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term: Short TermJA BerzabalNo ratings yet
- NCP StrokeDocument6 pagesNCP StrokeAnna PalimaNo ratings yet
- Subdural HematomaDocument4 pagesSubdural Hematomarodamel gundanNo ratings yet
- Ineffective Cerebral Tissue PerfusionDocument4 pagesIneffective Cerebral Tissue PerfusionLeticia ElricNo ratings yet
- Risk For IneffectiveDocument6 pagesRisk For IneffectiveAce FabrigasNo ratings yet
- Jade R. Dinolan BSN-4: Diagnosi SDocument5 pagesJade R. Dinolan BSN-4: Diagnosi SJhade Relleta100% (1)
- NCP BeeaDocument3 pagesNCP BeeaKiko BernardinoNo ratings yet
- Date/Time Cues N E E D Nursing Diagnosis Objectives of Care Nursing Interventions EvaluationDocument4 pagesDate/Time Cues N E E D Nursing Diagnosis Objectives of Care Nursing Interventions EvaluationRczhNo ratings yet
- Nursing Care Plan 1Document4 pagesNursing Care Plan 1Kiko BernardinoNo ratings yet
- NCP - Tissue Perfusion (Cerebral)Document2 pagesNCP - Tissue Perfusion (Cerebral)moodlayers50% (6)
- Decreased Cardiac OutputDocument5 pagesDecreased Cardiac Outputshuang81No ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanAmal Bacaraman MauteNo ratings yet
- annotated-COURSE TASK 2 INCREASED ICPDocument8 pagesannotated-COURSE TASK 2 INCREASED ICPJake AllegoNo ratings yet
- Hemorrhagic StrokeDocument2 pagesHemorrhagic StrokeMuhammad Anwar AnsoriNo ratings yet
- Nursing Care PlanDocument7 pagesNursing Care PlanGem Ma100% (7)
- Nic IctpDocument2 pagesNic IctpRobby BanjarNo ratings yet
- Concept Map, Neil Floyd Ventura PDFDocument1 pageConcept Map, Neil Floyd Ventura PDFNeil Floyd VenturaNo ratings yet
- Revised NCP 1-3Document6 pagesRevised NCP 1-3MarcieNo ratings yet
- NCP - Activity IntoleranceDocument4 pagesNCP - Activity IntoleranceRoyce Vincent TizonNo ratings yet
- Patients Nursing PlanDocument3 pagesPatients Nursing Planmharjoe pulmanoNo ratings yet
- Final NCP (Jannel)Document6 pagesFinal NCP (Jannel)Zed P. EstalillaNo ratings yet
- Med Ward NCP Week 3Document4 pagesMed Ward NCP Week 3Ghianx Carlox PioquintoxNo ratings yet
- NCP (Stroke)Document9 pagesNCP (Stroke)Claire M. AuditorNo ratings yet
- Assessment Explanation Planning Interventions Rationale Evaluation Subjective: Objective: STG: STGDocument11 pagesAssessment Explanation Planning Interventions Rationale Evaluation Subjective: Objective: STG: STGGrape JuiceNo ratings yet
- The Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaFrom EverandThe Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaNo ratings yet
- Absence Seizures: From Pathophysiology to Personalized CareFrom EverandAbsence Seizures: From Pathophysiology to Personalized CareNo ratings yet
- A Simple Guide to Parkinson's Disease and Related Brain ConditionsFrom EverandA Simple Guide to Parkinson's Disease and Related Brain ConditionsNo ratings yet
- Republic of The PhilippinesDocument12 pagesRepublic of The PhilippinesDienizs Labini TadenaNo ratings yet
- Poor Water Supply and SanitationDocument1 pagePoor Water Supply and SanitationDienizs Labini TadenaNo ratings yet
- Case Scenario Rotation 2Document3 pagesCase Scenario Rotation 2Dienizs Labini TadenaNo ratings yet
- Discharge Planning: MedicationsDocument3 pagesDischarge Planning: MedicationsDienizs Labini TadenaNo ratings yet
- Labini, Dienizs Act.1 CHNDocument4 pagesLabini, Dienizs Act.1 CHNDienizs Labini TadenaNo ratings yet
- DS 4 To 6Document8 pagesDS 4 To 6Dienizs Labini TadenaNo ratings yet
- Labini, Dienizs Bsn-3E: Incomplete Immunization Criteria Score Computation Answer JustificationDocument6 pagesLabini, Dienizs Bsn-3E: Incomplete Immunization Criteria Score Computation Answer JustificationDienizs Labini TadenaNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanDienizs Labini Tadena100% (1)
- Drug Study: Labini, Dienizs Bsn-3EDocument10 pagesDrug Study: Labini, Dienizs Bsn-3EDienizs Labini TadenaNo ratings yet
- Rhu Act. 2Document2 pagesRhu Act. 2Dienizs Labini TadenaNo ratings yet
- Kardex: GCS: 12-13/15 (M:5, V:4-5, E:3)Document11 pagesKardex: GCS: 12-13/15 (M:5, V:4-5, E:3)Dienizs Labini TadenaNo ratings yet
- MVH Ward Case ScenarioDocument3 pagesMVH Ward Case ScenarioDienizs Labini TadenaNo ratings yet
- Dienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDocument11 pagesDienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDienizs Labini TadenaNo ratings yet
- Dienizs Labini - NCM 117 Skills Activity #1Document3 pagesDienizs Labini - NCM 117 Skills Activity #1Dienizs Labini TadenaNo ratings yet
- Case Scenario For ADHDDocument2 pagesCase Scenario For ADHDDienizs Labini TadenaNo ratings yet
- Dienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDocument11 pagesDienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDienizs Labini TadenaNo ratings yet
- D123 DRQDocument1 pageD123 DRQDienizs Labini TadenaNo ratings yet
- University of Northern PhilippinesDocument15 pagesUniversity of Northern PhilippinesDienizs Labini TadenaNo ratings yet
- Do You Love MeDocument3 pagesDo You Love MeDienizs Labini TadenaNo ratings yet
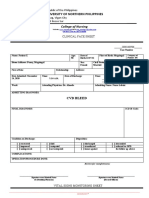
- Clinical Face Sheet: Diabetes Millitus T2Document3 pagesClinical Face Sheet: Diabetes Millitus T2Dienizs Labini TadenaNo ratings yet
- Read The Passage and Answer The Questions: by An Old Age"Document1 pageRead The Passage and Answer The Questions: by An Old Age"Hesen Gozelov100% (1)
- Quality and Standards and Their Role in Responding To Covid-19Document18 pagesQuality and Standards and Their Role in Responding To Covid-19Ardhi Novrialdi GintingNo ratings yet
- Exercise 4: Cost Benefits Analysis: 1. UK HSE CBA MethodDocument4 pagesExercise 4: Cost Benefits Analysis: 1. UK HSE CBA MethodMuhammad.SaimNo ratings yet
- Benign Anorectal Conditions: Ahmed Badrek-AmoudiDocument20 pagesBenign Anorectal Conditions: Ahmed Badrek-AmoudiAna De La RosaNo ratings yet
- Bact Enyeritis ElancoDocument20 pagesBact Enyeritis Elancoamamùra maamarNo ratings yet
- Persistant Pain in Olders. Updated (Dr. WILLY HALIM, MD, PHD, FIPP)Document25 pagesPersistant Pain in Olders. Updated (Dr. WILLY HALIM, MD, PHD, FIPP)Mulya ImansyahNo ratings yet
- Eco 2Document11 pagesEco 2Walaa KhasawnehNo ratings yet
- Res 2020-225 Ord Penalizing Dishonesty Untruthful Declaration Patient Times Public Health Emergency IloIloDocument3 pagesRes 2020-225 Ord Penalizing Dishonesty Untruthful Declaration Patient Times Public Health Emergency IloIloRave PerezNo ratings yet
- Drug StudyDocument2 pagesDrug StudySORENI SORENINo ratings yet
- Real-World Evidence For Assessing Treatment Effectiveness and Safety in Pediatric PopulationsDocument5 pagesReal-World Evidence For Assessing Treatment Effectiveness and Safety in Pediatric PopulationsAnonymous EAPbx6No ratings yet
- CGH PPT - CCCDocument45 pagesCGH PPT - CCCIan GreyNo ratings yet
- Physiology lab: Faculty of Medical laboratory since Patch 7 ليعامسإ دمحم اللهدبع مكوخأ صيخلتDocument32 pagesPhysiology lab: Faculty of Medical laboratory since Patch 7 ليعامسإ دمحم اللهدبع مكوخأ صيخلتmohammedNo ratings yet
- EchinococcosisDocument52 pagesEchinococcosisZezo TarekNo ratings yet
- P&T Chapter Wise 300 MCQDocument13 pagesP&T Chapter Wise 300 MCQsudeep kulkarni100% (1)
- Predictive Homeopathy Course Review, Part I: Susanne Saltzman, MDDocument5 pagesPredictive Homeopathy Course Review, Part I: Susanne Saltzman, MDdr TotoNo ratings yet
- HAK DAN KEWAJIBAN PASIEN InggrisDocument1 pageHAK DAN KEWAJIBAN PASIEN Inggrisdewi asnaniNo ratings yet
- NRG 204: 3Rd Week Gestational Conditions Pregnancy-Induced Hypertension What Is Blood Pressure? Risk FactorsDocument16 pagesNRG 204: 3Rd Week Gestational Conditions Pregnancy-Induced Hypertension What Is Blood Pressure? Risk FactorsEmmy Flor ValmoriaNo ratings yet
- Oral Hygiene Status of Mentally Handicapped School Children in Ibadan, NigeriaDocument3 pagesOral Hygiene Status of Mentally Handicapped School Children in Ibadan, Nigeriadaniel_siitompulNo ratings yet
- What Every Church Needs To Know About Generation ZDocument225 pagesWhat Every Church Needs To Know About Generation ZSamuel MolinaNo ratings yet
- Report On HivDocument4 pagesReport On HivRody Mark AraoNo ratings yet
- Lorenzo VS Gsis and DepedDocument28 pagesLorenzo VS Gsis and DepedViolet BlueNo ratings yet
- Admin, JPHV VESTIBULAR NEURONITIS 3Document5 pagesAdmin, JPHV VESTIBULAR NEURONITIS 3williams papilayaNo ratings yet
- Chronic Renal Failure: Lecture Speaker Dr. V. Lakshmi Prasanna MariseDocument23 pagesChronic Renal Failure: Lecture Speaker Dr. V. Lakshmi Prasanna MariseManjunath ArunachalamNo ratings yet
- BENNETT VS SACRAMENTO COUNTY JAIL Et Al.Document57 pagesBENNETT VS SACRAMENTO COUNTY JAIL Et Al.Andrew LiebichNo ratings yet
- Pengelolaan Prediabetes Di Faskes PrimerDocument37 pagesPengelolaan Prediabetes Di Faskes PrimerRia Mokoagow Bunda ReyvanNo ratings yet
- Position Paper SudanDocument2 pagesPosition Paper SudanPI CubingNo ratings yet
- Oncology NursingDocument19 pagesOncology NursingMarlowe DulayNo ratings yet
- Hypothyroidism An UpdateDocument8 pagesHypothyroidism An Updateجعفر محمدNo ratings yet