Download as pdf or txt
You might also like
- SSNB QuestionDocument41 pagesSSNB Questionms_ayeayenu95% (294)
- Overtraining Syndrome (OTS) and Relative Energy Deficiency in Sport (RED S) : Shared Pathways, Symptoms and ComplexitiesDocument30 pagesOvertraining Syndrome (OTS) and Relative Energy Deficiency in Sport (RED S) : Shared Pathways, Symptoms and ComplexitiesHugo TintiNo ratings yet
- Anxiety in PCOSDocument5 pagesAnxiety in PCOSUsama Bin ZubairNo ratings yet
- Abdominal Problems in Children With Congenital Cardiovascular AbnormalitiesDocument6 pagesAbdominal Problems in Children With Congenital Cardiovascular AbnormalitiesEldoNo ratings yet
- E2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Document1 pageE2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Sadam_fasterNo ratings yet
- Association of Clinical Features With Obesity and Gonadotropin Levels in Women With Polycystic Ovarian SyndromeDocument4 pagesAssociation of Clinical Features With Obesity and Gonadotropin Levels in Women With Polycystic Ovarian Syndromedoctor wajihaNo ratings yet
- Epidemiology of Polycystic Ovary Syndrome: A Cross Sectional Study of University Students at An-Najah National University-PalestineDocument6 pagesEpidemiology of Polycystic Ovary Syndrome: A Cross Sectional Study of University Students at An-Najah National University-PalestineOckta KaruniaNo ratings yet
- PIH Renal Doppler Pregnancy - CutDocument4 pagesPIH Renal Doppler Pregnancy - CutAnonymous 9QxPDpNo ratings yet
- Whither PCOS The Challenges of Establishing Hyperandrogenism in Adolescent Girls 2008 Journal of Adolescent HealthDocument3 pagesWhither PCOS The Challenges of Establishing Hyperandrogenism in Adolescent Girls 2008 Journal of Adolescent HealthfujimeisterNo ratings yet
- Chest 147 1 132Document8 pagesChest 147 1 132Timothy Eduard A. SupitNo ratings yet
- 6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Document11 pages6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Johanna Bustos NutricionistaNo ratings yet
- 10.1515@jpem 2018 0516Document8 pages10.1515@jpem 2018 0516pelinNo ratings yet
- Relationship Between Psoriasis and Non-Alcoholic Fatty Liver DiseaseDocument14 pagesRelationship Between Psoriasis and Non-Alcoholic Fatty Liver Diseaseimam mulyadiNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptYuniati ValentinaNo ratings yet
- Fasting Serum Insulin Levels and Insulin Resistance Are Associated With Colorectal Adenoma in KoreansDocument8 pagesFasting Serum Insulin Levels and Insulin Resistance Are Associated With Colorectal Adenoma in KoreansTanveerNo ratings yet
- Cancer de Endometrio Preserv Fer 2021Document15 pagesCancer de Endometrio Preserv Fer 2021Claudia Mugruza BedoyaNo ratings yet
- 1 s2.0 S168719792100040X MainDocument4 pages1 s2.0 S168719792100040X MainfelipetheNo ratings yet
- Dickson 1989Document7 pagesDickson 1989Necesito esta cuentaNo ratings yet
- The Impact of Malnutritional Status On Survival in Elderly Hemodialysis PatientsDocument5 pagesThe Impact of Malnutritional Status On Survival in Elderly Hemodialysis PatientsTika MahelsaNo ratings yet
- Seite 92-98 #220341-ErkanDocument7 pagesSeite 92-98 #220341-Erkancaydin33No ratings yet
- Proteinuria and The Risk of Developing End-Stage Renal DiseaseDocument7 pagesProteinuria and The Risk of Developing End-Stage Renal Diseasemutiara nurzaniNo ratings yet
- The Severity of Ultrasonographic Findings in Nonalcoholic Fatty Liver Disease Reflects The Metabolic Syndrome and Visceral Fat AccumulationDocument8 pagesThe Severity of Ultrasonographic Findings in Nonalcoholic Fatty Liver Disease Reflects The Metabolic Syndrome and Visceral Fat AccumulationMohammed KedirNo ratings yet
- Essah 2011Document6 pagesEssah 2011ThormmmNo ratings yet
- Costello 2007Document10 pagesCostello 2007ThormmmNo ratings yet
- PCOS Guidelines 1Document14 pagesPCOS Guidelines 1Angelie Therese ChuaNo ratings yet
- Early Atherosclerotic Changes in The Patients With Idiopathic Epilepsyegyptian Preliminary Study 2472 0895 1000112Document6 pagesEarly Atherosclerotic Changes in The Patients With Idiopathic Epilepsyegyptian Preliminary Study 2472 0895 1000112Luther ThengNo ratings yet
- 11 134 v12n4 2013 PredictingPortalDocument11 pages11 134 v12n4 2013 PredictingPortalDevy Widiya GrafitasariNo ratings yet
- Differences in Nutritional Risk Assessment Between NRS2002, RFH-NPT and LDUST in Cirrhotic PatientsDocument8 pagesDifferences in Nutritional Risk Assessment Between NRS2002, RFH-NPT and LDUST in Cirrhotic PatientsMasna ArahmanNo ratings yet
- EJMCM - Volume 10 - Issue 4 - Pages 893-903Document11 pagesEJMCM - Volume 10 - Issue 4 - Pages 893-903Junaid IwqNo ratings yet
- Reliability of Mini Nutritional Assessment in Hemodialysis Compared With Subjective Global AssessmentDocument6 pagesReliability of Mini Nutritional Assessment in Hemodialysis Compared With Subjective Global AssessmentyafanitaizzatiNo ratings yet
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocument7 pagesNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedNo ratings yet
- First Trimester Renin and Aldosterone Levels of Pregnancies Complicated With Preeclampsia And:or Related Adverse Pregnancy OutcomesDocument6 pagesFirst Trimester Renin and Aldosterone Levels of Pregnancies Complicated With Preeclampsia And:or Related Adverse Pregnancy OutcomesyinvilllNo ratings yet
- Hidronefrosis 3Document11 pagesHidronefrosis 3Zwinglie SandagNo ratings yet
- Articulo Juan SarcopeniaDocument5 pagesArticulo Juan SarcopeniaLaura Valentina Paez PeñaNo ratings yet
- Jurnal DWIDocument6 pagesJurnal DWIDwi Asti Lestari PandeNo ratings yet
- Nutritional Rehabilitation For Children With Congenital Heart Disease With Left To Right ShuntDocument10 pagesNutritional Rehabilitation For Children With Congenital Heart Disease With Left To Right ShuntJiradett Arm KerdsriNo ratings yet
- Polycystic Ovary SyndromeDocument13 pagesPolycystic Ovary SyndromeLIZARDO CRUZADO DIAZNo ratings yet
- Protein Energy Malnutrition in CKD PatientsDocument4 pagesProtein Energy Malnutrition in CKD PatientsEditor IJTSRDNo ratings yet
- Factors Predicting Malnutrition in Hemodialysis Patients: A Cross-Sectional StudyDocument10 pagesFactors Predicting Malnutrition in Hemodialysis Patients: A Cross-Sectional StudyMarco TolentinoNo ratings yet
- Jurnal AKIDocument7 pagesJurnal AKIAnonymous Vz9teLNo ratings yet
- Preeclampsia and ESRD The Role of Shared Risk Factors - 2017 - American Journal of Kidney Diseases PDFDocument8 pagesPreeclampsia and ESRD The Role of Shared Risk Factors - 2017 - American Journal of Kidney Diseases PDFfujimeisterNo ratings yet
- Clinical Presentation, Diagnosis and Long-Term Outcome of Wilson's Disease: A Cohort StudyDocument6 pagesClinical Presentation, Diagnosis and Long-Term Outcome of Wilson's Disease: A Cohort Studyvinodksahu100% (1)
- AKI Child W NS 2018Document4 pagesAKI Child W NS 2018Indah Nur LathifahNo ratings yet
- Study of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyDocument6 pagesStudy of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyHarvey MatbaganNo ratings yet
- Nelson2013 Ajog PDFDocument7 pagesNelson2013 Ajog PDFsaryindrianyNo ratings yet
- Androgen Excess in Women Experience With Over 1000Document10 pagesAndrogen Excess in Women Experience With Over 1000Luisa Salazar VillegasNo ratings yet
- RMB2 16 67 PDFDocument5 pagesRMB2 16 67 PDFMariam QaisNo ratings yet
- Zhang 2015 PDFDocument8 pagesZhang 2015 PDFSward FamNo ratings yet
- Irisin in AdolecenceDocument4 pagesIrisin in Adolecencemiss beeNo ratings yet
- Association of Biochemical Markers With The Severity of Pre EclampsiaDocument7 pagesAssociation of Biochemical Markers With The Severity of Pre EclampsiaFer OrnelasNo ratings yet
- Newell Price2006Document13 pagesNewell Price2006fkia2013No ratings yet
- Conjugated Hyperbilirubinemia in The Neonatal Intensive Care UnitDocument9 pagesConjugated Hyperbilirubinemia in The Neonatal Intensive Care UnitIvan HoNo ratings yet
- Absolute Final Corrected Fecal Elastase ProposalDocument4 pagesAbsolute Final Corrected Fecal Elastase ProposalSaad KhanNo ratings yet
- Nephrectomymarch 17Document6 pagesNephrectomymarch 17Muthoh HaroNo ratings yet
- PGHN 17 162Document8 pagesPGHN 17 162Melany Sii PenghayalNo ratings yet
- Adler 2015Document7 pagesAdler 2015nathaliepichardoNo ratings yet
- GWAS PCOS KoreaDocument9 pagesGWAS PCOS KoreaedwardNo ratings yet
- Accepted Manuscript: 10.1016/j.jpag.2017.07.008Document25 pagesAccepted Manuscript: 10.1016/j.jpag.2017.07.008Fifi Retiaty YasinNo ratings yet
- Is Massive Proteinuria Associated With Maternal An PDFDocument6 pagesIs Massive Proteinuria Associated With Maternal An PDFAmpry LoyraNo ratings yet
- Fasting Glucose Insulin Ratio: A Useful Measure of Insulin Resistance in Girls With Premature AdrenarcheDocument4 pagesFasting Glucose Insulin Ratio: A Useful Measure of Insulin Resistance in Girls With Premature AdrenarcheYOG.GANAR2291No ratings yet
- The Metabolic Syndrome in Polycystic Ovary SyndromeDocument21 pagesThe Metabolic Syndrome in Polycystic Ovary SyndromeHAVIZ YUADNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyFrom EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyNo ratings yet
- Surrogate Pregnancy: An Analysis of The Current Situation: Questions of The Víctor Grífols I Lucas FoundationDocument43 pagesSurrogate Pregnancy: An Analysis of The Current Situation: Questions of The Víctor Grífols I Lucas Foundationmeltwithsnow163.comNo ratings yet
- Myelination All About Rac N' RollDocument3 pagesMyelination All About Rac N' Rollmeltwithsnow163.comNo ratings yet
- ErbB Signaling Has A Role in Radial Sorting Independent of Schwann Cell NumberDocument15 pagesErbB Signaling Has A Role in Radial Sorting Independent of Schwann Cell Numbermeltwithsnow163.comNo ratings yet
- Anti-Mouse Igg1 Microbeads: 2 ML 130-047-101 1 ML 130-047-102Document4 pagesAnti-Mouse Igg1 Microbeads: 2 ML 130-047-101 1 ML 130-047-102meltwithsnow163.comNo ratings yet
- Gestational Surrogacy Contract InfographicDocument1 pageGestational Surrogacy Contract Infographicmeltwithsnow163.comNo ratings yet
- Ms Columns: Miltenyi Biotec Inc. Miltenyi Biotec GMBHDocument2 pagesMs Columns: Miltenyi Biotec Inc. Miltenyi Biotec GMBHmeltwithsnow163.comNo ratings yet
- Gmail - ABM Order Processing - Confirmation of Order 40662 - Notice of BackorderDocument2 pagesGmail - ABM Order Processing - Confirmation of Order 40662 - Notice of Backordermeltwithsnow163.comNo ratings yet
- ART 2015 Clinic Report Tables ID NY PDFDocument177 pagesART 2015 Clinic Report Tables ID NY PDFmeltwithsnow163.comNo ratings yet
- ART 2015 Clinic Report Full PDFDocument586 pagesART 2015 Clinic Report Full PDFmeltwithsnow163.comNo ratings yet
- ART 2014 Clinic Report Full PDFDocument588 pagesART 2014 Clinic Report Full PDFmeltwithsnow163.comNo ratings yet
- Art 2014 National Summary Report PDFDocument78 pagesArt 2014 National Summary Report PDFmeltwithsnow163.comNo ratings yet
- Ajas 27 10 1411 PDFDocument6 pagesAjas 27 10 1411 PDFmeltwithsnow163.comNo ratings yet
- Determination of Sperm Sex Ratio in Bovine Semen Using Multiplex Real-Time Polymerase Chain ReactionDocument6 pagesDetermination of Sperm Sex Ratio in Bovine Semen Using Multiplex Real-Time Polymerase Chain Reactionmeltwithsnow163.comNo ratings yet
- Original Article: Serum Metabolomic Profiles Suggest Influence of Sex and Oral Contraceptive UseDocument11 pagesOriginal Article: Serum Metabolomic Profiles Suggest Influence of Sex and Oral Contraceptive Usemeltwithsnow163.comNo ratings yet
- AromatherapyDocument3 pagesAromatherapyFrancesco100% (2)
- Physiology Chapter 30 Renal Regulation of PotassiumDocument32 pagesPhysiology Chapter 30 Renal Regulation of PotassiumDaniel AdamsNo ratings yet
- Water: Carah Fe Bacus, RNDocument24 pagesWater: Carah Fe Bacus, RNcoosa liquorsNo ratings yet
- LECTURE 6 Male Reproductive System - Histology HB II 2023Document76 pagesLECTURE 6 Male Reproductive System - Histology HB II 2023Emmanuel AssopiahNo ratings yet
- Ceramides - 2 JurnalDocument54 pagesCeramides - 2 Jurnaldian kaizenNo ratings yet
- The 3 Stages of LoveDocument2 pagesThe 3 Stages of LoveShekinah Mae M. CulhiNo ratings yet
- 1 - Preaseason Quiz - Biochemistry (Interns)Document14 pages1 - Preaseason Quiz - Biochemistry (Interns)Reidan de CastroNo ratings yet
- Material Safety Data Sheet Product Identity: Power Cool CoolantDocument12 pagesMaterial Safety Data Sheet Product Identity: Power Cool CoolantMauricio CasasNo ratings yet
- Aerobic Respiration WorksheetDocument1 pageAerobic Respiration Worksheet20WestheadBNo ratings yet
- Vitamin DeficiencyDocument5 pagesVitamin Deficiencyritika jainNo ratings yet
- IBDP Biology Option - D - SummaryDocument5 pagesIBDP Biology Option - D - SummaryRafi FarhanNo ratings yet
- FSHN Quizes Exam 3Document13 pagesFSHN Quizes Exam 3Jillian NicoleNo ratings yet
- Ketogenesis and KetolysisDocument4 pagesKetogenesis and KetolysisSergio D. Sánchez VillamarínNo ratings yet
- A Clinician's Guide To Topical Retinoids: Melika Motamedi, Ahmad Chehade, Ravina Sanghera, and Parbeer GrewalDocument8 pagesA Clinician's Guide To Topical Retinoids: Melika Motamedi, Ahmad Chehade, Ravina Sanghera, and Parbeer Grewalzendah123No ratings yet
- Atlas of Postmenopausal Osteoporosis 3rd Ed. - R. Rizzoli (CMG, 2010) WWDocument127 pagesAtlas of Postmenopausal Osteoporosis 3rd Ed. - R. Rizzoli (CMG, 2010) WWBrankoSalvariNo ratings yet
- Anatomy and Physiology of Adrenal GlandsDocument14 pagesAnatomy and Physiology of Adrenal GlandsEunice CuñadaNo ratings yet
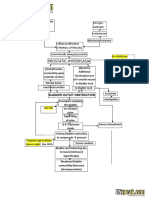
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDocument2 pagesBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailNo ratings yet
- B12 CobasDocument5 pagesB12 CobasAntonio Morales CanoNo ratings yet
- Embryonal Remnants in The Testis and EpididymisDocument9 pagesEmbryonal Remnants in The Testis and EpididymisKata TölgyesiNo ratings yet
- Hypothermia - StatPearls - NCBI BookshelfDocument9 pagesHypothermia - StatPearls - NCBI BookshelfAyishaNo ratings yet
- Case Study Med SurgDocument2 pagesCase Study Med SurgKayla NapolitanoNo ratings yet
- Grade 10 Quarter 3 Lym ADocument4 pagesGrade 10 Quarter 3 Lym ALymberth BenallaNo ratings yet
- Diarrea Aguda FisiopatologiaDocument9 pagesDiarrea Aguda FisiopatologiaSeverino P. CrispinNo ratings yet
- Principles of Medical Laboratory Science 1Document15 pagesPrinciples of Medical Laboratory Science 1Julianne Marie LacsentoNo ratings yet
- Serum Ionic Calcium Levels and Hypocalcemia in DenDocument5 pagesSerum Ionic Calcium Levels and Hypocalcemia in DenJoko Purnomo HNo ratings yet
- UrsodiolDocument2 pagesUrsodiolFarahNo ratings yet
- Soy - Peptone - FM MsdsDocument1 pageSoy - Peptone - FM MsdsSorin LazarNo ratings yet
- Anemia Umam FazlurrahmanDocument44 pagesAnemia Umam Fazlurrahmanumam fazlurrahmanNo ratings yet