Download as pdf or txt
You might also like
- PCP Western Visayad Panay Chapter Rite/Psbim ReviewDocument6 pagesPCP Western Visayad Panay Chapter Rite/Psbim ReviewKarl Pineda0% (1)
- KetoconazoleDocument2 pagesKetoconazoleMD. DELWAR HOSSAINNo ratings yet
- Ertapenem (Invanz)Document1 pageErtapenem (Invanz)Adrianne BazoNo ratings yet
- Medication: Expected Pharmacological Action Therapeutic UseDocument1 pageMedication: Expected Pharmacological Action Therapeutic UseAli GarciaNo ratings yet
- Glipizide Glucotrol XL Drug CardDocument1 pageGlipizide Glucotrol XL Drug CardSheri490No ratings yet
- DiazepamDocument1 pageDiazepamFerdinand Sherwin MorataNo ratings yet
- Bioh111 So S1 2013Document9 pagesBioh111 So S1 2013monicq77No ratings yet
- Piracetam 800mg TabletsDocument5 pagesPiracetam 800mg TabletsSuvaneel MoulickNo ratings yet
- Drug StudyDocument8 pagesDrug StudyGian Era100% (1)
- Drug StudyDocument3 pagesDrug StudyTrixia ArcegonoNo ratings yet
- Insulin As PartDocument3 pagesInsulin As PartRezaNo ratings yet
- Combizar Drug StudyDocument6 pagesCombizar Drug StudymrnmrsllNo ratings yet
- Amikacin 2Document2 pagesAmikacin 2Sian AsadaNo ratings yet
- SeroquelDocument2 pagesSeroqueldanaNo ratings yet
- GravolDocument5 pagesGravoldrugcardrefNo ratings yet
- Nortriptyline Hydro ChlorideDocument3 pagesNortriptyline Hydro Chlorideapi-3797941No ratings yet
- DRUG StudyDocument6 pagesDRUG StudyJheryck SabadaoNo ratings yet
- OmeprazoleDocument2 pagesOmeprazoleKristine YoungNo ratings yet
- Drug Name Mechanism of Action Administration Indication Contraindication Adverse Effects Nursing ResponsibilitiesDocument1 pageDrug Name Mechanism of Action Administration Indication Contraindication Adverse Effects Nursing ResponsibilitiesIvan Liquiran AvenadoNo ratings yet
- NiacinDocument2 pagesNiacinΚωνσταντίνος ΓκάργκαςNo ratings yet
- Drug Analysis: Malaise, Fatigue, Dizziness, Tremors, AtaxiaDocument2 pagesDrug Analysis: Malaise, Fatigue, Dizziness, Tremors, AtaxiaFerdinand Sherwin MorataNo ratings yet
- Miglitol (Glyset)Document1 pageMiglitol (Glyset)ENo ratings yet
- Metoclopramide (Reglan)Document1 pageMetoclopramide (Reglan)ENo ratings yet
- Anticholinergics Study Drug ListDocument1 pageAnticholinergics Study Drug ListDrima Edi100% (1)
- Drug StudyDocument14 pagesDrug StudyNikki RodrigoNo ratings yet
- Drug Study: (Celecoxib)Document11 pagesDrug Study: (Celecoxib)Princess Brigitte R. PATE�ANo ratings yet
- Drug Study FUROSEMIDE (Eugene San)Document2 pagesDrug Study FUROSEMIDE (Eugene San)Ana LanticseNo ratings yet
- Drug Study: Meclizine Is An Antagonist atDocument2 pagesDrug Study: Meclizine Is An Antagonist atJayson Ray AbellarNo ratings yet
- MoclodemideDocument1 pageMoclodemideArnzz AgbulosNo ratings yet
- Drug StudyDocument11 pagesDrug StudyJay VillasotoNo ratings yet
- 005LEU11EDocument4 pages005LEU11ELiaWahyuniNo ratings yet
- IFOSFAMIDEDocument4 pagesIFOSFAMIDEErza GenatrikaNo ratings yet
- Drug Study: Patient: B.V Age: 58y/oDocument2 pagesDrug Study: Patient: B.V Age: 58y/oAndrea Sibayan SorianoNo ratings yet
- IvabradineDocument4 pagesIvabradineLamy SNo ratings yet
- SimethiconeDocument1 pageSimethiconeDivine Dela PenaNo ratings yet
- PonstanDocument2 pagesPonstanianecunar100% (2)
- Parenteral NutritionDocument5 pagesParenteral NutritionReanne PaulineNo ratings yet
- PiracetamDocument5 pagesPiracetamtTEInjr0kZNo ratings yet
- ACALKADocument1 pageACALKAErnie LaraNo ratings yet
- DrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Document2 pagesDrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Coleen Mae CamaristaNo ratings yet
- RisperidoneDocument2 pagesRisperidoneNinoska Garcia-Ortiz100% (1)
- Disaster Nursing SAS Session 13Document7 pagesDisaster Nursing SAS Session 13Niceniadas CaraballeNo ratings yet
- BrivaracetamDocument110 pagesBrivaracetamBendisDacicaNo ratings yet
- ValsartanDocument3 pagesValsartanapi-3797941100% (1)
- Drug Study KeterolacDocument2 pagesDrug Study KeterolacKillerBall RegioNo ratings yet
- Drug Study HepatitisDocument7 pagesDrug Study HepatitisKateLayaogNo ratings yet
- Er Drug StudyDocument29 pagesEr Drug StudyMa Karenina DualanNo ratings yet
- Ciprofloxacin CiproDocument1 pageCiprofloxacin CiproKristi WrayNo ratings yet
- ImipramineDocument1 pageImipramineMuhammad ArsalanNo ratings yet
- PrednisoneDocument3 pagesPrednisoneMaja DeraNo ratings yet
- Drug StudyDocument5 pagesDrug StudyRai D. MacapantonNo ratings yet
- DRUG NAME: Hydroxyurea: Synonym (S) : Common Trade Name (S) : ClassificationDocument7 pagesDRUG NAME: Hydroxyurea: Synonym (S) : Common Trade Name (S) : ClassificationDewinta AbutNo ratings yet
- Serratiopeptidase Is An Enzyme Having AntiDocument12 pagesSerratiopeptidase Is An Enzyme Having Antidracula386No ratings yet
- Drug Study: Aspirin (Asa)Document5 pagesDrug Study: Aspirin (Asa)Shara Lailanie A. AzisNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- New Zealand Data Sheet: 1 Product NameDocument8 pagesNew Zealand Data Sheet: 1 Product NameAhmed Abd El HakimNo ratings yet
- Levothyroxine 50mcg Tablets: 1. Name of The Medicinal ProductDocument7 pagesLevothyroxine 50mcg Tablets: 1. Name of The Medicinal ProductAnwaar Yousaf SmoreNo ratings yet
- Eltroxin TabletsDocument16 pagesEltroxin TabletsSarthak DixitNo ratings yet
- Eltroxin (New) TabDocument8 pagesEltroxin (New) TabhpradeepNo ratings yet
- Brand Name Generic Name Indications Dosage Side Effects: HyperthyroidismDocument11 pagesBrand Name Generic Name Indications Dosage Side Effects: HyperthyroidismshieNo ratings yet
- Eltroxin TabletsDocument17 pagesEltroxin Tabletsdaya A LNo ratings yet
- Eltroxin TabletsDocument17 pagesEltroxin TabletsYogeesh ChandrashekarNo ratings yet
- Estradiol As Hemihydrate 3.2mg (Evorel - 50)Document20 pagesEstradiol As Hemihydrate 3.2mg (Evorel - 50)ddandan_2No ratings yet
- Initial Treatment: Special WarningsDocument10 pagesInitial Treatment: Special Warningsddandan_2No ratings yet
- The Content of This Leaflet Was Updated According To The Guidelines of The Ministry of Health in September 2017Document14 pagesThe Content of This Leaflet Was Updated According To The Guidelines of The Ministry of Health in September 2017ddandan_2No ratings yet
- AMARYL 1mg, 2mg, 3mg, 4mg: 1 Indications and UsageDocument16 pagesAMARYL 1mg, 2mg, 3mg, 4mg: 1 Indications and Usageddandan_2No ratings yet
- Aclidinium Bromide 340mcg + Formoterol Fumarate 11.8mcg (Duaklir Genuair Inhalation Powder)Document22 pagesAclidinium Bromide 340mcg + Formoterol Fumarate 11.8mcg (Duaklir Genuair Inhalation Powder)ddandan_2No ratings yet
- Adapalene 0.1% (Adaferin Cream)Document6 pagesAdapalene 0.1% (Adaferin Cream)ddandan_2No ratings yet
- BaclofenDocument11 pagesBaclofenddandan_2No ratings yet
- Haloperidol 2mg-ml DropsDocument15 pagesHaloperidol 2mg-ml Dropsddandan_2No ratings yet
- Summary of Product CharacteristicsDocument24 pagesSummary of Product Characteristicsddandan_2No ratings yet
- Zofran Tablets 4mg Zofran Tablets 8mg: 1. Trade Name of The Medicinal ProductDocument12 pagesZofran Tablets 4mg Zofran Tablets 8mg: 1. Trade Name of The Medicinal Productddandan_2No ratings yet
- Dekinet Tablets: Use in PregnancyDocument3 pagesDekinet Tablets: Use in Pregnancyddandan_2No ratings yet
- Levodopa 250mg + Carbidopa 25mg (Dopicar)Document10 pagesLevodopa 250mg + Carbidopa 25mg (Dopicar)ddandan_2No ratings yet
- Doctor Leaflet: 1. Name of The Medicinal Product: Budeson 3 MGDocument11 pagesDoctor Leaflet: 1. Name of The Medicinal Product: Budeson 3 MGddandan_2No ratings yet
- Product Information: Chemical StructureDocument10 pagesProduct Information: Chemical Structureddandan_2No ratings yet
- AnastrozoleDocument13 pagesAnastrozoleddandan_2No ratings yet
- Netupitant 300mg + Palonosetron HCL 0.56mg (Akynzeo)Document16 pagesNetupitant 300mg + Palonosetron HCL 0.56mg (Akynzeo)ddandan_2No ratings yet
- Ibuprofen 150mg + Paracetamol 500mg (Combodex)Document15 pagesIbuprofen 150mg + Paracetamol 500mg (Combodex)ddandan_2No ratings yet
- Summary of Product Characteristics: Edronax 4 MGDocument9 pagesSummary of Product Characteristics: Edronax 4 MGddandan_2No ratings yet
- Cataflam: (Diclofenac Potassium)Document10 pagesCataflam: (Diclofenac Potassium)ddandan_2No ratings yet
- Summary of Product Characteristics 1 Name of The Medicinal ProductDocument9 pagesSummary of Product Characteristics 1 Name of The Medicinal Productddandan_2No ratings yet
- Adapalene 0.1% (Adaferin Gel)Document4 pagesAdapalene 0.1% (Adaferin Gel)ddandan_2No ratings yet
- Mycophenolate Mofetil (CellCept)Document16 pagesMycophenolate Mofetil (CellCept)ddandan_2No ratings yet
- Fusid®: TabletsDocument8 pagesFusid®: Tabletsddandan_2No ratings yet
- Endocrinology - Review NotesDocument9 pagesEndocrinology - Review NotesRoa Al-SajjanNo ratings yet
- Chemical Coordination and IntegrationDocument34 pagesChemical Coordination and IntegrationBiju Mylachal100% (9)
- Master Nilai Mapel Ips Kelas 7 Sem GenapDocument5 pagesMaster Nilai Mapel Ips Kelas 7 Sem GenapAlbert LiwaNo ratings yet
- AcromegalyDocument15 pagesAcromegalyHernandez LennieNo ratings yet
- Drugs For Repro System-1Document67 pagesDrugs For Repro System-1Jan Oliver YaresNo ratings yet
- Check in Out OutletDocument147 pagesCheck in Out Outlethrca spnNo ratings yet
- Self-Learning Home Task (SLHT)Document9 pagesSelf-Learning Home Task (SLHT)GraceEstoleCaloNo ratings yet
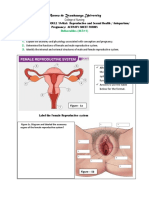
- ANATOMY OF THE FEMALE REPRODUCTIVE SYSTEM - RamosDocument4 pagesANATOMY OF THE FEMALE REPRODUCTIVE SYSTEM - RamosLouwella RamosNo ratings yet
- 7 Chakara and AssanaDocument32 pages7 Chakara and AssanadineshgomberNo ratings yet
- Elecsys AMH: 06331076 190 Cobas e 411 Cobas e 601 Cobas e 602 English System InformationDocument6 pagesElecsys AMH: 06331076 190 Cobas e 411 Cobas e 601 Cobas e 602 English System InformationAbdullah ZobayerNo ratings yet
- Osteoporosis Treatment-Teriparatide Injections - ForteoDocument2 pagesOsteoporosis Treatment-Teriparatide Injections - Forteorameshg2020No ratings yet
- TLC Flyer AADocument8 pagesTLC Flyer AAbearteddy17193No ratings yet
- Chronic Kidney Disease: The Philippine SituationDocument28 pagesChronic Kidney Disease: The Philippine SituationMarffy LlamasNo ratings yet
- Shahid Athar, MD, FACP, Face Author, "Islamic Perspective in Medicine" (ATP)Document25 pagesShahid Athar, MD, FACP, Face Author, "Islamic Perspective in Medicine" (ATP)She JocelynNo ratings yet
- Alert !!! 10-12 Hours Fasting Is Mandatory For Lipid Parameters. If Not, Values Might FluctuateDocument2 pagesAlert !!! 10-12 Hours Fasting Is Mandatory For Lipid Parameters. If Not, Values Might FluctuateArka Prava PaulNo ratings yet
- PT Cakra Medika Utama: Price List Boditech Med Inc (I-Chroma)Document2 pagesPT Cakra Medika Utama: Price List Boditech Med Inc (I-Chroma)raditNo ratings yet
- Hormones: Siti Zulaika Binti KasmatDocument21 pagesHormones: Siti Zulaika Binti KasmatikaNo ratings yet
- Dian Ais EditDocument41 pagesDian Ais EditDian SiregarNo ratings yet
- Board Question Paper - March 2023 - For Reprint Update - 641b040f4992cDocument4 pagesBoard Question Paper - March 2023 - For Reprint Update - 641b040f4992cSushan BhagatNo ratings yet
- Management of Insulin Resistance Through Ayurveda A Case StudyDocument3 pagesManagement of Insulin Resistance Through Ayurveda A Case StudyEditor IJTSRDNo ratings yet
- The Menstrual Cycle and Its AbnormalitiesDocument25 pagesThe Menstrual Cycle and Its AbnormalitiesAsteway MesfinNo ratings yet
- Hormonal Manipulation of Fishes As An Aquacultural TechniqueDocument11 pagesHormonal Manipulation of Fishes As An Aquacultural TechniqueRommel CorpuzNo ratings yet
- Soal InaCOG PembahasanDocument15 pagesSoal InaCOG Pembahasanevi.pratiwiNo ratings yet
- Hypoglycemia: Prepared By: Ahmed Rawhi DabourDocument84 pagesHypoglycemia: Prepared By: Ahmed Rawhi DabourKaterina FusaNo ratings yet
- Asynchronous Activity Sheet FormsDocument8 pagesAsynchronous Activity Sheet FormsNur SanaaniNo ratings yet
- Diseases Resulting From Nutrient DeficiencyDocument21 pagesDiseases Resulting From Nutrient DeficiencyAltrelle MoryelNo ratings yet
- Ncma217 Prelim ReviewerDocument51 pagesNcma217 Prelim Reviewerroldanmarygrace023No ratings yet
- Systemic Effects of Surgical Stress:: Dr. H.R.Bhardwaj: Asif AliDocument23 pagesSystemic Effects of Surgical Stress:: Dr. H.R.Bhardwaj: Asif Alimanzoor bhatNo ratings yet