Download as pdf or txt
You might also like
- Toronto Police Report On "Systemic Racism" in Officer Use of Force and Strip SearchesDocument119 pagesToronto Police Report On "Systemic Racism" in Officer Use of Force and Strip SearchesToronto Star100% (2)
- 2024-01-29 Municipal Permitting - Flushing Out The Nonsense enDocument37 pages2024-01-29 Municipal Permitting - Flushing Out The Nonsense enToronto StarNo ratings yet
- Application of The Convention On The Prevention and Punishment of The Crime of Genocide in The Gaza StripDocument29 pagesApplication of The Convention On The Prevention and Punishment of The Crime of Genocide in The Gaza StripToronto StarNo ratings yet
- The DRCOG Revision Guide Examination Preparation and Practice Questions 2nd Edition PDFDocument329 pagesThe DRCOG Revision Guide Examination Preparation and Practice Questions 2nd Edition PDFFarhan Kabir71% (7)
- Our Campus, Our SafetyDocument44 pagesOur Campus, Our SafetyToronto Star100% (2)
- Do2011 0255Document7 pagesDo2011 0255JBLMGH EMPLOYEESCLINICNo ratings yet
- Coronation Order of ServiceDocument50 pagesCoronation Order of ServiceCTV News100% (5)
- Case Study 3 Diabetes Mellitus Type 1Document62 pagesCase Study 3 Diabetes Mellitus Type 1HananErekat100% (2)
- Letter To Minister Downey Re Bingo Halls and OLGDocument3 pagesLetter To Minister Downey Re Bingo Halls and OLGToronto StarNo ratings yet
- Traditional Chinese Medicine TheoryDocument15 pagesTraditional Chinese Medicine TheorywarnerNo ratings yet
- Anapathic Machine Instructions FinalDocument5 pagesAnapathic Machine Instructions FinalGeraldine SamperioNo ratings yet
- Franklin Gardens Inspection ReportDocument5 pagesFranklin Gardens Inspection ReportToronto StarNo ratings yet
- Grace Villa Ministry Inspection Report Dec 22, 2020Document3 pagesGrace Villa Ministry Inspection Report Dec 22, 2020The Hamilton SpectatorNo ratings yet
- Mount Hope Ministry of Health Inspection ReportDocument55 pagesMount Hope Ministry of Health Inspection ReportmatthewtrevithickNo ratings yet
- Yukio Okutsu State Veterans Home ReportDocument16 pagesYukio Okutsu State Veterans Home ReportHPR News100% (1)
- Assessment Tool 10-26-2021Document17 pagesAssessment Tool 10-26-2021Aroroy RHUNo ratings yet
- DUMALNEG Assessment Tool For PCFDocument17 pagesDUMALNEG Assessment Tool For PCFdumalneghrh 2017No ratings yet
- Care Home Adults 18-65Document30 pagesCare Home Adults 18-65api-15470446100% (2)
- Urology in The Time of Covid19 Telemedicine and Econsults For Hospitalized Patients During Covid-19Document3 pagesUrology in The Time of Covid19 Telemedicine and Econsults For Hospitalized Patients During Covid-19tresy kalawaNo ratings yet
- 1 Public Materials Book - IC Com MTG 8.26.2020Document304 pages1 Public Materials Book - IC Com MTG 8.26.2020unidadqualityNo ratings yet
- Validation of Sentrong Sigla Criteria - BlankDocument26 pagesValidation of Sentrong Sigla Criteria - BlankkenvysNo ratings yet
- O. Reg. 305/21: REGULATED HEALTH PROFESSIONALSDocument2 pagesO. Reg. 305/21: REGULATED HEALTH PROFESSIONALSJason CookNo ratings yet
- 3021 PDFDocument20 pages3021 PDFDrKunal KaradeNo ratings yet
- Office of The SecretaryDocument12 pagesOffice of The SecretaryAnna Marie PadulNo ratings yet
- Regulation of Indonesian Medical CouncilDocument7 pagesRegulation of Indonesian Medical CouncilSagir AlvaNo ratings yet
- Onboarding Paperwork - CP-PY-039 COVID-19 Influenza Immunisation PolicyDocument2 pagesOnboarding Paperwork - CP-PY-039 COVID-19 Influenza Immunisation PolicyKiran JoshiNo ratings yet
- Oxygen Concentrator Services - Office of Inspector GeneralDocument77 pagesOxygen Concentrator Services - Office of Inspector Generaldj22500No ratings yet
- Convergence - PHC LevelDocument3 pagesConvergence - PHC LeveluhckkrNo ratings yet
- Grace Villa Inspection Report: Dec 11, 2020Document3 pagesGrace Villa Inspection Report: Dec 11, 2020The Hamilton SpectatorNo ratings yet
- DO 83 s2020 PDFDocument5 pagesDO 83 s2020 PDFRonaldo B. VillaromanNo ratings yet
- Rhu Citizen CharterDocument18 pagesRhu Citizen Charteradrian100% (1)
- In-Service Education VirginiaDocument25 pagesIn-Service Education Virginiaapi-234162801No ratings yet
- OnlineCIF Server Maintenance CIF Version 9 MergedDocument6 pagesOnlineCIF Server Maintenance CIF Version 9 MergedMarzen SumalbagNo ratings yet
- Ic-01-048 Infection Control in Pediatric Intensive Care UnitDocument6 pagesIc-01-048 Infection Control in Pediatric Intensive Care UnitDerick RanaNo ratings yet
- Dental Registration Act 1996Document26 pagesDental Registration Act 1996Ghansham SamarooNo ratings yet
- Vancouver Coastal Health Enhanced Surveillance and Precautions ProtocolsDocument1 pageVancouver Coastal Health Enhanced Surveillance and Precautions ProtocolsIan YoungNo ratings yet
- LC05 Rev06 SoC Legionella Control ServicesDocument4 pagesLC05 Rev06 SoC Legionella Control ServicesTarundeep SinghNo ratings yet
- Health: Citystate Boul RD, L'asig Call 0 TrunklincDocument22 pagesHealth: Citystate Boul RD, L'asig Call 0 TrunklincRappler100% (1)
- Students SecDocument8 pagesStudents Secyilongwei.comNo ratings yet
- April From Time Time For: Orders Have Been Issued Additional Lab by All TheDocument2 pagesApril From Time Time For: Orders Have Been Issued Additional Lab by All TheRaghavendra RaoNo ratings yet
- Milestone House: Care and Normalisation LimitedDocument18 pagesMilestone House: Care and Normalisation LimitedAlthea Mae GelacioNo ratings yet
- Daisuki Sushi Victoria Certificate PDFDocument2 pagesDaisuki Sushi Victoria Certificate PDFNicolae C.No ratings yet
- Covid 19 Modified RestrictionsDocument4 pagesCovid 19 Modified RestrictionsMelbinGeorgeNo ratings yet
- House Rules and Procedures For Reception and Accommodation CentresDocument53 pagesHouse Rules and Procedures For Reception and Accommodation CentresbourdillonjonesNo ratings yet
- National Protocol For Covid-19 Vaccine Astrazeneca, (Chadox1-S (Recombinant) )Document23 pagesNational Protocol For Covid-19 Vaccine Astrazeneca, (Chadox1-S (Recombinant) )lijoNo ratings yet
- COVID-19 Guidance and Standard Operating Procedure: Urgent Dental Care Systems in The Context of CoronavirusDocument49 pagesCOVID-19 Guidance and Standard Operating Procedure: Urgent Dental Care Systems in The Context of CoronavirusRolando SchmidtNo ratings yet
- dc2021 0386Document13 pagesdc2021 0386Chang GelvoleoNo ratings yet
- Standard No. CEA/Wellness Centre-018Document21 pagesStandard No. CEA/Wellness Centre-018Gladys MatiraNo ratings yet
- Citizen's CharterDocument12 pagesCitizen's CharterShayne Cabotaje Delos Santos - BorlingNo ratings yet
- Dec. 13 Letter of Instruction From Peterborough Public Health To Food PremisesDocument4 pagesDec. 13 Letter of Instruction From Peterborough Public Health To Food PremisesPeterborough ExaminerNo ratings yet
- Missing and Absent Without Leave Policy 1.2Document20 pagesMissing and Absent Without Leave Policy 1.2hatem newishyNo ratings yet
- preparing-for-a-dtss-practice-inspection -INTDocument14 pagespreparing-for-a-dtss-practice-inspection -INTPreciosa SilvaNo ratings yet
- Citizens CharterDocument29 pagesCitizens CharterHarold Paulo MejiaNo ratings yet
- Laporan Audit ISO14001-2015 THN 2019Document13 pagesLaporan Audit ISO14001-2015 THN 2019Rick SitumorangNo ratings yet
- Ic-01-039 Infection Control in Adult Intensive Care UnitDocument7 pagesIc-01-039 Infection Control in Adult Intensive Care UnitDerick RanaNo ratings yet
- K.C.S (R.P.P.P) Act 1973Document23 pagesK.C.S (R.P.P.P) Act 1973rohitNo ratings yet
- Health Protocols PDFDocument9 pagesHealth Protocols PDFEdz SoncioNo ratings yet
- Maintaiing Non COVID Services in All Hospitals Clinic and Nursing HomesDocument23 pagesMaintaiing Non COVID Services in All Hospitals Clinic and Nursing HomesSanjay BhagwatNo ratings yet
- Republic Act No. 11712 Public Health Emergency Benefits and Allowances For Health Care Workers ActDocument24 pagesRepublic Act No. 11712 Public Health Emergency Benefits and Allowances For Health Care Workers ActgenNo ratings yet
- Maintaining Non COVID Services in All Hospitals Clinic and Nursing HomesDocument23 pagesMaintaining Non COVID Services in All Hospitals Clinic and Nursing HomesSanjay BhagwatNo ratings yet
- Republic The Philippines Health: ClarifyDocument12 pagesRepublic The Philippines Health: ClarifyFret Ramirez Coronia RNNo ratings yet
- AccomplishmentDocument3 pagesAccomplishmentJomar Reuben A. RuecoNo ratings yet
- Ar 2022-23Document228 pagesAr 2022-23PuligalNo ratings yet
- LC05 - Fitz Scientific - SoC - Rev5Document4 pagesLC05 - Fitz Scientific - SoC - Rev5Tarundeep SinghNo ratings yet
- ?.or:r-IIOO (P: of ofDocument9 pages?.or:r-IIOO (P: of ofJayson PaladoNo ratings yet
- Function and Responsibilities of Various Contract of ServiceDocument22 pagesFunction and Responsibilities of Various Contract of ServiceEfren Jr. MateoNo ratings yet
- COVID 19 VACCINATION POLICY With IATF RESOLUTIONSDocument11 pagesCOVID 19 VACCINATION POLICY With IATF RESOLUTIONSImags GamiNo ratings yet
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- China's Novel Coronavirus Response: Guidelines for Governments, Communities, Entities and Individuals to Combat COVID-19From EverandChina's Novel Coronavirus Response: Guidelines for Governments, Communities, Entities and Individuals to Combat COVID-19No ratings yet
- Manual for the Implementation of Environmental, Health, and Safety Standards for the Control of Locusts: December 2021From EverandManual for the Implementation of Environmental, Health, and Safety Standards for the Control of Locusts: December 2021No ratings yet
- Succession Bingo Board SMDocument1 pageSuccession Bingo Board SMToronto StarNo ratings yet
- Bulletin Licence PlateDocument1 pageBulletin Licence PlateToronto StarNo ratings yet
- ETFO AgreementDocument2 pagesETFO AgreementToronto StarNo ratings yet
- Metrolinx - Metrolinx Statement On Eglinton Crosstown LRTDocument1 pageMetrolinx - Metrolinx Statement On Eglinton Crosstown LRTToronto StarNo ratings yet
- Nick Nurse Relieved of Head Coaching DutiesDocument1 pageNick Nurse Relieved of Head Coaching DutiesToronto StarNo ratings yet
- Ruling On Access To Trump ArraignmentDocument6 pagesRuling On Access To Trump ArraignmentToronto StarNo ratings yet
- Play Dressup With Our Royal Paper DollsDocument2 pagesPlay Dressup With Our Royal Paper DollsToronto StarNo ratings yet
- Canadian Forces Administrative Order (CFAO 19-20)Document3 pagesCanadian Forces Administrative Order (CFAO 19-20)Toronto StarNo ratings yet
- Ruling On Access To Trump ArraignmentDocument6 pagesRuling On Access To Trump ArraignmentToronto StarNo ratings yet
- Michele Landsberg Introduces Marian XDocument1 pageMichele Landsberg Introduces Marian XToronto StarNo ratings yet
- Letter Bill 39Document1 pageLetter Bill 39Toronto StarNo ratings yet
- Ontario Deaths in Custody On The Rise 2022Document16 pagesOntario Deaths in Custody On The Rise 2022Toronto StarNo ratings yet
- Affidavit For The FBI Search of President Donald Trump's HomeDocument55 pagesAffidavit For The FBI Search of President Donald Trump's HomeTrisha Powell CrainNo ratings yet
- Pollara EconoOutlook2023Document18 pagesPollara EconoOutlook2023Toronto StarNo ratings yet
- COVID-19 PANDEMIC - Specific COVID-19 Benefits - AG ReportDocument92 pagesCOVID-19 PANDEMIC - Specific COVID-19 Benefits - AG ReportToronto StarNo ratings yet
- Overview Report: Fundraising in Support of ProtestorsDocument61 pagesOverview Report: Fundraising in Support of ProtestorsToronto StarNo ratings yet
- Exhibit # 4 - Doc - Victim Impact Statement From T.kuuzUZDocument2 pagesExhibit # 4 - Doc - Victim Impact Statement From T.kuuzUZToronto StarNo ratings yet
- Dominic Cardy's Resignation LetterDocument2 pagesDominic Cardy's Resignation LetterToronto StarNo ratings yet
- 2022 Dora Award WinnersDocument7 pages2022 Dora Award WinnersToronto Star100% (2)
- Sept. 7 Toronto StarDocument1 pageSept. 7 Toronto StarToronto StarNo ratings yet
- Toronto StarDocument1 pageToronto StarToronto StarNo ratings yet
- Search Warrant MALDocument7 pagesSearch Warrant MALpelofskyj100% (1)
- Exhibit # 5 - Doc - Victim Impact Statement From S. MACKAYDocument1 pageExhibit # 5 - Doc - Victim Impact Statement From S. MACKAYToronto StarNo ratings yet
- Exhibit # 9 - Doc-Victim Impact Statement From M. JUSTINODocument2 pagesExhibit # 9 - Doc-Victim Impact Statement From M. JUSTINOToronto StarNo ratings yet
- Keseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicDocument79 pagesKeseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicdrroytambunanNo ratings yet
- Data and Analysis Considerations in Oncology Clinical TrialsDocument7 pagesData and Analysis Considerations in Oncology Clinical Trialsimk_mithunNo ratings yet
- CONDUCTING FAMILY HEALTH ASSESSMENT TOOL Geno Adrian T. Pampanga BSN-2ADocument11 pagesCONDUCTING FAMILY HEALTH ASSESSMENT TOOL Geno Adrian T. Pampanga BSN-2AGeno Adrian T PampangaNo ratings yet
- Coenzyme Q10 - A Novel MoleculeDocument9 pagesCoenzyme Q10 - A Novel MoleculeArmyiizz OLittlefishoNo ratings yet
- Morphological Study On Torus Palatinus in Adult Human SkullsDocument4 pagesMorphological Study On Torus Palatinus in Adult Human SkullsOttofianus Alvedo Hewick KalangiNo ratings yet
- Massey Bedside ScreenDocument1 pageMassey Bedside ScreenAna Carolina Machuca100% (1)
- Carnitine - WikipediaDocument57 pagesCarnitine - WikipediaMuhammad KashifNo ratings yet
- Intracranial Hemorrage in Term NewbornsDocument35 pagesIntracranial Hemorrage in Term NewbornsHeri suhendraNo ratings yet
- Chung 2016 Stop Bang QuestionnaireDocument8 pagesChung 2016 Stop Bang QuestionnaireDicka adhitya kamilNo ratings yet
- GERBDocument24 pagesGERBdevutty 123No ratings yet
- Are You One of The Obesity Suffers in Indonesia?Document1 pageAre You One of The Obesity Suffers in Indonesia?Titin Evania ManaluNo ratings yet
- 21 40Document6 pages21 40Ira YaoNo ratings yet
- Virus StructureDocument2 pagesVirus Structurewakadur RahmanNo ratings yet
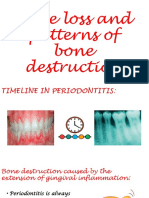
- Bone Loss and Patterns of Bone DestructionDocument21 pagesBone Loss and Patterns of Bone Destructionsonika selvarajNo ratings yet
- Robie Harris Sell SheetDocument2 pagesRobie Harris Sell SheetCandlewick PressNo ratings yet
- Coconut DiseasesDocument32 pagesCoconut Diseasesmohamed ismailNo ratings yet
- Sande's HIV - AIDS Medicine (PDFDrive)Document562 pagesSande's HIV - AIDS Medicine (PDFDrive)angel muñozNo ratings yet
- Techniques For Parasite Egg Identification in Faecal SamplesDocument9 pagesTechniques For Parasite Egg Identification in Faecal SamplesDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (2)
- Biology Hssc-I (3 Set) : SECTION - A (Marks 17) Time Allowed: 25 MinutesDocument10 pagesBiology Hssc-I (3 Set) : SECTION - A (Marks 17) Time Allowed: 25 Minutesوحید حسنNo ratings yet
- The Introduction of Adult Appendicitis Score Reduced Negative Appendectomy RateDocument6 pagesThe Introduction of Adult Appendicitis Score Reduced Negative Appendectomy RateAnonymous V5l8nmcSxbNo ratings yet
- 7th English Science 02Document180 pages7th English Science 02Chaitra KrNo ratings yet
- Employing Vocabulary Instruction For Effective Word Structure and Meaning RecognitionDocument21 pagesEmploying Vocabulary Instruction For Effective Word Structure and Meaning RecognitionWena Fernando Ildefonso100% (1)
- Behavioral and Psychological Symptoms in Alzheimer 'S Dementia and Vascular DementiaDocument28 pagesBehavioral and Psychological Symptoms in Alzheimer 'S Dementia and Vascular DementiaCindy GautamaNo ratings yet
- Prentice9e Im Chap17Document5 pagesPrentice9e Im Chap17api-281340024100% (1)
- Gordons Functional Health Pattern AssessmentDocument5 pagesGordons Functional Health Pattern Assessmentarabellagrace.barrigaNo ratings yet
- Controversies in Treating Cardiogenic ShockDocument59 pagesControversies in Treating Cardiogenic Shockadultmedicalconsultants100% (12)