
Oral Squamous Cell Carcinoma of Tongue: Histological Risk Assessment. A Pilot Study
Oral Squamous Cell Carcinoma of Tongue: Histological Risk Assessment. A Pilot Study
You might also like
- NRG Oncology: RTOG 1308Document84 pagesNRG Oncology: RTOG 1308mark100% (1)
- Contemporary Oral Oncology Diagnosis and ManagementDocument327 pagesContemporary Oral Oncology Diagnosis and ManagementJacky JunaediNo ratings yet
- Lesson Plan On CataractDocument8 pagesLesson Plan On Cataractsimonjosan88% (8)
- 1995 Hellman, Weichselbaum, Weichselbaum OligometastasesDocument4 pages1995 Hellman, Weichselbaum, Weichselbaum OligometastasesPoljarLijanNo ratings yet
- MelanomaDocument6 pagesMelanomaagung permanaNo ratings yet
- Efficacy of Oral and Topical AntioxidantsDocument15 pagesEfficacy of Oral and Topical AntioxidantsJesica SigismondoNo ratings yet
- Chromosomal Instability, DNA Index, Dysplasia, and SubsiteDocument10 pagesChromosomal Instability, DNA Index, Dysplasia, and SubsiteManar AliNo ratings yet
- Mikroba KankerDocument12 pagesMikroba KankerSilpi HamidiyahNo ratings yet
- Risk Factors of Oral Cancer-A Hospital Based Case Control StudyDocument6 pagesRisk Factors of Oral Cancer-A Hospital Based Case Control StudyDevica DR PutriNo ratings yet
- Incidence and Prevalence of Salivary Glands Tumors in Valparaíso, ChileDocument8 pagesIncidence and Prevalence of Salivary Glands Tumors in Valparaíso, ChileJAVIERA HIDALGONo ratings yet
- Laserterapy For Treatment of Oral Mucositis in Patients With Head and Neck CancerDocument17 pagesLaserterapy For Treatment of Oral Mucositis in Patients With Head and Neck CancerarbfilmsNo ratings yet
- Tongue Cancer Pubmed VIIDocument15 pagesTongue Cancer Pubmed VIIAsri Alifa SholehahNo ratings yet
- Jensen Et Al-2014-Journal of Oral Pathology & Medicine PDFDocument10 pagesJensen Et Al-2014-Journal of Oral Pathology & Medicine PDFMega MalyndaNo ratings yet
- Pjms 29 1112Document4 pagesPjms 29 1112Diana IancuNo ratings yet
- Artigo 1 ParacococcidiodomicoseDocument9 pagesArtigo 1 Paracococcidiodomicoseandre.jaccoud2No ratings yet
- Oral Cancer-GeneticsDocument18 pagesOral Cancer-GeneticsAlberto FilhoNo ratings yet
- Articulo 4Document12 pagesArticulo 4Karen CaizaNo ratings yet
- Clinical Histological and Immunohistochemical Study of Colorectal CarcinomaDocument14 pagesClinical Histological and Immunohistochemical Study of Colorectal Carcinomahappymeluckyme3No ratings yet
- 1 s2.0 S0923753419374125 MainDocument7 pages1 s2.0 S0923753419374125 MainGabriela MonteiroNo ratings yet
- Medoral 18 E392Document11 pagesMedoral 18 E392susanti bulanNo ratings yet
- Advances in The Biology of Oral Cancer: P.K. Tsantoulis, N.G. Kastrinakis, A.D. Tourvas, G. Laskaris, V.G. GorgoulisDocument12 pagesAdvances in The Biology of Oral Cancer: P.K. Tsantoulis, N.G. Kastrinakis, A.D. Tourvas, G. Laskaris, V.G. GorgoulisIsabel RamosNo ratings yet
- Hed 44 1481Document11 pagesHed 44 1481dayllyn iglesiasNo ratings yet
- Ebm IpaDocument7 pagesEbm IparivahazmarNo ratings yet
- Wide Field of Cancerization Case Report: February 2017Document5 pagesWide Field of Cancerization Case Report: February 2017Mira AnggrianiNo ratings yet
- 2021 MO Laser CCEODocument8 pages2021 MO Laser CCEOAndressa A.No ratings yet
- Factors Influencing Severity of Medication OsteonecrosisDocument6 pagesFactors Influencing Severity of Medication OsteonecrosisJose IgnacioNo ratings yet
- Cancers 14 04967 v2Document30 pagesCancers 14 04967 v2MARITZA GARCIA JIMENEZNo ratings yet
- BMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanDocument11 pagesBMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanLinaena MericyNo ratings yet
- Squamous Cell Carcinoma of The Oral Tongue in Patients Younger Than 30 Years: Clinicopathologic Features and OutcomeDocument7 pagesSquamous Cell Carcinoma of The Oral Tongue in Patients Younger Than 30 Years: Clinicopathologic Features and OutcomeDew DjengNo ratings yet
- Squamous Cell Carcinoma of The Oral Tongue in Patients Younger Than 30 Years: Clinicopathologic Features and OutcomeDocument7 pagesSquamous Cell Carcinoma of The Oral Tongue in Patients Younger Than 30 Years: Clinicopathologic Features and OutcomeIndahK.WardhaniPutriNo ratings yet
- Original ArticlesDocument7 pagesOriginal ArticlesFernando Emanuel Olmedo BroemserNo ratings yet
- 03 - MACH-NC TumourSite Radio&Onco2011Document8 pages03 - MACH-NC TumourSite Radio&Onco2011Omar SettiNo ratings yet
- JHeadNeckPhysiciansSurg4129-194289 052348Document6 pagesJHeadNeckPhysiciansSurg4129-194289 052348Javeria MNo ratings yet
- Medoralv16 I4 p473Document5 pagesMedoralv16 I4 p473AbhinavNo ratings yet
- HN 04-2011 Sublingual Gland Tumors PDFDocument6 pagesHN 04-2011 Sublingual Gland Tumors PDFHafiz FatmarNo ratings yet
- Clinicopathological Behaviour of Multiple Oral Dysplastic Lesions Compared With That of Single LesionsDocument4 pagesClinicopathological Behaviour of Multiple Oral Dysplastic Lesions Compared With That of Single Lesionsamer_d_89No ratings yet
- Salivary Gland YumorDocument6 pagesSalivary Gland YumorreioctabianoNo ratings yet
- Mouth Cancer Research PaperDocument6 pagesMouth Cancer Research Paperqhujvirhf100% (1)
- Oral Cancer Research PaperDocument4 pagesOral Cancer Research Paperqwmojqund100% (1)
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document8 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Research ParkNo ratings yet
- MicroRNA-based Risk Scoring System To Identify EarDocument14 pagesMicroRNA-based Risk Scoring System To Identify EarDavidNo ratings yet
- BrazilDocument7 pagesBrazilkarinagitakNo ratings yet
- Research Paper On Oral CancerDocument4 pagesResearch Paper On Oral Cancerdyf0g0h0fap3100% (1)
- 2019 WedadDocument8 pages2019 Wedadnermal93No ratings yet
- Introduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"Document11 pagesIntroduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"jesus ulises estrada cantuNo ratings yet
- Epidemiology of Periodontal Older: Disease Among AdultsDocument18 pagesEpidemiology of Periodontal Older: Disease Among AdultsDiana Choiro WNo ratings yet
- Lectura 1 PDFDocument5 pagesLectura 1 PDFCarmen Castillo RequenaNo ratings yet
- 1 s2.0 S1368837518304299 MainDocument8 pages1 s2.0 S1368837518304299 MainIgor VainerNo ratings yet
- Medoral 29 E135Document10 pagesMedoral 29 E135Maria CorenaNo ratings yet
- 10 1016@j Oraloncology 2019 07 012Document10 pages10 1016@j Oraloncology 2019 07 012Parikesit MuhammadNo ratings yet
- Field Cancerization in Oral Lichen PlanusDocument7 pagesField Cancerization in Oral Lichen PlanusAl RawdhaNo ratings yet
- Research ArticleDocument3 pagesResearch ArticleshahrukhNo ratings yet
- Oral Cancer: The First Symptoms and Reasons For Delaying Correct Diagnosis and Appropriate TreatmentDocument9 pagesOral Cancer: The First Symptoms and Reasons For Delaying Correct Diagnosis and Appropriate TreatmentMarekNo ratings yet
- Gaba Et Al 2022 Original Review Article - The Role of Oral Fusobacterium Nucleatum in Female Breast Cancer: A Systematic Review and Meta-AnalysisDocument12 pagesGaba Et Al 2022 Original Review Article - The Role of Oral Fusobacterium Nucleatum in Female Breast Cancer: A Systematic Review and Meta-AnalysisFariah GabaNo ratings yet
- 10.1007@s40368 017 0290 Z 3Document6 pages10.1007@s40368 017 0290 Z 3andi winayaNo ratings yet
- 22826Document9 pages22826Ghina Mukti LuthfiaNo ratings yet
- The Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFDocument7 pagesThe Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFJorge JaraNo ratings yet
- Modern Surgical Management of Tongue Carcinoma - A Clinical Retrospective Research Over A 12 Years PeriodDocument8 pagesModern Surgical Management of Tongue Carcinoma - A Clinical Retrospective Research Over A 12 Years PeriodDian Permana BurlandNo ratings yet
- MDV 484Document26 pagesMDV 484NDJNo ratings yet
- Oral Potentially Malignant Disorders A Consensus Report From An International Seminar On Nomenclature and Classification, ConvenDocument19 pagesOral Potentially Malignant Disorders A Consensus Report From An International Seminar On Nomenclature and Classification, ConvenSophia RochaNo ratings yet
- Tumores Malignos de Anexos CutáneosDocument7 pagesTumores Malignos de Anexos CutáneostisadermaNo ratings yet
- SDJ 2018-05 ResearchDocument11 pagesSDJ 2018-05 ResearchSaifuddin HaswareNo ratings yet
- Chapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartDocument53 pagesChapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartSaifuddin HaswareNo ratings yet
- Mono99 17Document160 pagesMono99 17Saifuddin HaswareNo ratings yet
- Variations of Hair Follicle Size and Distribution in Different Body SitesDocument6 pagesVariations of Hair Follicle Size and Distribution in Different Body SitesSaifuddin HaswareNo ratings yet
- Capture of Hair Geometry From Multiple ImagesDocument8 pagesCapture of Hair Geometry From Multiple ImagesSaifuddin HaswareNo ratings yet
- Psoriasis and Cardiovascular Disease: Where Is The Risk?: CommentaryDocument4 pagesPsoriasis and Cardiovascular Disease: Where Is The Risk?: CommentarySaifuddin HaswareNo ratings yet
- JCDP 20 444Document5 pagesJCDP 20 444Saifuddin HaswareNo ratings yet
- Cheng JARODocument15 pagesCheng JAROSaifuddin HaswareNo ratings yet
- Crisp1 and Alopecia Areata in C3H/Hej Mice: Crisp1/Crisp1, Cysteine-Rich Secretory Protein 1, Gene/Protein Crisp1Document12 pagesCrisp1 and Alopecia Areata in C3H/Hej Mice: Crisp1/Crisp1, Cysteine-Rich Secretory Protein 1, Gene/Protein Crisp1Saifuddin HaswareNo ratings yet
- 286 FullDocument8 pages286 FullSaifuddin HaswareNo ratings yet
- Splenic Melanosis During Normal Murine C57BL/6 Hair Cycle and After ChemotherapyDocument9 pagesSplenic Melanosis During Normal Murine C57BL/6 Hair Cycle and After ChemotherapySaifuddin HaswareNo ratings yet
- Adenovirus-Mediated Wnt5a Expression Inhibits The Telogen-To-Anagen Transition of Hair Follicles in MiceDocument7 pagesAdenovirus-Mediated Wnt5a Expression Inhibits The Telogen-To-Anagen Transition of Hair Follicles in MiceSaifuddin HaswareNo ratings yet
- Inexhaustible Hair-Cell Regeneration in Young and Aged ZebrafishDocument7 pagesInexhaustible Hair-Cell Regeneration in Young and Aged ZebrafishSaifuddin HaswareNo ratings yet
- Noise Induced Loss of Hair Cells and Cochlear Synaptopathy Are Mediated by The Activation of AMPKDocument14 pagesNoise Induced Loss of Hair Cells and Cochlear Synaptopathy Are Mediated by The Activation of AMPKSaifuddin HaswareNo ratings yet
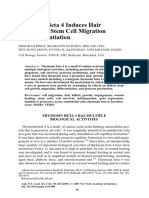
- Thymosin Beta 4 Induces Hair Growth Via Stem Cell Migration and DifferentiationDocument9 pagesThymosin Beta 4 Induces Hair Growth Via Stem Cell Migration and DifferentiationSaifuddin HaswareNo ratings yet
- Hair Cortisol Analyses in Different Mammal Species: Choosing The Wrong Assay May Lead To Erroneous ResultsDocument15 pagesHair Cortisol Analyses in Different Mammal Species: Choosing The Wrong Assay May Lead To Erroneous ResultsSaifuddin HaswareNo ratings yet
- Uncombable Hair SyndromeDocument3 pagesUncombable Hair SyndromeSaifuddin HaswareNo ratings yet
- Anisotropic Elastoplasticity For Cloth, Knit and Hair Frictional ContactDocument14 pagesAnisotropic Elastoplasticity For Cloth, Knit and Hair Frictional ContactSaifuddin HaswareNo ratings yet
- September 2013 BourlandDocument38 pagesSeptember 2013 BourlandSaifuddin HaswareNo ratings yet
- Root Hair Mutants of BarleyDocument6 pagesRoot Hair Mutants of BarleySaifuddin HaswareNo ratings yet
- Histological and Molecular Aspects of Oral Squamous Cell Carcinoma (Review)Document5 pagesHistological and Molecular Aspects of Oral Squamous Cell Carcinoma (Review)Yeni PuspitasariNo ratings yet
- An In-Depth Look at Krukenberg TumorDocument6 pagesAn In-Depth Look at Krukenberg Tumor垂直马克No ratings yet
- Cancers 16 00006Document13 pagesCancers 16 00006Team Check88No ratings yet
- Cervical CancerDocument2 pagesCervical Cancergilpogs0% (1)
- Cancer:causes and TreatmentsDocument15 pagesCancer:causes and TreatmentskashirokoshiroNo ratings yet
- Dr. Wifanto-Management Liver Metastasis CRCDocument46 pagesDr. Wifanto-Management Liver Metastasis CRCAfkar30No ratings yet
- Thyroid NeoplasmsDocument62 pagesThyroid Neoplasmshemanarasimha gandikotaNo ratings yet
- Soft Tissue SarcomaDocument45 pagesSoft Tissue SarcomaWadhe TobingNo ratings yet
- The OncologistDocument7 pagesThe OncologistManunart FeungpeanNo ratings yet
- BB5506: The Biology, Genetics and Treatment of Human CancerDocument54 pagesBB5506: The Biology, Genetics and Treatment of Human Cancerpriyaa100% (1)
- OncologyDocument149 pagesOncologyAnonymous uCOxeD1q100% (1)
- What To Know About CancerDocument17 pagesWhat To Know About CancerKARL PASCUANo ratings yet
- Brest Lump History TakingDocument3 pagesBrest Lump History Takinganon_619577898No ratings yet
- Euromedlab 2013 Abstracts 211 and 219Document103 pagesEuromedlab 2013 Abstracts 211 and 219Jagannadha Rao PeelaNo ratings yet
- Tumor Marker DENDocument12 pagesTumor Marker DENArtheswara SidhajatiNo ratings yet
- Gamma Knife1Document17 pagesGamma Knife1api-247561652No ratings yet
- Patho of Invasive Duct CarcinomaDocument3 pagesPatho of Invasive Duct CarcinomaBESA JERIC FLORESNo ratings yet
- P Reddy SAJS 2017Document6 pagesP Reddy SAJS 2017Sumayyah EbrahimNo ratings yet
- Professionalsphysician Glspdfovarian PDFDocument241 pagesProfessionalsphysician Glspdfovarian PDFfrancisco248ramonNo ratings yet
- Final Scientific ScheduleDocument7 pagesFinal Scientific SchedulesaikrishnamedicoNo ratings yet
- MBBS Pathology-High-Yield TopicsDocument8 pagesMBBS Pathology-High-Yield TopicsRohith ReddyNo ratings yet
- Prostate Cancer: Presented By, Denna Benny Roll. No:21 3 Year B. SC NursingDocument58 pagesProstate Cancer: Presented By, Denna Benny Roll. No:21 3 Year B. SC NursingSamuel LalNo ratings yet
- Segment III Bypass 18 407Document23 pagesSegment III Bypass 18 407riskywhiskyNo ratings yet
- Study Protocol of A Randomised Controlled Trial of Prostate Radiotherapy in High-Risk and Node-Positive Disease Comparing Moderate and Extreme Hypofractionation (PRIME TRIAL)Document8 pagesStudy Protocol of A Randomised Controlled Trial of Prostate Radiotherapy in High-Risk and Node-Positive Disease Comparing Moderate and Extreme Hypofractionation (PRIME TRIAL)William trincaNo ratings yet
- Radiotherapy: IPEM Grade A' Training PortfolioDocument9 pagesRadiotherapy: IPEM Grade A' Training PortfoliorodricesarNo ratings yet
- Basal Cell Carcinoma Squamous Cell Carcinoma Guide Nov 2008-Final With CorrigendumsDocument183 pagesBasal Cell Carcinoma Squamous Cell Carcinoma Guide Nov 2008-Final With CorrigendumsBoofy27No ratings yet
- Structure and Format Icd-ODocument23 pagesStructure and Format Icd-OhendryfransiskusNo ratings yet











































































































Download as pdf or txt
You might also like
- NRG Oncology: RTOG 1308Document84 pagesNRG Oncology: RTOG 1308mark100% (1)
- Contemporary Oral Oncology Diagnosis and ManagementDocument327 pagesContemporary Oral Oncology Diagnosis and ManagementJacky JunaediNo ratings yet
- Lesson Plan On CataractDocument8 pagesLesson Plan On Cataractsimonjosan88% (8)
- 1995 Hellman, Weichselbaum, Weichselbaum OligometastasesDocument4 pages1995 Hellman, Weichselbaum, Weichselbaum OligometastasesPoljarLijanNo ratings yet
- MelanomaDocument6 pagesMelanomaagung permanaNo ratings yet
- Efficacy of Oral and Topical AntioxidantsDocument15 pagesEfficacy of Oral and Topical AntioxidantsJesica SigismondoNo ratings yet
- Chromosomal Instability, DNA Index, Dysplasia, and SubsiteDocument10 pagesChromosomal Instability, DNA Index, Dysplasia, and SubsiteManar AliNo ratings yet
- Mikroba KankerDocument12 pagesMikroba KankerSilpi HamidiyahNo ratings yet
- Risk Factors of Oral Cancer-A Hospital Based Case Control StudyDocument6 pagesRisk Factors of Oral Cancer-A Hospital Based Case Control StudyDevica DR PutriNo ratings yet
- Incidence and Prevalence of Salivary Glands Tumors in Valparaíso, ChileDocument8 pagesIncidence and Prevalence of Salivary Glands Tumors in Valparaíso, ChileJAVIERA HIDALGONo ratings yet
- Laserterapy For Treatment of Oral Mucositis in Patients With Head and Neck CancerDocument17 pagesLaserterapy For Treatment of Oral Mucositis in Patients With Head and Neck CancerarbfilmsNo ratings yet
- Tongue Cancer Pubmed VIIDocument15 pagesTongue Cancer Pubmed VIIAsri Alifa SholehahNo ratings yet
- Jensen Et Al-2014-Journal of Oral Pathology & Medicine PDFDocument10 pagesJensen Et Al-2014-Journal of Oral Pathology & Medicine PDFMega MalyndaNo ratings yet
- Pjms 29 1112Document4 pagesPjms 29 1112Diana IancuNo ratings yet
- Artigo 1 ParacococcidiodomicoseDocument9 pagesArtigo 1 Paracococcidiodomicoseandre.jaccoud2No ratings yet
- Oral Cancer-GeneticsDocument18 pagesOral Cancer-GeneticsAlberto FilhoNo ratings yet
- Articulo 4Document12 pagesArticulo 4Karen CaizaNo ratings yet
- Clinical Histological and Immunohistochemical Study of Colorectal CarcinomaDocument14 pagesClinical Histological and Immunohistochemical Study of Colorectal Carcinomahappymeluckyme3No ratings yet
- 1 s2.0 S0923753419374125 MainDocument7 pages1 s2.0 S0923753419374125 MainGabriela MonteiroNo ratings yet
- Medoral 18 E392Document11 pagesMedoral 18 E392susanti bulanNo ratings yet
- Advances in The Biology of Oral Cancer: P.K. Tsantoulis, N.G. Kastrinakis, A.D. Tourvas, G. Laskaris, V.G. GorgoulisDocument12 pagesAdvances in The Biology of Oral Cancer: P.K. Tsantoulis, N.G. Kastrinakis, A.D. Tourvas, G. Laskaris, V.G. GorgoulisIsabel RamosNo ratings yet
- Hed 44 1481Document11 pagesHed 44 1481dayllyn iglesiasNo ratings yet
- Ebm IpaDocument7 pagesEbm IparivahazmarNo ratings yet
- Wide Field of Cancerization Case Report: February 2017Document5 pagesWide Field of Cancerization Case Report: February 2017Mira AnggrianiNo ratings yet
- 2021 MO Laser CCEODocument8 pages2021 MO Laser CCEOAndressa A.No ratings yet
- Factors Influencing Severity of Medication OsteonecrosisDocument6 pagesFactors Influencing Severity of Medication OsteonecrosisJose IgnacioNo ratings yet
- Cancers 14 04967 v2Document30 pagesCancers 14 04967 v2MARITZA GARCIA JIMENEZNo ratings yet
- BMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanDocument11 pagesBMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanLinaena MericyNo ratings yet
- Squamous Cell Carcinoma of The Oral Tongue in Patients Younger Than 30 Years: Clinicopathologic Features and OutcomeDocument7 pagesSquamous Cell Carcinoma of The Oral Tongue in Patients Younger Than 30 Years: Clinicopathologic Features and OutcomeDew DjengNo ratings yet
- Squamous Cell Carcinoma of The Oral Tongue in Patients Younger Than 30 Years: Clinicopathologic Features and OutcomeDocument7 pagesSquamous Cell Carcinoma of The Oral Tongue in Patients Younger Than 30 Years: Clinicopathologic Features and OutcomeIndahK.WardhaniPutriNo ratings yet
- Original ArticlesDocument7 pagesOriginal ArticlesFernando Emanuel Olmedo BroemserNo ratings yet
- 03 - MACH-NC TumourSite Radio&Onco2011Document8 pages03 - MACH-NC TumourSite Radio&Onco2011Omar SettiNo ratings yet
- JHeadNeckPhysiciansSurg4129-194289 052348Document6 pagesJHeadNeckPhysiciansSurg4129-194289 052348Javeria MNo ratings yet
- Medoralv16 I4 p473Document5 pagesMedoralv16 I4 p473AbhinavNo ratings yet
- HN 04-2011 Sublingual Gland Tumors PDFDocument6 pagesHN 04-2011 Sublingual Gland Tumors PDFHafiz FatmarNo ratings yet
- Clinicopathological Behaviour of Multiple Oral Dysplastic Lesions Compared With That of Single LesionsDocument4 pagesClinicopathological Behaviour of Multiple Oral Dysplastic Lesions Compared With That of Single Lesionsamer_d_89No ratings yet
- Salivary Gland YumorDocument6 pagesSalivary Gland YumorreioctabianoNo ratings yet
- Mouth Cancer Research PaperDocument6 pagesMouth Cancer Research Paperqhujvirhf100% (1)
- Oral Cancer Research PaperDocument4 pagesOral Cancer Research Paperqwmojqund100% (1)
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document8 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Research ParkNo ratings yet
- MicroRNA-based Risk Scoring System To Identify EarDocument14 pagesMicroRNA-based Risk Scoring System To Identify EarDavidNo ratings yet
- BrazilDocument7 pagesBrazilkarinagitakNo ratings yet
- Research Paper On Oral CancerDocument4 pagesResearch Paper On Oral Cancerdyf0g0h0fap3100% (1)
- 2019 WedadDocument8 pages2019 Wedadnermal93No ratings yet
- Introduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"Document11 pagesIntroduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"jesus ulises estrada cantuNo ratings yet
- Epidemiology of Periodontal Older: Disease Among AdultsDocument18 pagesEpidemiology of Periodontal Older: Disease Among AdultsDiana Choiro WNo ratings yet
- Lectura 1 PDFDocument5 pagesLectura 1 PDFCarmen Castillo RequenaNo ratings yet
- 1 s2.0 S1368837518304299 MainDocument8 pages1 s2.0 S1368837518304299 MainIgor VainerNo ratings yet
- Medoral 29 E135Document10 pagesMedoral 29 E135Maria CorenaNo ratings yet
- 10 1016@j Oraloncology 2019 07 012Document10 pages10 1016@j Oraloncology 2019 07 012Parikesit MuhammadNo ratings yet
- Field Cancerization in Oral Lichen PlanusDocument7 pagesField Cancerization in Oral Lichen PlanusAl RawdhaNo ratings yet
- Research ArticleDocument3 pagesResearch ArticleshahrukhNo ratings yet
- Oral Cancer: The First Symptoms and Reasons For Delaying Correct Diagnosis and Appropriate TreatmentDocument9 pagesOral Cancer: The First Symptoms and Reasons For Delaying Correct Diagnosis and Appropriate TreatmentMarekNo ratings yet
- Gaba Et Al 2022 Original Review Article - The Role of Oral Fusobacterium Nucleatum in Female Breast Cancer: A Systematic Review and Meta-AnalysisDocument12 pagesGaba Et Al 2022 Original Review Article - The Role of Oral Fusobacterium Nucleatum in Female Breast Cancer: A Systematic Review and Meta-AnalysisFariah GabaNo ratings yet
- 10.1007@s40368 017 0290 Z 3Document6 pages10.1007@s40368 017 0290 Z 3andi winayaNo ratings yet
- 22826Document9 pages22826Ghina Mukti LuthfiaNo ratings yet
- The Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFDocument7 pagesThe Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFJorge JaraNo ratings yet
- Modern Surgical Management of Tongue Carcinoma - A Clinical Retrospective Research Over A 12 Years PeriodDocument8 pagesModern Surgical Management of Tongue Carcinoma - A Clinical Retrospective Research Over A 12 Years PeriodDian Permana BurlandNo ratings yet
- MDV 484Document26 pagesMDV 484NDJNo ratings yet
- Oral Potentially Malignant Disorders A Consensus Report From An International Seminar On Nomenclature and Classification, ConvenDocument19 pagesOral Potentially Malignant Disorders A Consensus Report From An International Seminar On Nomenclature and Classification, ConvenSophia RochaNo ratings yet
- Tumores Malignos de Anexos CutáneosDocument7 pagesTumores Malignos de Anexos CutáneostisadermaNo ratings yet
- SDJ 2018-05 ResearchDocument11 pagesSDJ 2018-05 ResearchSaifuddin HaswareNo ratings yet
- Chapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartDocument53 pagesChapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartSaifuddin HaswareNo ratings yet
- Mono99 17Document160 pagesMono99 17Saifuddin HaswareNo ratings yet
- Variations of Hair Follicle Size and Distribution in Different Body SitesDocument6 pagesVariations of Hair Follicle Size and Distribution in Different Body SitesSaifuddin HaswareNo ratings yet
- Capture of Hair Geometry From Multiple ImagesDocument8 pagesCapture of Hair Geometry From Multiple ImagesSaifuddin HaswareNo ratings yet
- Psoriasis and Cardiovascular Disease: Where Is The Risk?: CommentaryDocument4 pagesPsoriasis and Cardiovascular Disease: Where Is The Risk?: CommentarySaifuddin HaswareNo ratings yet
- JCDP 20 444Document5 pagesJCDP 20 444Saifuddin HaswareNo ratings yet
- Cheng JARODocument15 pagesCheng JAROSaifuddin HaswareNo ratings yet
- Crisp1 and Alopecia Areata in C3H/Hej Mice: Crisp1/Crisp1, Cysteine-Rich Secretory Protein 1, Gene/Protein Crisp1Document12 pagesCrisp1 and Alopecia Areata in C3H/Hej Mice: Crisp1/Crisp1, Cysteine-Rich Secretory Protein 1, Gene/Protein Crisp1Saifuddin HaswareNo ratings yet
- 286 FullDocument8 pages286 FullSaifuddin HaswareNo ratings yet
- Splenic Melanosis During Normal Murine C57BL/6 Hair Cycle and After ChemotherapyDocument9 pagesSplenic Melanosis During Normal Murine C57BL/6 Hair Cycle and After ChemotherapySaifuddin HaswareNo ratings yet
- Adenovirus-Mediated Wnt5a Expression Inhibits The Telogen-To-Anagen Transition of Hair Follicles in MiceDocument7 pagesAdenovirus-Mediated Wnt5a Expression Inhibits The Telogen-To-Anagen Transition of Hair Follicles in MiceSaifuddin HaswareNo ratings yet
- Inexhaustible Hair-Cell Regeneration in Young and Aged ZebrafishDocument7 pagesInexhaustible Hair-Cell Regeneration in Young and Aged ZebrafishSaifuddin HaswareNo ratings yet
- Noise Induced Loss of Hair Cells and Cochlear Synaptopathy Are Mediated by The Activation of AMPKDocument14 pagesNoise Induced Loss of Hair Cells and Cochlear Synaptopathy Are Mediated by The Activation of AMPKSaifuddin HaswareNo ratings yet
- Thymosin Beta 4 Induces Hair Growth Via Stem Cell Migration and DifferentiationDocument9 pagesThymosin Beta 4 Induces Hair Growth Via Stem Cell Migration and DifferentiationSaifuddin HaswareNo ratings yet
- Hair Cortisol Analyses in Different Mammal Species: Choosing The Wrong Assay May Lead To Erroneous ResultsDocument15 pagesHair Cortisol Analyses in Different Mammal Species: Choosing The Wrong Assay May Lead To Erroneous ResultsSaifuddin HaswareNo ratings yet
- Uncombable Hair SyndromeDocument3 pagesUncombable Hair SyndromeSaifuddin HaswareNo ratings yet
- Anisotropic Elastoplasticity For Cloth, Knit and Hair Frictional ContactDocument14 pagesAnisotropic Elastoplasticity For Cloth, Knit and Hair Frictional ContactSaifuddin HaswareNo ratings yet
- September 2013 BourlandDocument38 pagesSeptember 2013 BourlandSaifuddin HaswareNo ratings yet
- Root Hair Mutants of BarleyDocument6 pagesRoot Hair Mutants of BarleySaifuddin HaswareNo ratings yet
- Histological and Molecular Aspects of Oral Squamous Cell Carcinoma (Review)Document5 pagesHistological and Molecular Aspects of Oral Squamous Cell Carcinoma (Review)Yeni PuspitasariNo ratings yet
- An In-Depth Look at Krukenberg TumorDocument6 pagesAn In-Depth Look at Krukenberg Tumor垂直马克No ratings yet
- Cancers 16 00006Document13 pagesCancers 16 00006Team Check88No ratings yet
- Cervical CancerDocument2 pagesCervical Cancergilpogs0% (1)
- Cancer:causes and TreatmentsDocument15 pagesCancer:causes and TreatmentskashirokoshiroNo ratings yet
- Dr. Wifanto-Management Liver Metastasis CRCDocument46 pagesDr. Wifanto-Management Liver Metastasis CRCAfkar30No ratings yet
- Thyroid NeoplasmsDocument62 pagesThyroid Neoplasmshemanarasimha gandikotaNo ratings yet
- Soft Tissue SarcomaDocument45 pagesSoft Tissue SarcomaWadhe TobingNo ratings yet
- The OncologistDocument7 pagesThe OncologistManunart FeungpeanNo ratings yet
- BB5506: The Biology, Genetics and Treatment of Human CancerDocument54 pagesBB5506: The Biology, Genetics and Treatment of Human Cancerpriyaa100% (1)
- OncologyDocument149 pagesOncologyAnonymous uCOxeD1q100% (1)
- What To Know About CancerDocument17 pagesWhat To Know About CancerKARL PASCUANo ratings yet
- Brest Lump History TakingDocument3 pagesBrest Lump History Takinganon_619577898No ratings yet
- Euromedlab 2013 Abstracts 211 and 219Document103 pagesEuromedlab 2013 Abstracts 211 and 219Jagannadha Rao PeelaNo ratings yet
- Tumor Marker DENDocument12 pagesTumor Marker DENArtheswara SidhajatiNo ratings yet
- Gamma Knife1Document17 pagesGamma Knife1api-247561652No ratings yet
- Patho of Invasive Duct CarcinomaDocument3 pagesPatho of Invasive Duct CarcinomaBESA JERIC FLORESNo ratings yet
- P Reddy SAJS 2017Document6 pagesP Reddy SAJS 2017Sumayyah EbrahimNo ratings yet
- Professionalsphysician Glspdfovarian PDFDocument241 pagesProfessionalsphysician Glspdfovarian PDFfrancisco248ramonNo ratings yet
- Final Scientific ScheduleDocument7 pagesFinal Scientific SchedulesaikrishnamedicoNo ratings yet
- MBBS Pathology-High-Yield TopicsDocument8 pagesMBBS Pathology-High-Yield TopicsRohith ReddyNo ratings yet
- Prostate Cancer: Presented By, Denna Benny Roll. No:21 3 Year B. SC NursingDocument58 pagesProstate Cancer: Presented By, Denna Benny Roll. No:21 3 Year B. SC NursingSamuel LalNo ratings yet
- Segment III Bypass 18 407Document23 pagesSegment III Bypass 18 407riskywhiskyNo ratings yet
- Study Protocol of A Randomised Controlled Trial of Prostate Radiotherapy in High-Risk and Node-Positive Disease Comparing Moderate and Extreme Hypofractionation (PRIME TRIAL)Document8 pagesStudy Protocol of A Randomised Controlled Trial of Prostate Radiotherapy in High-Risk and Node-Positive Disease Comparing Moderate and Extreme Hypofractionation (PRIME TRIAL)William trincaNo ratings yet
- Radiotherapy: IPEM Grade A' Training PortfolioDocument9 pagesRadiotherapy: IPEM Grade A' Training PortfoliorodricesarNo ratings yet
- Basal Cell Carcinoma Squamous Cell Carcinoma Guide Nov 2008-Final With CorrigendumsDocument183 pagesBasal Cell Carcinoma Squamous Cell Carcinoma Guide Nov 2008-Final With CorrigendumsBoofy27No ratings yet
- Structure and Format Icd-ODocument23 pagesStructure and Format Icd-OhendryfransiskusNo ratings yet