
ClubfootBrochure Kaki Pengkor
ClubfootBrochure Kaki Pengkor
You might also like
- ASTA Membership Directory 2022Document18 pagesASTA Membership Directory 2022Vasanthi Muthayan100% (1)
- Pediatric Potpourri 200+ New CPEN Questions: Certified Pediatric Emergency Nurse Review (3rd Edition Supplement)From EverandPediatric Potpourri 200+ New CPEN Questions: Certified Pediatric Emergency Nurse Review (3rd Edition Supplement)No ratings yet
- Actividad A4. Study CaseDocument2 pagesActividad A4. Study CaseDavid Padilla AcostaNo ratings yet
- Objectives CLUB FOOTDocument2 pagesObjectives CLUB FOOTAdriano SonnyNo ratings yet
- Club FootDocument3 pagesClub FootKim GalamgamNo ratings yet
- Club FootDocument5 pagesClub FootanisadestyaNo ratings yet
- Clubfoot: Lady Diane M. Cabriga Bsn-IiiDocument7 pagesClubfoot: Lady Diane M. Cabriga Bsn-IiiDayan CabrigaNo ratings yet
- Clubfoot: What Is A Clubfoot?Document1 pageClubfoot: What Is A Clubfoot?Joshua MccrayNo ratings yet
- Talipes Deformity or ClubfootDocument5 pagesTalipes Deformity or ClubfootcrisolandNo ratings yet
- ClubfootDocument5 pagesClubfootCherry AlmarezNo ratings yet
- Clubfoot ThesisDocument7 pagesClubfoot ThesisCollegePaperGhostWriterAkron100% (2)
- Scoliosis Surgery: Preparing For Surgery and A Hospital StayDocument9 pagesScoliosis Surgery: Preparing For Surgery and A Hospital StayFaris Aziz PridiantoNo ratings yet
- Physical Therapy in Corpus Christi For Pediatric Issues: Guide To Clubfoot MenuDocument17 pagesPhysical Therapy in Corpus Christi For Pediatric Issues: Guide To Clubfoot MenunovialbarNo ratings yet
- Symptoms: If Your Child Has Clubfoot, Here's What It Might Look LikeDocument112 pagesSymptoms: If Your Child Has Clubfoot, Here's What It Might Look LikeSantosh RudraNo ratings yet
- Physical Therapy in Corpus Christi For Pediatric Issues: Guide To Clubfoot MenuDocument17 pagesPhysical Therapy in Corpus Christi For Pediatric Issues: Guide To Clubfoot MenuHusna NadiaNo ratings yet
- ClubfootDocument22 pagesClubfootJhong Xyrus100% (3)
- ClubfootDocument12 pagesClubfootjoycesiosonNo ratings yet
- Adduction and Equinus.: Citation NeededDocument16 pagesAdduction and Equinus.: Citation NeededMaria Ardhail Dasalla RagodonNo ratings yet
- Developmental Dysplasia of The Hip, (DDH) Including Femoral and Pelvic OsteotomyDocument16 pagesDevelopmental Dysplasia of The Hip, (DDH) Including Femoral and Pelvic OsteotomyAkbar GazaliNo ratings yet
- Clubfoot - The Ponseti MethodDocument4 pagesClubfoot - The Ponseti MethodJerry Kurnia WahyudiNo ratings yet
- CLUBFOOTDocument19 pagesCLUBFOOTKaryn Joy LamisNo ratings yet
- ClubfootDocument27 pagesClubfootPrashanth K NairNo ratings yet
- Case StudyDocument11 pagesCase StudyAnj TadxNo ratings yet
- A. Skeletal System: Child Born With Physical/ Developmental ChallengeDocument10 pagesA. Skeletal System: Child Born With Physical/ Developmental ChallengeHazel NialaNo ratings yet
- Litrev ClubfootDocument6 pagesLitrev Clubfootdedyalkarni08No ratings yet
- CLUB FootDocument4 pagesCLUB FootDarwin Dux Lacson DimarucutNo ratings yet
- ClubfootDocument9 pagesClubfootLorebell100% (5)
- Slipped Upper Femoral Epiphysis: Child Health Information FactsheetDocument2 pagesSlipped Upper Femoral Epiphysis: Child Health Information FactsheetNurusshiami KhairatiNo ratings yet
- Help CfparentsDocument3 pagesHelp CfparentsjessgabNo ratings yet
- A Parents Guide To Treatment For Development Dysplasia of The HipDocument16 pagesA Parents Guide To Treatment For Development Dysplasia of The HipSunny Gabriels100% (1)
- Legg Perthes Disease What Is Legg-Perthes Disease?Document6 pagesLegg Perthes Disease What Is Legg-Perthes Disease?readerkellNo ratings yet
- Vincent Mosca - Clubfoot Guide For ParentsDocument3 pagesVincent Mosca - Clubfoot Guide For ParentsCatalin FloreaNo ratings yet
- ClubfootDocument27 pagesClubfootJaya Prabha100% (1)
- Club Foot: Ison, Kevin Christian B. BSN3D1Document27 pagesClub Foot: Ison, Kevin Christian B. BSN3D1Saputro AbdiNo ratings yet
- Diagnosing DDHDocument3 pagesDiagnosing DDHNylia AtibiNo ratings yet
- CONGENITAL TALIPES EQUINOVARUS in PMRDocument31 pagesCONGENITAL TALIPES EQUINOVARUS in PMRrachmadyNo ratings yet
- Congenital Hip DislocationDocument8 pagesCongenital Hip DislocationadrianojenfferNo ratings yet
- Developmental Dislocation (Dysplasia) of The Hip (DDH) : DescriptionDocument4 pagesDevelopmental Dislocation (Dysplasia) of The Hip (DDH) : DescriptiondfdnNo ratings yet
- Information For Patients Following Knee Arthroscopy: Therapies DirectorateDocument6 pagesInformation For Patients Following Knee Arthroscopy: Therapies Directoratepecson1No ratings yet
- Full Thickness Bowel Biopsy F1555 A4 BW FINAL Dec18Document2 pagesFull Thickness Bowel Biopsy F1555 A4 BW FINAL Dec18Nimra WaheedNo ratings yet
- HirschzxcxzcDocument2 pagesHirschzxcxzcZNEROLNo ratings yet
- Symptoms of Talipes DiseaseDocument6 pagesSymptoms of Talipes DiseaseJustine DumaguinNo ratings yet
- Eastern African International CollegeDocument5 pagesEastern African International CollegeDire DireNo ratings yet
- Beyond The Basics: Dr. Amna HaiderDocument29 pagesBeyond The Basics: Dr. Amna Haiderrabia khalidNo ratings yet
- Congenital-Torticollis (Wry Neck)Document57 pagesCongenital-Torticollis (Wry Neck)Shafiq Mohd NorNo ratings yet
- Splinting LeafletDocument2 pagesSplinting LeafletAbhishek GuptaNo ratings yet
- Scoliosis Surgery: Goals of The SurgeryDocument4 pagesScoliosis Surgery: Goals of The SurgeryFaris Aziz PridiantoNo ratings yet
- Developmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedDocument37 pagesDevelopmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedAh ZhangNo ratings yet
- CHD 1sDocument32 pagesCHD 1sLauNo ratings yet
- Perthes Disease - SurgeryDocument10 pagesPerthes Disease - SurgeryEla TINo ratings yet
- Congenital Talipes Equinovarus (Clubfoot)Document4 pagesCongenital Talipes Equinovarus (Clubfoot)Julliza Joy PandiNo ratings yet
- Club Foot: 1 Genetics 2 DiagnosisDocument8 pagesClub Foot: 1 Genetics 2 DiagnosispaulNo ratings yet
- Congenital Talipes EquinovarusDocument25 pagesCongenital Talipes EquinovarusArlyn MillanesNo ratings yet
- What Is Bladder Exstrophy?Document6 pagesWhat Is Bladder Exstrophy?preveennaNo ratings yet
- Rehab After OsteotomyDocument2 pagesRehab After OsteotomyMiguel OrdoñezNo ratings yet
- Knock Knees Genu Valgum: by DR - Abdullah AlmusallamDocument17 pagesKnock Knees Genu Valgum: by DR - Abdullah AlmusallamDrAbdullah AlmusallamNo ratings yet
- Clubfoot Written ReportDocument7 pagesClubfoot Written ReportAira Madel ArabaNo ratings yet
- Clubfoot - The Ponseti Method: Dale Elizabeth Jarka, MD, CM, FRCS (C)Document87 pagesClubfoot - The Ponseti Method: Dale Elizabeth Jarka, MD, CM, FRCS (C)muthia saniNo ratings yet
- Amp PedDocument118 pagesAmp PedElla ArusteiNo ratings yet
- Clubfoot Orthotic William Porter: Alexis Wickwire Erika Franzen Dr. Morey Moreland 02/08/2005Document11 pagesClubfoot Orthotic William Porter: Alexis Wickwire Erika Franzen Dr. Morey Moreland 02/08/2005Ay HaanNo ratings yet
- Club FootDocument11 pagesClub FootdrusmanjamilhcmdNo ratings yet
- If they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.From EverandIf they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.No ratings yet
- THE INDEPENDENT Issue 558Document44 pagesTHE INDEPENDENT Issue 558The Independent MagazineNo ratings yet
- The Role of EEG in The Diagnosis and Classification of The Epilepsy Syndromes (Part 1)Document66 pagesThe Role of EEG in The Diagnosis and Classification of The Epilepsy Syndromes (Part 1)Rosmery VillaNo ratings yet
- IS0125 F Fuel-ManagerDocument12 pagesIS0125 F Fuel-ManagerBilly12369No ratings yet
- Eq - 333Document1 pageEq - 333Franco SNo ratings yet
- Waste To Energy Potential in The Wastern Province of Saudi ArabiaDocument9 pagesWaste To Energy Potential in The Wastern Province of Saudi ArabiaahaaNo ratings yet
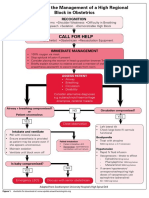
- Algorithm For The Management of A High Regional Block in ObstetricsDocument5 pagesAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNo ratings yet
- Final Exam QuestionsDocument4 pagesFinal Exam QuestionsAndil MaulanaNo ratings yet
- Comprehensive Report Card: About The Problems of Sub-Health TrendsDocument3 pagesComprehensive Report Card: About The Problems of Sub-Health TrendsFitriWidiastutiNo ratings yet
- Nepro Plastics Pvc4Document12 pagesNepro Plastics Pvc4chaouch.najehNo ratings yet
- Clinical Nutrition: Paediatric Nutrition Risk Scores in Clinical Practice: Children With Inflammatory Bowel DiseaseDocument4 pagesClinical Nutrition: Paediatric Nutrition Risk Scores in Clinical Practice: Children With Inflammatory Bowel DiseaseMaggie S HungNo ratings yet
- EcoDocument7 pagesEcoSushma YonzenNo ratings yet
- Laser Safety Test !Document5 pagesLaser Safety Test !shabeer hassimNo ratings yet
- COVID-19 and Disinfectants and Sanitizers in Food PremisesDocument5 pagesCOVID-19 and Disinfectants and Sanitizers in Food Premisesnur atiqah sobriNo ratings yet
- Transducer Engineering 2 Marks With AnswersDocument13 pagesTransducer Engineering 2 Marks With AnswersSridharan DNo ratings yet
- Construction and Installation of De-Icer BootsDocument11 pagesConstruction and Installation of De-Icer BootsPatrick dela rosaNo ratings yet
- Moving To A World Beyond P 0 05Document20 pagesMoving To A World Beyond P 0 05Frank LopezNo ratings yet
- Case Ih Tractor 1070 Operators Manual 9 2822Document22 pagesCase Ih Tractor 1070 Operators Manual 9 2822zacharygonzalez130703jse100% (140)
- The Microbiota in Cirrhosis and Its Role in Hepatic Decompensation. 2020Document15 pagesThe Microbiota in Cirrhosis and Its Role in Hepatic Decompensation. 2020mafe.z.solarte87No ratings yet
- Nitomortar FC Base - SDS11608 - 44Document13 pagesNitomortar FC Base - SDS11608 - 44Magesh MNo ratings yet
- Fatigue Stress in BoltsDocument26 pagesFatigue Stress in Boltsbiruk tolossaNo ratings yet
- G2C & B2C Services: Telecentre Entrepreneur CourseDocument6 pagesG2C & B2C Services: Telecentre Entrepreneur CourseKarthik VanamNo ratings yet
- Japanese Industrial StandardsDocument10 pagesJapanese Industrial StandardsKen SelorioNo ratings yet
- Carbohydrates Reaction - KLP 5Document23 pagesCarbohydrates Reaction - KLP 5Putri SalsabilaNo ratings yet
- 2007 06 08 OA FEA Kalaeloa Asphalt TerminalDocument255 pages2007 06 08 OA FEA Kalaeloa Asphalt TerminalEsteban Lopez ArboledaNo ratings yet
- Playground and Water Safety GuidelinesDocument50 pagesPlayground and Water Safety GuidelinesNgoc Nhu NguyenNo ratings yet
- Product Manual 3055Document5 pagesProduct Manual 3055North EastNo ratings yet
- Aboras MM 2015 Type of Failure in PFM RestorationDocument2 pagesAboras MM 2015 Type of Failure in PFM RestorationSopan SinamoNo ratings yet
- Product Risk Assessment Practices Regulatory AgenciesDocument19 pagesProduct Risk Assessment Practices Regulatory AgenciesAllyssa FernandezNo ratings yet
























































































Download as pdf or txt
You might also like
- ASTA Membership Directory 2022Document18 pagesASTA Membership Directory 2022Vasanthi Muthayan100% (1)
- Pediatric Potpourri 200+ New CPEN Questions: Certified Pediatric Emergency Nurse Review (3rd Edition Supplement)From EverandPediatric Potpourri 200+ New CPEN Questions: Certified Pediatric Emergency Nurse Review (3rd Edition Supplement)No ratings yet
- Actividad A4. Study CaseDocument2 pagesActividad A4. Study CaseDavid Padilla AcostaNo ratings yet
- Objectives CLUB FOOTDocument2 pagesObjectives CLUB FOOTAdriano SonnyNo ratings yet
- Club FootDocument3 pagesClub FootKim GalamgamNo ratings yet
- Club FootDocument5 pagesClub FootanisadestyaNo ratings yet
- Clubfoot: Lady Diane M. Cabriga Bsn-IiiDocument7 pagesClubfoot: Lady Diane M. Cabriga Bsn-IiiDayan CabrigaNo ratings yet
- Clubfoot: What Is A Clubfoot?Document1 pageClubfoot: What Is A Clubfoot?Joshua MccrayNo ratings yet
- Talipes Deformity or ClubfootDocument5 pagesTalipes Deformity or ClubfootcrisolandNo ratings yet
- ClubfootDocument5 pagesClubfootCherry AlmarezNo ratings yet
- Clubfoot ThesisDocument7 pagesClubfoot ThesisCollegePaperGhostWriterAkron100% (2)
- Scoliosis Surgery: Preparing For Surgery and A Hospital StayDocument9 pagesScoliosis Surgery: Preparing For Surgery and A Hospital StayFaris Aziz PridiantoNo ratings yet
- Physical Therapy in Corpus Christi For Pediatric Issues: Guide To Clubfoot MenuDocument17 pagesPhysical Therapy in Corpus Christi For Pediatric Issues: Guide To Clubfoot MenunovialbarNo ratings yet
- Symptoms: If Your Child Has Clubfoot, Here's What It Might Look LikeDocument112 pagesSymptoms: If Your Child Has Clubfoot, Here's What It Might Look LikeSantosh RudraNo ratings yet
- Physical Therapy in Corpus Christi For Pediatric Issues: Guide To Clubfoot MenuDocument17 pagesPhysical Therapy in Corpus Christi For Pediatric Issues: Guide To Clubfoot MenuHusna NadiaNo ratings yet
- ClubfootDocument22 pagesClubfootJhong Xyrus100% (3)
- ClubfootDocument12 pagesClubfootjoycesiosonNo ratings yet
- Adduction and Equinus.: Citation NeededDocument16 pagesAdduction and Equinus.: Citation NeededMaria Ardhail Dasalla RagodonNo ratings yet
- Developmental Dysplasia of The Hip, (DDH) Including Femoral and Pelvic OsteotomyDocument16 pagesDevelopmental Dysplasia of The Hip, (DDH) Including Femoral and Pelvic OsteotomyAkbar GazaliNo ratings yet
- Clubfoot - The Ponseti MethodDocument4 pagesClubfoot - The Ponseti MethodJerry Kurnia WahyudiNo ratings yet
- CLUBFOOTDocument19 pagesCLUBFOOTKaryn Joy LamisNo ratings yet
- ClubfootDocument27 pagesClubfootPrashanth K NairNo ratings yet
- Case StudyDocument11 pagesCase StudyAnj TadxNo ratings yet
- A. Skeletal System: Child Born With Physical/ Developmental ChallengeDocument10 pagesA. Skeletal System: Child Born With Physical/ Developmental ChallengeHazel NialaNo ratings yet
- Litrev ClubfootDocument6 pagesLitrev Clubfootdedyalkarni08No ratings yet
- CLUB FootDocument4 pagesCLUB FootDarwin Dux Lacson DimarucutNo ratings yet
- ClubfootDocument9 pagesClubfootLorebell100% (5)
- Slipped Upper Femoral Epiphysis: Child Health Information FactsheetDocument2 pagesSlipped Upper Femoral Epiphysis: Child Health Information FactsheetNurusshiami KhairatiNo ratings yet
- Help CfparentsDocument3 pagesHelp CfparentsjessgabNo ratings yet
- A Parents Guide To Treatment For Development Dysplasia of The HipDocument16 pagesA Parents Guide To Treatment For Development Dysplasia of The HipSunny Gabriels100% (1)
- Legg Perthes Disease What Is Legg-Perthes Disease?Document6 pagesLegg Perthes Disease What Is Legg-Perthes Disease?readerkellNo ratings yet
- Vincent Mosca - Clubfoot Guide For ParentsDocument3 pagesVincent Mosca - Clubfoot Guide For ParentsCatalin FloreaNo ratings yet
- ClubfootDocument27 pagesClubfootJaya Prabha100% (1)
- Club Foot: Ison, Kevin Christian B. BSN3D1Document27 pagesClub Foot: Ison, Kevin Christian B. BSN3D1Saputro AbdiNo ratings yet
- Diagnosing DDHDocument3 pagesDiagnosing DDHNylia AtibiNo ratings yet
- CONGENITAL TALIPES EQUINOVARUS in PMRDocument31 pagesCONGENITAL TALIPES EQUINOVARUS in PMRrachmadyNo ratings yet
- Congenital Hip DislocationDocument8 pagesCongenital Hip DislocationadrianojenfferNo ratings yet
- Developmental Dislocation (Dysplasia) of The Hip (DDH) : DescriptionDocument4 pagesDevelopmental Dislocation (Dysplasia) of The Hip (DDH) : DescriptiondfdnNo ratings yet
- Information For Patients Following Knee Arthroscopy: Therapies DirectorateDocument6 pagesInformation For Patients Following Knee Arthroscopy: Therapies Directoratepecson1No ratings yet
- Full Thickness Bowel Biopsy F1555 A4 BW FINAL Dec18Document2 pagesFull Thickness Bowel Biopsy F1555 A4 BW FINAL Dec18Nimra WaheedNo ratings yet
- HirschzxcxzcDocument2 pagesHirschzxcxzcZNEROLNo ratings yet
- Symptoms of Talipes DiseaseDocument6 pagesSymptoms of Talipes DiseaseJustine DumaguinNo ratings yet
- Eastern African International CollegeDocument5 pagesEastern African International CollegeDire DireNo ratings yet
- Beyond The Basics: Dr. Amna HaiderDocument29 pagesBeyond The Basics: Dr. Amna Haiderrabia khalidNo ratings yet
- Congenital-Torticollis (Wry Neck)Document57 pagesCongenital-Torticollis (Wry Neck)Shafiq Mohd NorNo ratings yet
- Splinting LeafletDocument2 pagesSplinting LeafletAbhishek GuptaNo ratings yet
- Scoliosis Surgery: Goals of The SurgeryDocument4 pagesScoliosis Surgery: Goals of The SurgeryFaris Aziz PridiantoNo ratings yet
- Developmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedDocument37 pagesDevelopmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedAh ZhangNo ratings yet
- CHD 1sDocument32 pagesCHD 1sLauNo ratings yet
- Perthes Disease - SurgeryDocument10 pagesPerthes Disease - SurgeryEla TINo ratings yet
- Congenital Talipes Equinovarus (Clubfoot)Document4 pagesCongenital Talipes Equinovarus (Clubfoot)Julliza Joy PandiNo ratings yet
- Club Foot: 1 Genetics 2 DiagnosisDocument8 pagesClub Foot: 1 Genetics 2 DiagnosispaulNo ratings yet
- Congenital Talipes EquinovarusDocument25 pagesCongenital Talipes EquinovarusArlyn MillanesNo ratings yet
- What Is Bladder Exstrophy?Document6 pagesWhat Is Bladder Exstrophy?preveennaNo ratings yet
- Rehab After OsteotomyDocument2 pagesRehab After OsteotomyMiguel OrdoñezNo ratings yet
- Knock Knees Genu Valgum: by DR - Abdullah AlmusallamDocument17 pagesKnock Knees Genu Valgum: by DR - Abdullah AlmusallamDrAbdullah AlmusallamNo ratings yet
- Clubfoot Written ReportDocument7 pagesClubfoot Written ReportAira Madel ArabaNo ratings yet
- Clubfoot - The Ponseti Method: Dale Elizabeth Jarka, MD, CM, FRCS (C)Document87 pagesClubfoot - The Ponseti Method: Dale Elizabeth Jarka, MD, CM, FRCS (C)muthia saniNo ratings yet
- Amp PedDocument118 pagesAmp PedElla ArusteiNo ratings yet
- Clubfoot Orthotic William Porter: Alexis Wickwire Erika Franzen Dr. Morey Moreland 02/08/2005Document11 pagesClubfoot Orthotic William Porter: Alexis Wickwire Erika Franzen Dr. Morey Moreland 02/08/2005Ay HaanNo ratings yet
- Club FootDocument11 pagesClub FootdrusmanjamilhcmdNo ratings yet
- If they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.From EverandIf they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.No ratings yet
- THE INDEPENDENT Issue 558Document44 pagesTHE INDEPENDENT Issue 558The Independent MagazineNo ratings yet
- The Role of EEG in The Diagnosis and Classification of The Epilepsy Syndromes (Part 1)Document66 pagesThe Role of EEG in The Diagnosis and Classification of The Epilepsy Syndromes (Part 1)Rosmery VillaNo ratings yet
- IS0125 F Fuel-ManagerDocument12 pagesIS0125 F Fuel-ManagerBilly12369No ratings yet
- Eq - 333Document1 pageEq - 333Franco SNo ratings yet
- Waste To Energy Potential in The Wastern Province of Saudi ArabiaDocument9 pagesWaste To Energy Potential in The Wastern Province of Saudi ArabiaahaaNo ratings yet
- Algorithm For The Management of A High Regional Block in ObstetricsDocument5 pagesAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNo ratings yet
- Final Exam QuestionsDocument4 pagesFinal Exam QuestionsAndil MaulanaNo ratings yet
- Comprehensive Report Card: About The Problems of Sub-Health TrendsDocument3 pagesComprehensive Report Card: About The Problems of Sub-Health TrendsFitriWidiastutiNo ratings yet
- Nepro Plastics Pvc4Document12 pagesNepro Plastics Pvc4chaouch.najehNo ratings yet
- Clinical Nutrition: Paediatric Nutrition Risk Scores in Clinical Practice: Children With Inflammatory Bowel DiseaseDocument4 pagesClinical Nutrition: Paediatric Nutrition Risk Scores in Clinical Practice: Children With Inflammatory Bowel DiseaseMaggie S HungNo ratings yet
- EcoDocument7 pagesEcoSushma YonzenNo ratings yet
- Laser Safety Test !Document5 pagesLaser Safety Test !shabeer hassimNo ratings yet
- COVID-19 and Disinfectants and Sanitizers in Food PremisesDocument5 pagesCOVID-19 and Disinfectants and Sanitizers in Food Premisesnur atiqah sobriNo ratings yet
- Transducer Engineering 2 Marks With AnswersDocument13 pagesTransducer Engineering 2 Marks With AnswersSridharan DNo ratings yet
- Construction and Installation of De-Icer BootsDocument11 pagesConstruction and Installation of De-Icer BootsPatrick dela rosaNo ratings yet
- Moving To A World Beyond P 0 05Document20 pagesMoving To A World Beyond P 0 05Frank LopezNo ratings yet
- Case Ih Tractor 1070 Operators Manual 9 2822Document22 pagesCase Ih Tractor 1070 Operators Manual 9 2822zacharygonzalez130703jse100% (140)
- The Microbiota in Cirrhosis and Its Role in Hepatic Decompensation. 2020Document15 pagesThe Microbiota in Cirrhosis and Its Role in Hepatic Decompensation. 2020mafe.z.solarte87No ratings yet
- Nitomortar FC Base - SDS11608 - 44Document13 pagesNitomortar FC Base - SDS11608 - 44Magesh MNo ratings yet
- Fatigue Stress in BoltsDocument26 pagesFatigue Stress in Boltsbiruk tolossaNo ratings yet
- G2C & B2C Services: Telecentre Entrepreneur CourseDocument6 pagesG2C & B2C Services: Telecentre Entrepreneur CourseKarthik VanamNo ratings yet
- Japanese Industrial StandardsDocument10 pagesJapanese Industrial StandardsKen SelorioNo ratings yet
- Carbohydrates Reaction - KLP 5Document23 pagesCarbohydrates Reaction - KLP 5Putri SalsabilaNo ratings yet
- 2007 06 08 OA FEA Kalaeloa Asphalt TerminalDocument255 pages2007 06 08 OA FEA Kalaeloa Asphalt TerminalEsteban Lopez ArboledaNo ratings yet
- Playground and Water Safety GuidelinesDocument50 pagesPlayground and Water Safety GuidelinesNgoc Nhu NguyenNo ratings yet
- Product Manual 3055Document5 pagesProduct Manual 3055North EastNo ratings yet
- Aboras MM 2015 Type of Failure in PFM RestorationDocument2 pagesAboras MM 2015 Type of Failure in PFM RestorationSopan SinamoNo ratings yet
- Product Risk Assessment Practices Regulatory AgenciesDocument19 pagesProduct Risk Assessment Practices Regulatory AgenciesAllyssa FernandezNo ratings yet