Download as docx, pdf, or txt
You might also like
- Pretest QuestionsDocument42 pagesPretest QuestionsSaras SinghNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Obagi Price ListDocument3 pagesObagi Price ListANDELYNNo ratings yet
- Pediatric Advanced Life Support: I. PALS System Approach AlgorithmDocument19 pagesPediatric Advanced Life Support: I. PALS System Approach AlgorithmIsabel Castillo100% (1)
- Haemodynamic Monitoring & Manipulation: an easy learning guideFrom EverandHaemodynamic Monitoring & Manipulation: an easy learning guideNo ratings yet
- 2017 05 GC Pocket CardDocument2 pages2017 05 GC Pocket Cardapi-312241089No ratings yet
- Poster1 Arrhythmia Recognition e PDFDocument1 pagePoster1 Arrhythmia Recognition e PDFSergio ChangNo ratings yet
- Icusheet - Anotherone 4Document1 pageIcusheet - Anotherone 4queenzkNo ratings yet
- DYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDocument3 pagesDYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDarell M. Book100% (1)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- IV PDFDocument63 pagesIV PDFelbagouryNo ratings yet
- Cardiac Study GuideDocument9 pagesCardiac Study GuideJane DiazNo ratings yet
- Cardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyDocument87 pagesCardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyummimalikihamidNo ratings yet
- ECG Master Class-2Document138 pagesECG Master Class-2Shohag ID Center100% (1)
- Brainsheet f04Document2 pagesBrainsheet f04mrsfelic08No ratings yet
- Nursing SheetDocument1 pageNursing Sheetseaturtles505100% (2)
- Lab Values - Chart by PriorityDocument2 pagesLab Values - Chart by PriorityashleyNo ratings yet
- Nursing Care of PlanDocument16 pagesNursing Care of PlanDbyNo ratings yet
- Arterial Lines in PACU: Presented by Autum Jacobs RN, BSNDocument34 pagesArterial Lines in PACU: Presented by Autum Jacobs RN, BSNinuko1212No ratings yet
- ACLS Class Packet PDFDocument9 pagesACLS Class Packet PDFImam GultomNo ratings yet
- Clinical KardexDocument2 pagesClinical KardexJackie Frey100% (2)
- Shock NotesDocument5 pagesShock NotesAlyss Wallschleger100% (1)
- Cardio MTB 2:3 Notes DONEDocument10 pagesCardio MTB 2:3 Notes DONESumatt KaurNo ratings yet
- ICU Rounding Template - v. WebsiteDocument2 pagesICU Rounding Template - v. Websitepattumkp0% (1)
- Rhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsDocument6 pagesRhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsJohnildy MatiasNo ratings yet
- Coumadin Dosing GuideDocument3 pagesCoumadin Dosing Guidemorale28No ratings yet
- Nurse Report SheetDocument1 pageNurse Report SheetTassos KolliasNo ratings yet
- Dysrhythmia TestsDocument3 pagesDysrhythmia TestsKimberly WhitesideNo ratings yet
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani Kayed100% (1)
- Fluid and Electrolyte Balance in ICUDocument46 pagesFluid and Electrolyte Balance in ICUtapas_kbNo ratings yet
- GI Skin GI Skin: Last BM Last BMDocument2 pagesGI Skin GI Skin: Last BM Last BMlmaoheartsNo ratings yet
- EKG Quick Reference ChartDocument4 pagesEKG Quick Reference ChartMildaNo ratings yet
- EKG - Assignment Without AnswersDocument10 pagesEKG - Assignment Without AnswersJon Millhollon100% (1)
- ECG Rythum Study Guide PDFDocument9 pagesECG Rythum Study Guide PDFArtika MayandaNo ratings yet
- LS Identifying ArrhythmiasDocument5 pagesLS Identifying ArrhythmiasClaudia Park100% (1)
- Ecg Reading NotesDocument17 pagesEcg Reading NotesMarian FloresNo ratings yet
- Cardiac Dysrhythmia Final Study GuideDocument14 pagesCardiac Dysrhythmia Final Study GuideBSNNursing101100% (2)
- Aha Guidelines StemiDocument94 pagesAha Guidelines StemiDika DekokNo ratings yet
- Introduction To ECG RhythmsDocument59 pagesIntroduction To ECG RhythmsIvona RagužNo ratings yet
- Cardiac MedicationsDocument8 pagesCardiac Medicationsangeline totaram100% (2)
- All ConditionsDocument6 pagesAll ConditionsJoya Ruben CamposNo ratings yet
- ICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHDocument32 pagesICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHNicole Adkins100% (1)
- Lab Values and Vital SignsDocument4 pagesLab Values and Vital SignsWole Olaluwoye100% (1)
- ICU Report SheetDocument1 pageICU Report SheetjejadayoNo ratings yet
- Patient Sticker Patient Sticker: AM LabsDocument3 pagesPatient Sticker Patient Sticker: AM LabsNurse BettyNo ratings yet
- Hemodynamic Drug InfusionsDocument45 pagesHemodynamic Drug InfusionsDawit MucheNo ratings yet
- Blood Gas InterpretationDocument36 pagesBlood Gas InterpretationMary Charmaine DivinagraciaNo ratings yet
- Example of Completed Form: Admit Dx/Chief Complaint/Hx Current ILLNESS: - Bowel Obstruction RespiratoryDocument3 pagesExample of Completed Form: Admit Dx/Chief Complaint/Hx Current ILLNESS: - Bowel Obstruction RespiratoryJosephNo ratings yet
- ICE DrugsDocument2 pagesICE DrugsRichelle FrondaNo ratings yet
- Nervous System AlterationsDocument45 pagesNervous System AlterationsMajesty ParkerNo ratings yet
- Dysrhythmia Instructor 2018 2 PDFDocument105 pagesDysrhythmia Instructor 2018 2 PDFtvrossyNo ratings yet
- Icu Nursing BrainDocument2 pagesIcu Nursing Brainapi-282417591100% (2)
- Cardio - ECGDocument13 pagesCardio - ECGSheryl Layne Lao-SebrioNo ratings yet
- This Study Resource WasDocument2 pagesThis Study Resource WasKimberly WhitesideNo ratings yet
- How To Read An ECGDocument21 pagesHow To Read An ECGSlychenkoNo ratings yet
- Hemodynamic Values PDFDocument1 pageHemodynamic Values PDFAudrey DelfinNo ratings yet
- The Ultimate Review For MedicalDocument15 pagesThe Ultimate Review For MedicalJap Avila BernasNo ratings yet
- Emergency Nurse Protocol Back PainDocument2 pagesEmergency Nurse Protocol Back PainSimon S. KledenNo ratings yet
- New Icu SheetDocument3 pagesNew Icu SheetJan MarcusNo ratings yet
- A Nurse's Guide to Caring for Cardiac Intervention PatientsFrom EverandA Nurse's Guide to Caring for Cardiac Intervention PatientsNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Yale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1Document12 pagesYale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1omegasauron0gmailcomNo ratings yet
- Remediating The Struggling ResidentDocument52 pagesRemediating The Struggling Residentomegasauron0gmailcomNo ratings yet
- Welcome To UNC Hematology/Oncology!Document80 pagesWelcome To UNC Hematology/Oncology!omegasauron0gmailcomNo ratings yet
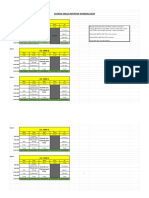
- CSI Schedule 2019-2020Document2 pagesCSI Schedule 2019-2020omegasauron0gmailcomNo ratings yet
- Mary Clare Higgins-Chen, MD, MPH Donna Windish, MD, MPH: Alopecia Week 25Document9 pagesMary Clare Higgins-Chen, MD, MPH Donna Windish, MD, MPH: Alopecia Week 25omegasauron0gmailcomNo ratings yet
- EBM Therapy and Diagnosis-Interpretation of Results ExerciseDocument3 pagesEBM Therapy and Diagnosis-Interpretation of Results Exerciseomegasauron0gmailcomNo ratings yet
- EBM Video TutorialsDocument1 pageEBM Video Tutorialsomegasauron0gmailcomNo ratings yet
- Allergy H&PDocument3 pagesAllergy H&Pomegasauron0gmailcomNo ratings yet
- AM Curriculum Review-2019-2020Document3 pagesAM Curriculum Review-2019-2020omegasauron0gmailcomNo ratings yet
- Therapy Article questions-ALLHATDocument2 pagesTherapy Article questions-ALLHATomegasauron0gmailcomNo ratings yet
- Supplemental Guide For Allergy and ImmunologyDocument52 pagesSupplemental Guide For Allergy and Immunologyomegasauron0gmailcomNo ratings yet
- Breast Cancer Screening ResDocument7 pagesBreast Cancer Screening Resomegasauron0gmailcomNo ratings yet
- BU Reaction Paper ChavezDocument2 pagesBU Reaction Paper ChavezShrwn JcNo ratings yet
- 841xx-Red Msds Na enDocument17 pages841xx-Red Msds Na enFarbod Jz.No ratings yet
- SerratiaDocument26 pagesSerratiaduverney.gaviriaNo ratings yet
- أسئلة الهيئة السعودية للتخصصات الطبية لاخاصئيي الكيمياء الحيوية 2015 الجزء الثانيDocument13 pagesأسئلة الهيئة السعودية للتخصصات الطبية لاخاصئيي الكيمياء الحيوية 2015 الجزء الثانيMohsen HaleemNo ratings yet
- Written Work 6 Career ProfileDocument4 pagesWritten Work 6 Career ProfileSean Benedict G. BalalaNo ratings yet
- Geopathic Stress: Causes & Symptoms Solutions & Costs Facts Testimonials ChoicesDocument28 pagesGeopathic Stress: Causes & Symptoms Solutions & Costs Facts Testimonials ChoicesgururajNo ratings yet
- Bionic Eye - An Artificial Vision & Comparative Study Based On Different Implant TechniquesDocument9 pagesBionic Eye - An Artificial Vision & Comparative Study Based On Different Implant TechniquesGabi BermudezNo ratings yet
- Davis v. LizzoDocument44 pagesDavis v. LizzoTHR100% (1)
- Junior 100m BDocument5 pagesJunior 100m BsjktkbbmNo ratings yet
- Evolution of Pollutants Emissionin Relation Toroad Traffic in The City of Lome (Togo) From 2010 To 2019Document7 pagesEvolution of Pollutants Emissionin Relation Toroad Traffic in The City of Lome (Togo) From 2010 To 2019IJAR JOURNALNo ratings yet
- da Silva 等 - 2023 - Comparison between clear aligners and 2 × 4 mechanDocument8 pagesda Silva 等 - 2023 - Comparison between clear aligners and 2 × 4 mechanDr.QiuNo ratings yet
- MusicStudies PDFDocument2 pagesMusicStudies PDFRosie VegaNo ratings yet
- Data Usulan R.S Ngawi 24Document26 pagesData Usulan R.S Ngawi 24medina madinahNo ratings yet
- Midwives and Nutrition During Preganncy - Contoh Literatuyr ReviewDocument7 pagesMidwives and Nutrition During Preganncy - Contoh Literatuyr ReviewNansa PuspaNo ratings yet
- Importance of Happiness at WorkplaceDocument1 pageImportance of Happiness at WorkplaceAparna Singh Res. Scholar, Humanistic Studies, IIT(BHU)No ratings yet
- Executive Summary: Corvallis School District COVID-19 Vaccine RequirementDocument17 pagesExecutive Summary: Corvallis School District COVID-19 Vaccine RequirementSinclair Broadcast Group - EugeneNo ratings yet
- Bloody MaryDocument2 pagesBloody MaryManolache AnaNo ratings yet
- Types of Cloud - 60589042Document1 pageTypes of Cloud - 60589042Violet ChertokNo ratings yet
- Learning and Teaching in The Clinical EnvironmentDocument4 pagesLearning and Teaching in The Clinical EnvironmentDaniel Alejandro Lozano MorenoNo ratings yet
- Analytical Exposition Text 2Document3 pagesAnalytical Exposition Text 2lnanurulizzatiNo ratings yet
- Creolin Eco MSDSDocument9 pagesCreolin Eco MSDSMusa SabujNo ratings yet
- Direct Anterior Composites: A Practical Guide: RestorativeDocument15 pagesDirect Anterior Composites: A Practical Guide: Restorativesuseth100% (1)
- The Five Basic Interactional PhenomenaDocument2 pagesThe Five Basic Interactional PhenomenaMa. Esperanza C. Eijansantos-Reavon0% (1)
- Medical ConventionalDocument6 pagesMedical ConventionalshamsulNo ratings yet
- IFU Dia TT EN 20170915Document2 pagesIFU Dia TT EN 20170915P managerNo ratings yet
- Aip Budget 2024 Needed DataDocument22 pagesAip Budget 2024 Needed Datamoox TVNo ratings yet
- Class 5 Subject Science Chapter 3 Health and DiseasesDocument3 pagesClass 5 Subject Science Chapter 3 Health and DiseasesVimal AnandNo ratings yet
- 8204 HardnessDocument8 pages8204 Hardnessedi_munawarNo ratings yet