Download as pdf or txt
You might also like
- Employment Verification LetterDocument3 pagesEmployment Verification LetterByron Bo' Jones100% (1)
- G3 - Cut Hair Using Basic Barbering Techniques PDFDocument10 pagesG3 - Cut Hair Using Basic Barbering Techniques PDFKetan Patel100% (2)
- Physiotherapy in Alopecia AreataDocument21 pagesPhysiotherapy in Alopecia AreataAngel100% (2)
- Alopecia Areata PresentationDocument12 pagesAlopecia Areata Presentationpcjoy2100% (1)
- Alopecia 160716052003Document26 pagesAlopecia 160716052003AbirajanNo ratings yet
- ALOPECIADocument90 pagesALOPECIAluckyswiss7776848No ratings yet
- Assessment of Hair and Scalp Disorders: Antonella Tosti and John GrayDocument5 pagesAssessment of Hair and Scalp Disorders: Antonella Tosti and John GrayDavid51No ratings yet
- Article 0011 44 50Document7 pagesArticle 0011 44 50apj abdulNo ratings yet
- Hair Problems 1Document4 pagesHair Problems 1مصطفى عبد الرزاق ورد حسينNo ratings yet
- Male Pattern Androgenetic AlopeciaDocument6 pagesMale Pattern Androgenetic AlopeciaYasser Yousif Al-ahmadyNo ratings yet
- Disorders of HairDocument5 pagesDisorders of Hairعبدالعزيز احمد علي عتشNo ratings yet
- Hair Loss Common Causes and TreatmentDocument8 pagesHair Loss Common Causes and TreatmentDesireé González ArzolayNo ratings yet
- Hair Disorders and Pigmented Disorders of The SkinDocument8 pagesHair Disorders and Pigmented Disorders of The SkinJim Jose AntonyNo ratings yet
- 2.hair DisordersDocument50 pages2.hair DisordersAzeem Majid100% (4)
- Hair DisordersDocument38 pagesHair DisordersMoayad NawaflehNo ratings yet
- 8 - Hair Disorders (Updated)Document14 pages8 - Hair Disorders (Updated)haytham aliNo ratings yet
- Hair and Nail DisordersDocument58 pagesHair and Nail DisordersHrishikesh NachinolkarNo ratings yet
- Hair Disorders: Biology of Hair GrowthDocument4 pagesHair Disorders: Biology of Hair GrowthCoral Srinivasa RamaluNo ratings yet
- 361 FullDocument7 pages361 FullFikri CarVlogNo ratings yet
- Whiting 2001Document6 pagesWhiting 2001Nur ElidaNo ratings yet
- 12 Harish K-Rajesh R-Yasar-Arafath A-Ramzan-Beevi MDocument15 pages12 Harish K-Rajesh R-Yasar-Arafath A-Ramzan-Beevi MMichaelNo ratings yet
- Androgenetic Alopecia: January 2015Document14 pagesAndrogenetic Alopecia: January 2015MFajri irfanNo ratings yet
- Androgenetic AlopeciaDocument22 pagesAndrogenetic AlopeciaYuliannisa Nyunyun100% (1)
- Hair Diseases: AnatomyDocument36 pagesHair Diseases: AnatomyMasithaNo ratings yet
- Dr. Dixit-MS 2nd ProofDocument22 pagesDr. Dixit-MS 2nd ProofGaneshKumarNo ratings yet
- Minerva Medica: Hair Loss in WomenDocument8 pagesMinerva Medica: Hair Loss in WomenMd Kamruzzaman KhanNo ratings yet
- 2024.derma#13. Hair DisordersDocument7 pages2024.derma#13. Hair DisordersB34-YvesJethro ReyesNo ratings yet
- Female Pattern Hair Loss Current TreatmentDocument13 pagesFemale Pattern Hair Loss Current Treatmentdiessica alvesNo ratings yet
- Hair 1Document26 pagesHair 1Abdelmouez AnwerNo ratings yet
- Alopecia PDFDocument36 pagesAlopecia PDFFelp ScholzNo ratings yet
- Estudio XL HAIR - Alopecia AreataDocument32 pagesEstudio XL HAIR - Alopecia AreataIrina KucevichuteNo ratings yet
- Alopecia HandoutDocument4 pagesAlopecia HandoutEmAlNourNo ratings yet
- Alopecia: Mrs. Neeraja Rajiv Asst Professor Cardio-RespDocument52 pagesAlopecia: Mrs. Neeraja Rajiv Asst Professor Cardio-RespNEERAJA O S O S100% (1)
- Hair4u MedDocument87 pagesHair4u MedkurutalaNo ratings yet
- Case of The Week - Hair LossDocument3 pagesCase of The Week - Hair LossMoet Moet KhineNo ratings yet
- 15 Female Pattern Alopecia and Telogen Effluvium, Figuring Out Diffuse AlopeciaDocument5 pages15 Female Pattern Alopecia and Telogen Effluvium, Figuring Out Diffuse AlopeciaGi D'AtriNo ratings yet
- Baldness: Androgenetic AlopeciaDocument3 pagesBaldness: Androgenetic Alopeciasanjay6969No ratings yet
- HairDocument38 pagesHairNithin NairNo ratings yet
- Steroidify Hair Loss GuideDocument13 pagesSteroidify Hair Loss GuidefizzNo ratings yet
- Hair Restoration Update: by DR - Tarek Ahmed Said Lecturer of Plastic Surgery, Cairo UniversityDocument27 pagesHair Restoration Update: by DR - Tarek Ahmed Said Lecturer of Plastic Surgery, Cairo UniversityHamid Reza TeymouriNo ratings yet
- AlopeciaDocument12 pagesAlopeciasonamNo ratings yet
- Systematic Approach To Hair Loss in Women: Ralph M. TrüebDocument15 pagesSystematic Approach To Hair Loss in Women: Ralph M. TrüebErika Alvarez IbarraNo ratings yet
- Common Hair Loss Disorders: Caring For Common Skin ConditionsDocument10 pagesCommon Hair Loss Disorders: Caring For Common Skin ConditionsDita N HapsariNo ratings yet
- AlopeciaDocument11 pagesAlopeciaAnonymous kltUTa100% (1)
- Male and Female Pattern Hair LossDocument15 pagesMale and Female Pattern Hair LossRahul SrivastavaNo ratings yet
- Microsoft PowerPoint - Hair N Nail - PPT (Compatibility Mode)Document4 pagesMicrosoft PowerPoint - Hair N Nail - PPT (Compatibility Mode)kamalab04No ratings yet
- HairMD Hair TreatmentDocument16 pagesHairMD Hair TreatmentrgfghgNo ratings yet
- Boards' Fodder: AlopeciaDocument2 pagesBoards' Fodder: AlopeciaIuliana NitaNo ratings yet
- 88 Hair Growth DisordrDocument24 pages88 Hair Growth DisordrAlivia Soeraya100% (1)
- Materi - AlopeciaDocument27 pagesMateri - Alopecia6130015013 MOCHAMMAD SULUNG NOVIYANTO SKMNo ratings yet
- Disorder of The HairDocument62 pagesDisorder of The HairzakiNo ratings yet
- Hair Loss (About, Types and Treatment) WhatsMedi ResearchDocument5 pagesHair Loss (About, Types and Treatment) WhatsMedi ResearchSiddharth Choudhery100% (1)
- Understanding AlopeciaDocument4 pagesUnderstanding Alopeciafarishahanis07No ratings yet
- Hair Fall Case DiscussionDocument18 pagesHair Fall Case DiscussionJo CanensNo ratings yet
- Female Pattern Baldness - Diagnosis and TreatmentsDocument3 pagesFemale Pattern Baldness - Diagnosis and TreatmentsKadeer AlamNo ratings yet
- Bio ProjectDocument12 pagesBio Projectshadabdel007No ratings yet
- Alopecia 160716052003Document27 pagesAlopecia 160716052003k. bNo ratings yet
- Physical Means of Treating Unwanted Hair: R W & T S. ADocument10 pagesPhysical Means of Treating Unwanted Hair: R W & T S. Adipika awindaNo ratings yet
- Homeopathic Treatment For Hair Loss PDFDocument6 pagesHomeopathic Treatment For Hair Loss PDFMd Kamruzzaman KhanNo ratings yet
- Lesser Known Homoeopathic Medicines of Alopecia Areata.20200718115446Document9 pagesLesser Known Homoeopathic Medicines of Alopecia Areata.20200718115446BruntNo ratings yet
- Disorders of Hair FollicleDocument41 pagesDisorders of Hair Folliclerejuven100% (3)
- Hair Loss In Women: The Ultimate Hair Loss Book For Every WomanFrom EverandHair Loss In Women: The Ultimate Hair Loss Book For Every WomanNo ratings yet
- Yale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1Document12 pagesYale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1omegasauron0gmailcomNo ratings yet
- Remediating The Struggling ResidentDocument52 pagesRemediating The Struggling Residentomegasauron0gmailcomNo ratings yet
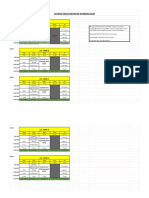
- CSI Schedule 2019-2020Document2 pagesCSI Schedule 2019-2020omegasauron0gmailcomNo ratings yet
- Allergy H&PDocument3 pagesAllergy H&Pomegasauron0gmailcomNo ratings yet
- Welcome To UNC Hematology/Oncology!Document80 pagesWelcome To UNC Hematology/Oncology!omegasauron0gmailcomNo ratings yet
- Ccu Survival GuideDocument10 pagesCcu Survival Guideomegasauron0gmailcom100% (1)
- EBM Therapy and Diagnosis-Interpretation of Results ExerciseDocument3 pagesEBM Therapy and Diagnosis-Interpretation of Results Exerciseomegasauron0gmailcomNo ratings yet
- AM Curriculum Review-2019-2020Document3 pagesAM Curriculum Review-2019-2020omegasauron0gmailcomNo ratings yet
- EBM Video TutorialsDocument1 pageEBM Video Tutorialsomegasauron0gmailcomNo ratings yet
- Supplemental Guide For Allergy and ImmunologyDocument52 pagesSupplemental Guide For Allergy and Immunologyomegasauron0gmailcomNo ratings yet
- Therapy Article questions-ALLHATDocument2 pagesTherapy Article questions-ALLHATomegasauron0gmailcomNo ratings yet
- Breast Cancer Screening ResDocument7 pagesBreast Cancer Screening Resomegasauron0gmailcomNo ratings yet
- Disponibil in Pagina Cod DenumireDocument3 pagesDisponibil in Pagina Cod DenumireSoryna IuliaNo ratings yet
- English 3 - Unit 11Document47 pagesEnglish 3 - Unit 11olga romeroNo ratings yet
- Tricology WordDocument26 pagesTricology WordDrushti KadamNo ratings yet
- Uniform AgreementDocument1 pageUniform Agreementvice gonzalezNo ratings yet
- 3 - Forensics 02 03 Botka Hair AnalysisDocument23 pages3 - Forensics 02 03 Botka Hair AnalysisFajar FebriantoNo ratings yet
- Charcoal Shampoo and ConditionerDocument7 pagesCharcoal Shampoo and ConditionerDIGITAL natureskarmaNo ratings yet
- PDFDocument2 pagesPDFIts Roudy100% (1)
- Evolution of Sun SilkDocument43 pagesEvolution of Sun Silkjonty31No ratings yet
- Zipper TechniqueDocument1 pageZipper TechniqueLeo CabelosNo ratings yet
- Describing PeopleDocument4 pagesDescribing PeopleMilena Rozo100% (1)
- TLE 9 10 Hairdressing 2 Q1 - M1 For Printing PDFDocument30 pagesTLE 9 10 Hairdressing 2 Q1 - M1 For Printing PDFJANE ABAPONo ratings yet
- Appearance Pictionary and ExcercisesDocument4 pagesAppearance Pictionary and ExcercisesJuan PleiadesNo ratings yet
- Perming: Reported By: Nahida H. AliDocument24 pagesPerming: Reported By: Nahida H. AliNahidaHali100% (2)
- Rangkuman Materi Bahasa Inggris Kelas 3 SDDocument2 pagesRangkuman Materi Bahasa Inggris Kelas 3 SDDian SaragihNo ratings yet
- Different Type of WigsDocument3 pagesDifferent Type of WigsArfaxed SaddiqueNo ratings yet
- S Wild-and-Wacky-WigsDocument9 pagesS Wild-and-Wacky-WigsNatalia IlhanNo ratings yet
- PricelistDocument11 pagesPricelistRike Dwi SantariiNo ratings yet
- Dadhi Aur Munch Ke Safed Baalo Ka Upchar 7 Gharelu NuskheDocument3 pagesDadhi Aur Munch Ke Safed Baalo Ka Upchar 7 Gharelu NuskheGovindNo ratings yet
- There Are Many Ways To Describe People Through Their Physical Appearances. The Following Are Some General Appearances of SomeoneDocument8 pagesThere Are Many Ways To Describe People Through Their Physical Appearances. The Following Are Some General Appearances of SomeoneEndah TeWe UddhiharyaNo ratings yet
- Describing People Greyscale Key Picture Description Exercises 14721Document3 pagesDescribing People Greyscale Key Picture Description Exercises 14721Gulderay IklassovaNo ratings yet
- Session 2 - The Verb 'Be' and Adjectives of Physical Description & PersonalityDocument19 pagesSession 2 - The Verb 'Be' and Adjectives of Physical Description & PersonalityParth MuniNo ratings yet
- Importance of Hair TransplantDocument8 pagesImportance of Hair TransplantKaayakalp ClinicNo ratings yet
- Match The Words and The Pictures.: Find Ten Describing Words in The Word SearchDocument2 pagesMatch The Words and The Pictures.: Find Ten Describing Words in The Word SearchСупер Вумэн0% (1)
- Price List BarkberDocument2 pagesPrice List BarkberCristieNo ratings yet
- 11 Tips For Amazing Male Curly HairDocument3 pages11 Tips For Amazing Male Curly HairWALEED HASSANNo ratings yet
- Soft SkillDocument15 pagesSoft SkillJeffery YipNo ratings yet
- Allure Hair Products Private LimitedDocument25 pagesAllure Hair Products Private LimitedAUDIO CLIPS BLOGNo ratings yet
- Afro-Textured Hair - WikipediaDocument98 pagesAfro-Textured Hair - Wikipediaخالد مدغشقرNo ratings yet