Download as pdf or txt
You might also like
- POLYGRAPHYDocument12 pagesPOLYGRAPHYKhimber Claire Lala MaduyoNo ratings yet
- Family Medicine Study GuideDocument240 pagesFamily Medicine Study GuideJeremy Christmann100% (1)
- Small Bowel Obstruction Concept Map-NursingDocument1 pageSmall Bowel Obstruction Concept Map-NursingTessa Claire JaranowskiNo ratings yet
- 05 IV Induction Agents PDFDocument0 pages05 IV Induction Agents PDFjuniorebinda100% (1)
- Organophospha Te (Op) Poisining: Presented byDocument44 pagesOrganophospha Te (Op) Poisining: Presented byShantanu Kr VatsyayanNo ratings yet
- Current Management Guidline in Organophosphors Poisoning: DR - Surendra Khosya Guided by Dr. S.R Meena Dr. Meenaxi ShardaDocument28 pagesCurrent Management Guidline in Organophosphors Poisoning: DR - Surendra Khosya Guided by Dr. S.R Meena Dr. Meenaxi ShardasurendrakhosyaNo ratings yet
- Organophosphate PoisoningDocument23 pagesOrganophosphate PoisoningUsman Ali AkbarNo ratings yet
- IAP PICU (1) - CompressedDocument3 pagesIAP PICU (1) - CompressedDr Divyarani D CNo ratings yet
- Iap PicuDocument3 pagesIap PicuDr Divyarani D CNo ratings yet
- Organophosphorus Poisoning PDFDocument5 pagesOrganophosphorus Poisoning PDFEliuth Zamora100% (1)
- Lo Week 5 TropmedDocument21 pagesLo Week 5 TropmedAnne MeilynNo ratings yet
- Lo Week 5 TropmedDocument25 pagesLo Week 5 TropmedDapot SianiparNo ratings yet
- Organophosphrous PoisoningDocument53 pagesOrganophosphrous Poisoningpriyashu78100% (1)
- 36-Organophosphorus PoisoningDocument28 pages36-Organophosphorus PoisoningSumaiyyaNo ratings yet
- Cholinergic SyndromeDocument3 pagesCholinergic SyndromeEmman AguilarNo ratings yet
- Op Compound Poisoning Guidelines AapDocument6 pagesOp Compound Poisoning Guidelines AapchtbhtNo ratings yet
- Op PoisoningDocument6 pagesOp PoisoningSid DhayriNo ratings yet
- Management Guidelines of Common PoisioningDocument52 pagesManagement Guidelines of Common PoisioningshravaniNo ratings yet
- Organophosphate Poisoning 2Document12 pagesOrganophosphate Poisoning 2Diana MurguiaNo ratings yet
- AnticholinergicDocument44 pagesAnticholinergicLucas JelmarNo ratings yet
- Poisoning: Clinical Biochemistry: Metabolic and Clinical Aspects (Third Edition)Document2 pagesPoisoning: Clinical Biochemistry: Metabolic and Clinical Aspects (Third Edition)lia lykimNo ratings yet
- Organophosphate POISONING 1 (1)Document12 pagesOrganophosphate POISONING 1 (1)Sudip PoudelNo ratings yet
- Organophosphate Poisoning (Reference Material For OSCE)Document29 pagesOrganophosphate Poisoning (Reference Material For OSCE)hovico3936No ratings yet
- OP PoisoningDocument14 pagesOP PoisoningAnmol KudalNo ratings yet
- OrganophosphateDocument21 pagesOrganophosphatehendra_darmawan_4No ratings yet
- Autonomic Nervous System-2Document8 pagesAutonomic Nervous System-2محمد علي حميدNo ratings yet
- Opc PoisoningDocument57 pagesOpc PoisoningJanthonyNo ratings yet
- Indirect Acting Cholinomimetics - BSNDocument33 pagesIndirect Acting Cholinomimetics - BSNKAMAU FRANCIS GATHUTHINo ratings yet
- 1 Anticholinergic DrugsDocument24 pages1 Anticholinergic DrugskiranNo ratings yet
- Pesticide and Herbicide Poisoning (Editedv2)Document58 pagesPesticide and Herbicide Poisoning (Editedv2)Alex MatthewNo ratings yet
- ANS & Cholinergic DrugsDocument62 pagesANS & Cholinergic DrugsSunanda mohanNo ratings yet
- Neurohumoral Transmission, Parasympatholytics, PS MimeticsDocument51 pagesNeurohumoral Transmission, Parasympatholytics, PS MimeticsrajeswariNo ratings yet
- Toxicology of Newer Insecticides in Small Animals - Wismer and Means 2012Document13 pagesToxicology of Newer Insecticides in Small Animals - Wismer and Means 2012Camyla NunesNo ratings yet
- 7 - PesticidesDocument10 pages7 - Pesticidesghada.k.elsamanNo ratings yet
- 7 OrganophsphorusDocument11 pages7 OrganophsphorusHeba AlhasiNo ratings yet
- Cholinergic and AnticholinergicDocument77 pagesCholinergic and Anticholinergicsweta sumanNo ratings yet
- AtropineDocument13 pagesAtropineMostafa HassanNo ratings yet
- Organophosphate and Carbamate PoisoningDocument9 pagesOrganophosphate and Carbamate PoisoningoscarcheongyjNo ratings yet
- Met Hamido PhosDocument2 pagesMet Hamido PhosesposibleNo ratings yet
- Jawt 11 I 1 P 1Document6 pagesJawt 11 I 1 P 1Jesicca SNo ratings yet
- IV Anesthetic AgentsDocument72 pagesIV Anesthetic AgentsRaghavendra PrasadNo ratings yet
- Organophosphate Poisoning GuidelineDocument5 pagesOrganophosphate Poisoning Guidelinelamoleverde9297No ratings yet
- Organophosphate Insecticides (OPC)Document27 pagesOrganophosphate Insecticides (OPC)ahmed.farag.ali2020No ratings yet
- ManagementofOPpoisoning JNHRCDocument9 pagesManagementofOPpoisoning JNHRCfakhrina nur fadhillahNo ratings yet
- Interest of Early Toxicological Sampling During Alpha Chloralose in Toxication, A Case ReportDocument4 pagesInterest of Early Toxicological Sampling During Alpha Chloralose in Toxication, A Case ReportIJAR JOURNALNo ratings yet
- O P Poisoning AnithaDocument56 pagesO P Poisoning AnithaAnitha NoronhaNo ratings yet
- Cholinergic drugs-BPTDocument39 pagesCholinergic drugs-BPTHUZAIFA YAMAANNo ratings yet
- Drug StudyDocument6 pagesDrug StudyMarielle Denise Tagtag BugtongNo ratings yet
- Organophosphorus PoisoningDocument6 pagesOrganophosphorus PoisoningNishaAhsin0% (1)
- Organophosphate and Carbamate PoisoningDocument13 pagesOrganophosphate and Carbamate PoisoningAntonella Angulo CruzadoNo ratings yet
- Cho Liner GicDocument34 pagesCho Liner GicIt's your ChannelNo ratings yet
- Organophosphate PoisoningDocument22 pagesOrganophosphate Poisoningatiyasimon2020No ratings yet
- Two Toxicologic Emergencies: Case Studies inDocument4 pagesTwo Toxicologic Emergencies: Case Studies insiddharsclubNo ratings yet
- Lecture 7Document26 pagesLecture 7Maya KawwaNo ratings yet
- Organophosphorus Insecticides and Nerve Gas Agents PoisoningDocument42 pagesOrganophosphorus Insecticides and Nerve Gas Agents PoisoningBhavanadhar PentaNo ratings yet
- Organophosphorus Toxicity - Show NotesDocument4 pagesOrganophosphorus Toxicity - Show NotesLakshay ChananaNo ratings yet
- Clinical Toxicology 2Document121 pagesClinical Toxicology 2sireenmahyobNo ratings yet
- A Case Report and Overview of Organophosphate (OP) PoisoningDocument5 pagesA Case Report and Overview of Organophosphate (OP) PoisoningDhruva PatelNo ratings yet
- SpeakingDocument6 pagesSpeakingLinh MaiNo ratings yet
- 1013 Vasoactive Agents in ShockDocument20 pages1013 Vasoactive Agents in Shockrogelio cruzNo ratings yet
- WS 11.1 The Gas Exchange SystemDocument3 pagesWS 11.1 The Gas Exchange SystemClaribelNo ratings yet
- Putrefaction and Livor MortisDocument19 pagesPutrefaction and Livor MortisKU RU RUNo ratings yet
- Extubation OR Decannulation (Assist)Document5 pagesExtubation OR Decannulation (Assist)ydtrgn100% (1)
- Cardiovascular System WORKS SHEET GRANETADocument9 pagesCardiovascular System WORKS SHEET GRANETAFrederick Matthew MendozaNo ratings yet
- Tepid SpongingDocument3 pagesTepid SpongingNrs Sani Sule MashiNo ratings yet
- Fluid Therapy For Critically Ill Dogs and Cats - WSAVA2005 - VINDocument14 pagesFluid Therapy For Critically Ill Dogs and Cats - WSAVA2005 - VINHament KumarNo ratings yet
- Quiz 003 - Attempt ReviewDocument2 pagesQuiz 003 - Attempt ReviewGian Peñaflor67% (3)
- 2023 - A Patient's Guide To Obstructive Sleep Apnea Syndrome (Arnav Shetty, Peter M Baptista Jardín)Document81 pages2023 - A Patient's Guide To Obstructive Sleep Apnea Syndrome (Arnav Shetty, Peter M Baptista Jardín)César EscobarNo ratings yet
- The Value of Vocal Warm-Up and Cool-Down Exercises: Questions and ControversiesDocument3 pagesThe Value of Vocal Warm-Up and Cool-Down Exercises: Questions and ControversiesTayssa MarquesNo ratings yet
- 2006 Lange OutlineDocument570 pages2006 Lange Outlinemequanint kefieNo ratings yet
- Nursing Responsibilities For Oxygen AdministrationDocument3 pagesNursing Responsibilities For Oxygen AdministrationJahseh WolfeNo ratings yet
- AutacoidsDocument21 pagesAutacoidsMuhammad Shahid BilalNo ratings yet
- Sepsis and SirsDocument14 pagesSepsis and SirsRuki HartawanNo ratings yet
- Dehydration Secondary To Diarrhea - NPDDocument3 pagesDehydration Secondary To Diarrhea - NPDLovely Grace PoreNo ratings yet
- 3.1 Homeostasis in Living ThingsDocument4 pages3.1 Homeostasis in Living ThingsJie TungNo ratings yet
- Laporan Jaga IGDDocument4 pagesLaporan Jaga IGDamal.fathullahNo ratings yet
- 1st Quarter PE Pre TestDocument2 pages1st Quarter PE Pre TestMaryJane SantiagoNo ratings yet
- Quarter: 4 / Semester: 2 / WEEK: 4: Online Resource/sDocument17 pagesQuarter: 4 / Semester: 2 / WEEK: 4: Online Resource/sTristan Paul PagalananNo ratings yet
- Nursing CS Blood-Transfusion-ChecklistDocument1 pageNursing CS Blood-Transfusion-ChecklistJanaNo ratings yet
- CABGDocument14 pagesCABGClaudette CayetanoNo ratings yet
- Acid Base ImbalanceDocument28 pagesAcid Base ImbalanceJean Gwyneth GatchalianNo ratings yet
- 3.46B1 Blood Worksheet 1Document4 pages3.46B1 Blood Worksheet 1Nakeisha Joseph100% (1)
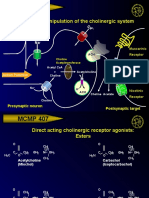
- MCMP 407: Pharmacologic Manipulation of The Cholinergic SystemDocument13 pagesMCMP 407: Pharmacologic Manipulation of The Cholinergic System16_dev5038No ratings yet
- Lesson Plan Simple FormDocument2 pagesLesson Plan Simple FormShaNe BesaresNo ratings yet
- Kerja Kursus Add Math (Johor)Document8 pagesKerja Kursus Add Math (Johor)Muhd MuqriNo ratings yet