Download as pdf or txt
You might also like
- UGB264 Assignment Question - Apr 2021Document10 pagesUGB264 Assignment Question - Apr 2021JisanNo ratings yet
- Suchman Figuring PersonhoodDocument18 pagesSuchman Figuring Personhoodlivelife01No ratings yet
- 2020ciencias Abiertas Suiza Acceso Abierto PDFDocument10 pages2020ciencias Abiertas Suiza Acceso Abierto PDFsanya eusebia lupaca lupacaNo ratings yet
- Efficient GAN-based Chest Radiographs (CXR) Augmentation To Diagnose Coronavirus Disease PneumoniaDocument10 pagesEfficient GAN-based Chest Radiographs (CXR) Augmentation To Diagnose Coronavirus Disease PneumoniaRabah AlobaidyNo ratings yet
- Paper 10-Dinacci2022Document13 pagesPaper 10-Dinacci2022barnacleboy111111No ratings yet
- Pneumonia Classification in Lung X-Ray Images Using CNN TechniqueDocument8 pagesPneumonia Classification in Lung X-Ray Images Using CNN TechniqueIJRASETPublicationsNo ratings yet
- Can AI Help in Screening Viral and COVID-19 PneumoniaDocument12 pagesCan AI Help in Screening Viral and COVID-19 PneumoniaMahesa Kurnianti PutriNo ratings yet
- Covid 19 PredictionDocument6 pagesCovid 19 Predictionchoudharynipun69No ratings yet
- Informatics in Medicine UnlockedDocument13 pagesInformatics in Medicine UnlockedAckshayaNo ratings yet
- Momentum Contrastive Learning For Few-Shot COVID-19 Diagnosis From Chest CT ImagesDocument8 pagesMomentum Contrastive Learning For Few-Shot COVID-19 Diagnosis From Chest CT ImagesLandon GrayNo ratings yet
- PREDICTION OF COVID-19 DIAGNOSIS BASED ON THE SYMPTOMS USING MACHINE LEARNING. by Rohan Ranjan SheeDocument9 pagesPREDICTION OF COVID-19 DIAGNOSIS BASED ON THE SYMPTOMS USING MACHINE LEARNING. by Rohan Ranjan Sheeshoubhik dasNo ratings yet
- Errattahi Et Al. - 2023Document7 pagesErrattahi Et Al. - 2023apatzNo ratings yet
- Intership Report1Document32 pagesIntership Report1Suman GowdaNo ratings yet
- Artificial Intelligence in Pneumonia DetectionDocument4 pagesArtificial Intelligence in Pneumonia DetectionPython JavaNo ratings yet
- COVID Detection Using Symptoms and X-RayDocument10 pagesCOVID Detection Using Symptoms and X-RayIJRASETPublicationsNo ratings yet
- Imu100378 PDFDocument13 pagesImu100378 PDFHaneya NaeemNo ratings yet
- Combatting COVID-19 - 2020 - Ultrasound PDFDocument6 pagesCombatting COVID-19 - 2020 - Ultrasound PDFarnaldops333No ratings yet
- Asif Et Al. - 2023Document19 pagesAsif Et Al. - 2023apatzNo ratings yet
- Multiclass Medical X-Ray Image Classification Using Deep Learning With Explainable AIDocument11 pagesMulticlass Medical X-Ray Image Classification Using Deep Learning With Explainable AIIJRASETPublicationsNo ratings yet
- Pneumonia and COVID-19 Detection Using Convolutional Neural NetworkDocument10 pagesPneumonia and COVID-19 Detection Using Convolutional Neural NetworkIJRASETPublicationsNo ratings yet
- Covid19 and Pneumonia Detection Using Deep-LeaningDocument17 pagesCovid19 and Pneumonia Detection Using Deep-LeaningIJRASETPublicationsNo ratings yet
- Evolution Splits in Two-4Document10 pagesEvolution Splits in Two-4api-534378795No ratings yet
- Modified - Remote Health Monitoring System For Covid 19Document19 pagesModified - Remote Health Monitoring System For Covid 19Flux PrimeNo ratings yet
- COVID-19 Future Forecasting SystemDocument7 pagesCOVID-19 Future Forecasting SystemIJRASETPublicationsNo ratings yet
- Acquisition, Segmentation, and Diagnosis of Imaging Data Using Artificial Intelligence Techniques For COVID-19Document9 pagesAcquisition, Segmentation, and Diagnosis of Imaging Data Using Artificial Intelligence Techniques For COVID-19IJRASETPublicationsNo ratings yet
- Ijbsv 17 P 1581Document7 pagesIjbsv 17 P 1581sarahulfaaNo ratings yet
- Artificial Intelligence and Machine Learning To Fight COVID-19Document3 pagesArtificial Intelligence and Machine Learning To Fight COVID-19Fidel Huanco RamosNo ratings yet
- Covid 19 Health Prediction Using Supervised Learning With OptimizationDocument5 pagesCovid 19 Health Prediction Using Supervised Learning With OptimizationEditor IJTSRDNo ratings yet
- (IJCST-V8I3P13) :pranali Manapure, Kiran Likhar, Hemlata KosareDocument5 pages(IJCST-V8I3P13) :pranali Manapure, Kiran Likhar, Hemlata KosareEighthSenseGroupNo ratings yet
- (IJCST-V9I3P10:Akshat Rustagi, Rudrangshu Tarafder, J. Rene BeulahDocument7 pages(IJCST-V9I3P10:Akshat Rustagi, Rudrangshu Tarafder, J. Rene BeulahEighthSenseGroupNo ratings yet
- Classification of COVID-19 Chest X-Rays With Deep Learning: New Models or Fine Tuning?Document11 pagesClassification of COVID-19 Chest X-Rays With Deep Learning: New Models or Fine Tuning?codelover0007No ratings yet
- Call For Papers Special Issue On Imaging-Based Diagnosis of COVID-19Document2 pagesCall For Papers Special Issue On Imaging-Based Diagnosis of COVID-19Arun Pratap SinghNo ratings yet
- Pandemic Management For Diseases Similar To COVID-19 Using Deep Learning and 5G CommunicationsDocument6 pagesPandemic Management For Diseases Similar To COVID-19 Using Deep Learning and 5G Communicationsmohammed meladNo ratings yet
- Shuja2020 Article COVID-19OpenSourceDataSetsACom PDFDocument30 pagesShuja2020 Article COVID-19OpenSourceDataSetsACom PDFSoumya DasNo ratings yet
- AI in Contact TracingDocument7 pagesAI in Contact Tracingpayal_joshi_14No ratings yet
- Chowdhury Et Al. - 2020Document12 pagesChowdhury Et Al. - 2020apatzNo ratings yet
- Bashar Et Al. - 2021Document18 pagesBashar Et Al. - 2021apatzNo ratings yet
- COVID-19 Detection From Chest X-Rays Using Trained Output Based Transfer Learning ApproachDocument24 pagesCOVID-19 Detection From Chest X-Rays Using Trained Output Based Transfer Learning ApproachAsmaa AbdulQawyNo ratings yet
- 2004 06912Document9 pages2004 06912Gaurav GaggarNo ratings yet
- Artificial Intelligence For COVID-19 Detection - A State-Of-The-Art ReviewDocument24 pagesArtificial Intelligence For COVID-19 Detection - A State-Of-The-Art Reviewkhurram shehzadNo ratings yet
- Biomedical Signal Processing and Control: Prasad Kalane, Sarika Patil, B.P. Patil, Davinder Pal SharmaDocument9 pagesBiomedical Signal Processing and Control: Prasad Kalane, Sarika Patil, B.P. Patil, Davinder Pal SharmaShivam Mani Tripathi x-c 11No ratings yet
- Artificial Intelligence in Disease OutbreakDocument9 pagesArtificial Intelligence in Disease OutbreakAchanya ChristopherNo ratings yet
- The Applications of Artificial Intelligence in Chest Imaging of COVID-19 Patients - A Literature ReviewDocument30 pagesThe Applications of Artificial Intelligence in Chest Imaging of COVID-19 Patients - A Literature ReviewfreteerNo ratings yet
- Automated Chest CT Image Segmentation of COVID-19 Lung Infection Based On 3D U-NetDocument9 pagesAutomated Chest CT Image Segmentation of COVID-19 Lung Infection Based On 3D U-NetballechaseNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument5 pagesDiabetes & Metabolic Syndrome: Clinical Research & Reviewssanya eusebia lupaca lupacaNo ratings yet
- Applsci 12 04825 v2Document23 pagesApplsci 12 04825 v2elkhaoula2009No ratings yet
- Detection of Covid-19 Using Deep LearningDocument6 pagesDetection of Covid-19 Using Deep LearningIJRASETPublicationsNo ratings yet
- DiseasesDocument13 pagesDiseasesoualid-kunNo ratings yet
- Covid 19 Health Prediction Using Supervised Learning With OptimizationDocument8 pagesCovid 19 Health Prediction Using Supervised Learning With OptimizationEditor IJTSRDNo ratings yet
- Journal Pre-Proof: Chaos, Solitons and FractalsDocument62 pagesJournal Pre-Proof: Chaos, Solitons and FractalsSUNDARAMAHALINGAM ANo ratings yet
- Journal Pre-Proof: Chaos, Solitons and FractalsDocument12 pagesJournal Pre-Proof: Chaos, Solitons and FractalsZaima Sartaj TaheriNo ratings yet
- (IJCST-V9I4P15) :unsa Maheen, Khawar Iqbal Malik, Gohar AliDocument9 pages(IJCST-V9I4P15) :unsa Maheen, Khawar Iqbal Malik, Gohar AliEighthSenseGroupNo ratings yet
- Covid19 Prediction Model With Hybrid Approach A ReviewDocument6 pagesCovid19 Prediction Model With Hybrid Approach A ReviewIJRASETPublicationsNo ratings yet
- Covi-Assist Automatic COVID-19 Detection From Chest X-RaysDocument10 pagesCovi-Assist Automatic COVID-19 Detection From Chest X-RaysIJRASETPublicationsNo ratings yet
- Covid-19 Analysis and Detection Using Chest X-Ray ImagesDocument10 pagesCovid-19 Analysis and Detection Using Chest X-Ray ImagesIJRASETPublicationsNo ratings yet
- Presentation 1Document22 pagesPresentation 1Vikas JatNo ratings yet
- Adedoyin Ahmed Hussain Ouns Bouachir Fadi Al-Turjman Moayad AloqailyDocument21 pagesAdedoyin Ahmed Hussain Ouns Bouachir Fadi Al-Turjman Moayad AloqailyIbn Alhalal AlhashimiNo ratings yet
- Blood Glucose Levels Hold Key To Severity of COVID-19 - Technology Networks p3-6Document4 pagesBlood Glucose Levels Hold Key To Severity of COVID-19 - Technology Networks p3-6Khushi GillNo ratings yet
- Islam Et Al. - 2023Document18 pagesIslam Et Al. - 2023apatzNo ratings yet
- Development of Convolutional Neural Network Based Diagnostic System For Detection of Coronavirus Using Magnetic Resonant Imaging Mri.Document22 pagesDevelopment of Convolutional Neural Network Based Diagnostic System For Detection of Coronavirus Using Magnetic Resonant Imaging Mri.Kelvin NnamaniNo ratings yet
- Artificial Intelligence in Healthcare and COVID-19From EverandArtificial Intelligence in Healthcare and COVID-19Parag ChatterjeeNo ratings yet
- Automated School Form 2 - DepEdDocument35 pagesAutomated School Form 2 - DepEdJeff HambreNo ratings yet
- Fourth Grading Period Grade III - Dove: Felipe Carreon Central SchoolDocument2 pagesFourth Grading Period Grade III - Dove: Felipe Carreon Central SchoolJeff HambreNo ratings yet
- Go Winds: Volume 4 Number 4 Winter 2001 $3.00Document12 pagesGo Winds: Volume 4 Number 4 Winter 2001 $3.00Jeff HambreNo ratings yet
- Grading SheetDocument2 pagesGrading SheetJeff HambreNo ratings yet
- A Computer Package For Measuring The STRDocument11 pagesA Computer Package For Measuring The STRJeff HambreNo ratings yet
- A Study of Encryption Algorithms (RSA, DES, 3DES and AES) For Information SecurityDocument6 pagesA Study of Encryption Algorithms (RSA, DES, 3DES and AES) For Information SecurityJeff HambreNo ratings yet
- On Correlation Between The Order of S-Boxes and The Strength of DESDocument10 pagesOn Correlation Between The Order of S-Boxes and The Strength of DESJeff HambreNo ratings yet
- Department of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Document12 pagesDepartment of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Jeff HambreNo ratings yet
- Modified Rsa Encryption Algorithm Using Four Keys IJERTCONV3IS07021Document5 pagesModified Rsa Encryption Algorithm Using Four Keys IJERTCONV3IS07021Jeff HambreNo ratings yet
- Bandwidth Allocation Mechanism Based On Users' Web Usage Patterns For Campus NetworksDocument10 pagesBandwidth Allocation Mechanism Based On Users' Web Usage Patterns For Campus NetworksJeff HambreNo ratings yet
- Novena To Saint Charbel-1Document2 pagesNovena To Saint Charbel-1Jeff HambreNo ratings yet
- Group2 PPT Proposal STEM12 ITDocument26 pagesGroup2 PPT Proposal STEM12 ITJeff HambreNo ratings yet
- Table of Specifications (Tos) : (1-30 Multiple Choice)Document3 pagesTable of Specifications (Tos) : (1-30 Multiple Choice)Jeff HambreNo ratings yet
- 7.6.1 Packet Tracer - WAN ConceptsDocument3 pages7.6.1 Packet Tracer - WAN ConceptsJeff HambreNo ratings yet
- 6.6.7 Packet Tracer - Configure PATDocument4 pages6.6.7 Packet Tracer - Configure PATJeff HambreNo ratings yet
- Developing E-Learning System To Support Teaching and Learning Activities Using DSDM ApproachDocument13 pagesDeveloping E-Learning System To Support Teaching and Learning Activities Using DSDM ApproachJeff HambreNo ratings yet
- Defining The Scourge of COVID-19 Hyperinflammatory Syndrome: Francesco Del GaldoDocument3 pagesDefining The Scourge of COVID-19 Hyperinflammatory Syndrome: Francesco Del GaldoJeff HambreNo ratings yet
- Writing Simple SentencesDocument1 pageWriting Simple SentencesCelestina Tan0% (2)
- 6.8.1 Packet Tracer - Configure NAT For IPv4Document2 pages6.8.1 Packet Tracer - Configure NAT For IPv4Jeff HambreNo ratings yet
- Department of Education: Individual Workweek Accomplishment ReportDocument1 pageDepartment of Education: Individual Workweek Accomplishment ReportJeff HambreNo ratings yet
- Honinbo DotekiDocument19 pagesHoninbo DotekiJeff HambreNo ratings yet
- How To Install Moodle 1Document31 pagesHow To Install Moodle 1Jeff HambreNo ratings yet
- Tally ResearchDocument4 pagesTally ResearchJeff HambreNo ratings yet
- 4 Computer ProgrammingDocument30 pages4 Computer ProgrammingJeff HambreNo ratings yet
- Class 9 Domains of AIDocument28 pagesClass 9 Domains of AIdhanvanth dhanvanthNo ratings yet
- CS361 Lec 02Document31 pagesCS361 Lec 02Omar AhmedNo ratings yet
- Artificial Intelligence Handwritten Notes by RiyaDocument118 pagesArtificial Intelligence Handwritten Notes by RiyaRiya jainNo ratings yet
- Savitribai Phule Pune University: Timetable For Fresh & Backlog Online Examination of October/November 2021Document9 pagesSavitribai Phule Pune University: Timetable For Fresh & Backlog Online Examination of October/November 2021sunny kumarNo ratings yet
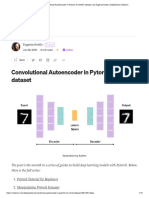
- Convolutional Autoencoder in Pytorch On MNIST Dataset - by Eugenia Anello - DataSeries - MediumDocument18 pagesConvolutional Autoencoder in Pytorch On MNIST Dataset - by Eugenia Anello - DataSeries - Mediumcloud4nrjNo ratings yet
- Sentiment Emotion RecognitionDocument6 pagesSentiment Emotion RecognitionSam RockNo ratings yet
- 03TP Condez John Paul HCIDocument3 pages03TP Condez John Paul HCIJanela Natal MurilloNo ratings yet
- DBSCAN AlgorithmDocument15 pagesDBSCAN AlgorithmMukesh GautamNo ratings yet
- Salesforce AI ReportDocument16 pagesSalesforce AI ReportNidhi SharmaNo ratings yet
- CS101 Quiz 2 Spring 2020 Solved by Waqas EjazDocument5 pagesCS101 Quiz 2 Spring 2020 Solved by Waqas EjazABDURREHMAN Muhammad IbrahimNo ratings yet
- Google Bard GuideDocument64 pagesGoogle Bard GuideBuroshivaDasguptaNo ratings yet
- The Generative AI Paradox in Evaluation: "What It Can Solve, It May Not Evaluate"Document10 pagesThe Generative AI Paradox in Evaluation: "What It Can Solve, It May Not Evaluate"e.sarasuadivNo ratings yet
- Benefits and Risks of Artificial IntelligenceDocument2 pagesBenefits and Risks of Artificial IntelligenceShivdev Sai50% (2)
- 23rd ICCRTS Revised Paper 54Document7 pages23rd ICCRTS Revised Paper 54MiracleNo ratings yet
- Nikhil Srihari: #258, 10 Cross, Kirloskar Layout, Off Hesarghatta Road, Bangalore - 560073Document1 pageNikhil Srihari: #258, 10 Cross, Kirloskar Layout, Off Hesarghatta Road, Bangalore - 560073Anonymous ZpfKTqNo ratings yet
- Business, Management and Economics Engineering: ISSN: 2669-2481 / eISSN: 2669-249X 2023 Volume 21 Issue 01Document11 pagesBusiness, Management and Economics Engineering: ISSN: 2669-2481 / eISSN: 2669-249X 2023 Volume 21 Issue 01Shivam ThakurNo ratings yet
- Battlefield Singularity November 2017Document74 pagesBattlefield Singularity November 2017dhavalnmodiNo ratings yet
- Monte Carlo Tree Search in MonopolyDocument5 pagesMonte Carlo Tree Search in MonopolyKapil KanagalNo ratings yet
- Machine Learning TechniquesDocument11 pagesMachine Learning Techniquesnopal mahingNo ratings yet
- 1 s2.0 S0031320311004006 MainDocument8 pages1 s2.0 S0031320311004006 MainOnur OzdemirNo ratings yet
- Notification: Teacher Training Sessions To Be Conducted by CBSE in Partnership With MicrosoftDocument5 pagesNotification: Teacher Training Sessions To Be Conducted by CBSE in Partnership With MicrosoftSaurav kundaliaNo ratings yet
- Ai 4 AllDocument33 pagesAi 4 AllMihai IlieNo ratings yet
- A Multi Perspective Study On Artificial Intelligence - 2020 - Computers and EduDocument11 pagesA Multi Perspective Study On Artificial Intelligence - 2020 - Computers and EduAko Badu VernzzNo ratings yet
- Afrodreams - AI - Jere Ikongio - (ZKM Artistic Residency NO.2)Document4 pagesAfrodreams - AI - Jere Ikongio - (ZKM Artistic Residency NO.2)Jeremiah IkongioNo ratings yet
- The Social Dilemma: Q1) List Your Key Learnings From This DocumentaryDocument2 pagesThe Social Dilemma: Q1) List Your Key Learnings From This DocumentaryAbeera Ahmed0% (1)
- A Multi-Task Model For Sentiment AnalysisDocument8 pagesA Multi-Task Model For Sentiment AnalysisChibueze Moriah Ihochi-EnwereNo ratings yet
- AI Answer Verifier: FeaturesDocument2 pagesAI Answer Verifier: FeaturesPoojaNo ratings yet
- Data Mining CS4168 Lecture 5 Basics of Classification 1Document25 pagesData Mining CS4168 Lecture 5 Basics of Classification 1alina sheikhNo ratings yet