Download as pdf or txt
You might also like
- UntitledDocument201 pagesUntitledCsongor KicsiNo ratings yet
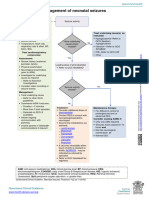
- Neonatal Seizures: Postgraduate Dept of PediatricsDocument42 pagesNeonatal Seizures: Postgraduate Dept of PediatricsG VenkateshNo ratings yet
- IB Psychology Revision Guide - FINALDocument108 pagesIB Psychology Revision Guide - FINALDhyan Valle93% (14)
- Roxana M. Culcer, M.D., FRACP - Aproach To A Collapsed NeonateDocument32 pagesRoxana M. Culcer, M.D., FRACP - Aproach To A Collapsed Neonatenicu 2021No ratings yet
- AAN2023 PedsNCC Case1 Compositeslides 4.13Document14 pagesAAN2023 PedsNCC Case1 Compositeslides 4.13Evelina ȘabanovNo ratings yet
- Recognizing and Managing Increased Intracranial Pressure (ICP)Document4 pagesRecognizing and Managing Increased Intracranial Pressure (ICP)Natalia OrtizNo ratings yet
- Neonatal Seizures: Chairperson - Prof A K Datta Speaker - Dr. SoutrikDocument21 pagesNeonatal Seizures: Chairperson - Prof A K Datta Speaker - Dr. SoutrikbidisNo ratings yet
- 322 Convulsions and Status EpilepticusDocument7 pages322 Convulsions and Status EpilepticusMohammad Irfan khanNo ratings yet
- Status Elipticus April 2018Document2 pagesStatus Elipticus April 2018walidNo ratings yet
- Emergency Presentation of Neurosurgical ConditionsDocument5 pagesEmergency Presentation of Neurosurgical ConditionsMuhammad Azhary LazuardyNo ratings yet
- 2021 SAN BEDA NSIII - SEIZURE and EPILEPSY in Infants and ChildrenDocument57 pages2021 SAN BEDA NSIII - SEIZURE and EPILEPSY in Infants and ChildrenKenneth Torres100% (1)
- Neonatal SeizuresDocument6 pagesNeonatal SeizuresClaraAmeliaNo ratings yet
- Pediatric Neurology Referral Guidelines: Table of ContentsDocument10 pagesPediatric Neurology Referral Guidelines: Table of ContentsEvannelson WardhanaNo ratings yet
- Cerebral Palsy: Signs & Symptoms / Pathophysiology / Drug Studies / Ncps / Health TeachingsDocument22 pagesCerebral Palsy: Signs & Symptoms / Pathophysiology / Drug Studies / Ncps / Health TeachingsGeoffrey Sintaan RiveraNo ratings yet
- Emergencytreatmentof Theseizuringpatient: Emergency MedicineDocument5 pagesEmergencytreatmentof Theseizuringpatient: Emergency Medicinecatalina igorNo ratings yet
- Drug StudyDocument3 pagesDrug StudyCyril_Cybernat_1553No ratings yet
- Paediatrics The Unconscious Child: GCS Measurement in ChildrenDocument2 pagesPaediatrics The Unconscious Child: GCS Measurement in Childrenrekha meenaNo ratings yet
- Evaluation and Management of Status Epilepticus in ChildrenDocument13 pagesEvaluation and Management of Status Epilepticus in ChildrenAyan BiswasNo ratings yet
- Birth AsphyxiaDocument5 pagesBirth Asphyxiacompudoc11No ratings yet
- Neonatal Seizures: Queensland Clinical GuidelinesDocument18 pagesNeonatal Seizures: Queensland Clinical GuidelinesAhmad WardimanNo ratings yet
- 21.2 Seizure in ChildhoodDocument4 pages21.2 Seizure in Childhoodhusenbrz4No ratings yet
- Acute ConfusionDocument7 pagesAcute ConfusionYasin JazNo ratings yet
- Guidelines and Protocols Of: Diabetes EmergenciesDocument36 pagesGuidelines and Protocols Of: Diabetes Emergenciesyassen hassanNo ratings yet
- (UHL CHILDREN) Diabetic Ketoacidosis (DKA) PDFDocument12 pages(UHL CHILDREN) Diabetic Ketoacidosis (DKA) PDFRizki Ismi Arsyad IINo ratings yet
- Frcem Sba Preparation Set 1Document107 pagesFrcem Sba Preparation Set 1jacknaim7090100% (2)
- Lec 4 CNSDocument12 pagesLec 4 CNShusainozelNo ratings yet
- F Seizures AssessDocument1 pageF Seizures Assessmahmudajannatul.7No ratings yet
- Neonatal SeizuresDocument19 pagesNeonatal SeizuresChrisNo ratings yet
- CH 040 Evaluation and Management of Status Epilepticus in ChildrenDocument7 pagesCH 040 Evaluation and Management of Status Epilepticus in Childrensuheena.CNo ratings yet
- NCM 116 - Nursing Care of Patients With Neurologic DysfunctionDocument11 pagesNCM 116 - Nursing Care of Patients With Neurologic DysfunctionRigel Kent C. TobiasNo ratings yet
- Decreased Level of Consciousness in A ChildDocument1 pageDecreased Level of Consciousness in A ChildHayder MuthanaNo ratings yet
- Approach To Comatose Patient: Nurul Izzah Binti AriffinDocument27 pagesApproach To Comatose Patient: Nurul Izzah Binti AriffinNurul IzzahNo ratings yet
- Neurology Paediatric ProtocolDocument44 pagesNeurology Paediatric ProtocolkirannesarajahNo ratings yet
- Clinical Pathway Peds Sepsis 2012Document3 pagesClinical Pathway Peds Sepsis 2012Kim MedairosNo ratings yet
- Head Injury: Closed Head Injury EG: Falls, Motor Vehicle Crashes, Bicycle InjuriesDocument13 pagesHead Injury: Closed Head Injury EG: Falls, Motor Vehicle Crashes, Bicycle InjuriesJudy HandlyNo ratings yet
- Neo SeizureDocument27 pagesNeo SeizureAchyut KanungoNo ratings yet
- Increased Icp NoesDocument3 pagesIncreased Icp NoesDarren Mae MosadaNo ratings yet
- Convulsive Disorders: Presenters: Kabwe Chanda EliasDocument30 pagesConvulsive Disorders: Presenters: Kabwe Chanda EliasHomeground entertainmentNo ratings yet
- Estatus EpilépticoDocument16 pagesEstatus EpilépticoLizbeth PalomecNo ratings yet
- MIS C Algorithim Version 2Document8 pagesMIS C Algorithim Version 2Saima UmairNo ratings yet
- QRH 3-10 Local Anaesthetic Toxicity v2 June 2023Document1 pageQRH 3-10 Local Anaesthetic Toxicity v2 June 2023ReddyNo ratings yet
- Diabetic Ketoacidosis Care Guideline EdDocument2 pagesDiabetic Ketoacidosis Care Guideline EdSeno Adi WicaksonoNo ratings yet
- 4 - Management of Patients With Neurologic Dysfunction Origenal K.Document21 pages4 - Management of Patients With Neurologic Dysfunction Origenal K.Taif SalimNo ratings yet
- 1 - Status EpilepticusDocument82 pages1 - Status EpilepticusfennycarlaNo ratings yet
- (NEURO) 006 SEIZURES-and-EPILEPSYDocument16 pages(NEURO) 006 SEIZURES-and-EPILEPSY3BBEGILJUDY ANNBNo ratings yet
- Pediatric Status Epilepticus CPGDocument7 pagesPediatric Status Epilepticus CPGAndriNo ratings yet
- Hypoglycemia (Moderate or Severe) Diabetic Ketoacidosis (DKA)Document1 pageHypoglycemia (Moderate or Severe) Diabetic Ketoacidosis (DKA)Hanouf BakriNo ratings yet
- Hypoxic Ischemic Encephalopathy (Hie) : AlgorithmDocument11 pagesHypoxic Ischemic Encephalopathy (Hie) : AlgorithmAndreiMunteanuNo ratings yet
- Convulsion, Spasm and UnconsciousnessDocument19 pagesConvulsion, Spasm and UnconsciousnessDesima Tamara sinuratNo ratings yet
- Emergency Neurological Life Support: Status EpilepticusDocument21 pagesEmergency Neurological Life Support: Status EpilepticusElisabeth Permatasari SidabutarNo ratings yet
- Convulsion, Spasm and UnconsciousnessDocument19 pagesConvulsion, Spasm and UnconsciousnessKatrin Marcelina SihombingNo ratings yet
- Status EpilepticusDocument43 pagesStatus EpilepticusPatsuda DreematurakulNo ratings yet
- Henoch-Scholein Purpura - 240524 - 092956Document15 pagesHenoch-Scholein Purpura - 240524 - 092956dakwah mujahadahNo ratings yet
- Neurological EmergenciesDocument11 pagesNeurological Emergenciespunit lakraNo ratings yet
- Shock PresentationDocument20 pagesShock PresentationvgmanjunathNo ratings yet
- Convulsion, Spasm and UnconsciousnessDocument19 pagesConvulsion, Spasm and UnconsciousnessJoko Pratama AtmayudhaNo ratings yet
- MS Lec IicpDocument4 pagesMS Lec IicpTrishia Camille GuillermoNo ratings yet
- 2 - Critical Care Case Studies - LoiDocument51 pages2 - Critical Care Case Studies - Loimadimadi11No ratings yet
- VPK3611 Diseases of The Nervous System Seizures: Intan ShafieDocument29 pagesVPK3611 Diseases of The Nervous System Seizures: Intan Shafieiloveyou_143No ratings yet
- Principles of Seizure ManagementDocument119 pagesPrinciples of Seizure ManagementRenan Toledo SandaloNo ratings yet
- Increased Intracranial Pressure (Iicp)Document3 pagesIncreased Intracranial Pressure (Iicp)رجمه ديوانNo ratings yet
- ABG SamplingDocument4 pagesABG SamplingDeomicah SolanoNo ratings yet
- Physiology Finals ReviewerDocument22 pagesPhysiology Finals ReviewerDeomicah SolanoNo ratings yet
- Aplastic Anemia: Deomicah D. SolanoDocument17 pagesAplastic Anemia: Deomicah D. SolanoDeomicah SolanoNo ratings yet
- Source: Nelson Textbook of Pediatrics 21 Edition, Chapter 273 by Wilbert H. Mason and Hayley A. GansDocument20 pagesSource: Nelson Textbook of Pediatrics 21 Edition, Chapter 273 by Wilbert H. Mason and Hayley A. GansDeomicah SolanoNo ratings yet
- Neurology 1.03 Approach To Cerebral Function - Dr. MartinezDocument7 pagesNeurology 1.03 Approach To Cerebral Function - Dr. MartinezDeomicah SolanoNo ratings yet
- 2 Comparison of Maternal CRP With WBC Count in Predicting Intra Amniotic Infection in Premature Rupture of MembranesDocument4 pages2 Comparison of Maternal CRP With WBC Count in Predicting Intra Amniotic Infection in Premature Rupture of MembranesDeomicah SolanoNo ratings yet
- Dengue in Children 2017Document18 pagesDengue in Children 2017Deomicah SolanoNo ratings yet
- ABG Sampling (10-15 SOLANO) .OdtDocument4 pagesABG Sampling (10-15 SOLANO) .OdtDeomicah SolanoNo ratings yet
- Covid-19 On Pediatric Patients Part 1 (10-15 Solano)Document25 pagesCovid-19 On Pediatric Patients Part 1 (10-15 Solano)Deomicah SolanoNo ratings yet
- Bacterial Identification and StrategiesDocument9 pagesBacterial Identification and StrategiesDeomicah Solano100% (1)
- RBC Morphology and InclusionsDocument3 pagesRBC Morphology and InclusionsDeomicah SolanoNo ratings yet
- Morning Endorsement: October 7, 2020 Group 10 - Subgroup 3Document26 pagesMorning Endorsement: October 7, 2020 Group 10 - Subgroup 3Deomicah SolanoNo ratings yet
- Wound Healing PDFDocument46 pagesWound Healing PDFDeomicah SolanoNo ratings yet
- Pathology Lab 54 - Liver & GallbladderDocument26 pagesPathology Lab 54 - Liver & GallbladderDeomicah SolanoNo ratings yet
- Chest Trauma 2017 PDFDocument96 pagesChest Trauma 2017 PDFDeomicah SolanoNo ratings yet
- RBC&WBC AbnormalitiesDocument10 pagesRBC&WBC AbnormalitiesDeomicah SolanoNo ratings yet
- Varisara Kriya PDFDocument14 pagesVarisara Kriya PDFGottimukkala Muralikrishna100% (1)
- 27 May 2016 Pre-Feasibility Project Report BMWDocument53 pages27 May 2016 Pre-Feasibility Project Report BMWVishal V Bhagwat100% (2)
- Health Science and Food Choices PTC March 2019Document101 pagesHealth Science and Food Choices PTC March 2019IliaNo ratings yet
- Anesthesia Case Report Pulseless VTDocument4 pagesAnesthesia Case Report Pulseless VTLjubomirErdoglijaNo ratings yet
- Public Health Law: Healthy," & How To Balance These Authorities & Duties With "Individual Rights" ToDocument25 pagesPublic Health Law: Healthy," & How To Balance These Authorities & Duties With "Individual Rights" ToMarielle ChuaNo ratings yet
- COVID Cluster Epi Curves 11052020Document1 pageCOVID Cluster Epi Curves 11052020Adrian MojicaNo ratings yet
- An Introduction To Stem CellsDocument14 pagesAn Introduction To Stem CellsAref DahabrahNo ratings yet
- Physiology Lecture 3Document28 pagesPhysiology Lecture 3Muhammad Khubaib AzeemNo ratings yet
- DissociativeidentitydisorderDocument8 pagesDissociativeidentitydisorderapi-355984916No ratings yet
- List of Pharma DrugsDocument6 pagesList of Pharma DrugsAndreaSanchezNo ratings yet
- Reading For Journal WritingDocument4 pagesReading For Journal WritingRAPIDAH BINTI OMAR KPM-GuruNo ratings yet
- 1 s2.0 S2212827122008290 MainDocument6 pages1 s2.0 S2212827122008290 Mainomansukendar03No ratings yet
- Origin of The Pantaneiro Horse in Brazil: Additional Keywords Palabras Clave AdicionalesDocument11 pagesOrigin of The Pantaneiro Horse in Brazil: Additional Keywords Palabras Clave AdicionalesmmbasquesNo ratings yet
- Low-Dose Desoxycorticosterone Pivalate Treatment of Hypoadrenocorticism in Dogs: A Randomized Controlled Clinical TrialDocument9 pagesLow-Dose Desoxycorticosterone Pivalate Treatment of Hypoadrenocorticism in Dogs: A Randomized Controlled Clinical TrialEduardo SantamaríaNo ratings yet
- SHSS Placement Brochure 09 - 11Document31 pagesSHSS Placement Brochure 09 - 11healthsutraNo ratings yet
- Rizal Act3&4Document26 pagesRizal Act3&4ma.antonette orsalNo ratings yet
- Herbal Plants Tamil Names and UsesDocument2 pagesHerbal Plants Tamil Names and UsesBalaji Venktesh100% (1)
- Adolescence: Biosocial Development: The Developing Person Through AdolescenceDocument46 pagesAdolescence: Biosocial Development: The Developing Person Through AdolescenceHUMSS 12ANo ratings yet
- 2000+ MCQS With Solution: of Physics, Chemistry, Biology, Maths & EnglishDocument169 pages2000+ MCQS With Solution: of Physics, Chemistry, Biology, Maths & EnglishMuhammad UmairNo ratings yet
- CFTDocument14 pagesCFTNandeesh Kumar.bNo ratings yet
- International Transcript RequestDocument78 pagesInternational Transcript RequestShahabNo ratings yet
- Lecture 29 30 Thyroid TherapeuticsDocument3 pagesLecture 29 30 Thyroid TherapeuticsAhmed MashalyNo ratings yet
- Trichoscopy Simplified: Ebtisam ElghblawiDocument9 pagesTrichoscopy Simplified: Ebtisam ElghblawidrsunilarrakhNo ratings yet
- The Internship Report OnDocument18 pagesThe Internship Report OnMazhar HaseebNo ratings yet
- Kidney Transplantation: Group 9 Syazwaniyati Nurulasmira Nur Hamiza Siti NursuhadaDocument12 pagesKidney Transplantation: Group 9 Syazwaniyati Nurulasmira Nur Hamiza Siti NursuhadaSiti Nursuhada binti Mohd AminNo ratings yet
- Laboratorijske Pretrage WebDocument127 pagesLaboratorijske Pretrage WebLuka LeskoNo ratings yet
- Colds: What Is A Cold?Document2 pagesColds: What Is A Cold?Mocha BorgsNo ratings yet
- Advocacy Letter-Amy JohnsDocument2 pagesAdvocacy Letter-Amy Johnsapi-239145075No ratings yet