
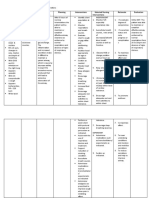
Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluation
Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluation
You might also like
- VSIM Clinical Worksheet 07.10.2020Document6 pagesVSIM Clinical Worksheet 07.10.2020Jackie Griffis100% (1)
- Scalar Wave Laser Protocol ManualDocument40 pagesScalar Wave Laser Protocol ManualAnthony Usera100% (5)
- NCP - Impaired Verbal CommunicationDocument1 pageNCP - Impaired Verbal CommunicationCzarina_May_Tr_429888% (8)
- NCP 1 N 2Document5 pagesNCP 1 N 2Cuttie Anne GalangNo ratings yet
- NCP For Impaired Gas ExchangeDocument2 pagesNCP For Impaired Gas ExchangeSweetie Star94% (16)
- Fatigue NCPDocument2 pagesFatigue NCPclydell joyce masiar100% (6)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationTrisha SuazoNo ratings yet
- NCM 118 SDL#1 - Orcullo 4NFDocument5 pagesNCM 118 SDL#1 - Orcullo 4NFGerelNo ratings yet
- Asthma Nursing Care Plan NCP Ineffective Airway Clearance CompressDocument2 pagesAsthma Nursing Care Plan NCP Ineffective Airway Clearance CompressMargarette GeresNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjectivecammel ramos100% (1)
- NCP Difficulties in BreathingDocument4 pagesNCP Difficulties in BreathingKingJayson Pacman06No ratings yet
- Nursing Care Plan AnemiaDocument3 pagesNursing Care Plan AnemiaNat B. AntipoloNo ratings yet
- CKD Case 2Document16 pagesCKD Case 2Arabylle Maranca AbuelNo ratings yet
- PNNCPDocument2 pagesPNNCPJacky BrightNo ratings yet
- Nursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPDocument2 pagesNursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPLP Benoza100% (2)
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Community Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientDocument4 pagesCommunity Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientKrisianne Mae Lorenzo Francisco100% (1)
- Nursing Care PlanDocument2 pagesNursing Care PlanDenise Garcia MolinaNo ratings yet
- Alteration in OxygenDocument8 pagesAlteration in OxygenBb RabbitNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationJustine Mae A. LoriaNo ratings yet
- NCP Anaphylactic ShockDocument6 pagesNCP Anaphylactic ShockKirstin del CarmenNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- GROUP 8 NCP Patient FDocument12 pagesGROUP 8 NCP Patient FasdasdNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument10 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- Assesment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssesment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- Braga, Patricia 4B (NCM 118)Document4 pagesBraga, Patricia 4B (NCM 118)Jessica BragaNo ratings yet
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternPaolo Anthony GonzalesNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- Septic ShockDocument3 pagesSeptic ShockYuvi Rociandel LUARDONo ratings yet
- Oxygen Administration: Steps RationaleDocument2 pagesOxygen Administration: Steps Rationale2BGrp3Plaza, Anna MaeNo ratings yet
- Work On The Following QuestionsDocument7 pagesWork On The Following QuestionsCenn Dela RosaNo ratings yet
- Cu 4Document3 pagesCu 4Paul SahagunNo ratings yet
- Week 3 - Ms1 Course Task - Cu 3Document2 pagesWeek 3 - Ms1 Course Task - Cu 302 - DIMAYUGA, BRYANNo ratings yet
- Materi Nursing Care PlanDocument1 pageMateri Nursing Care PlanSiti nur Kholifatus samsiyahNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- NCP Hiatal HerniaDocument8 pagesNCP Hiatal HerniaLalaine NadulpitNo ratings yet
- ASSESSMENT NCPDocument4 pagesASSESSMENT NCPjana manaloNo ratings yet
- NCP AsthmaDocument8 pagesNCP Asthmaqweyo yhuNo ratings yet
- NCPDocument7 pagesNCPRuth MontebonNo ratings yet
- Chona NCP 1Document5 pagesChona NCP 1Jan Mark SotoNo ratings yet
- Assessment Planning Intervention Rationale Evaluation: Mechanism of ActionDocument2 pagesAssessment Planning Intervention Rationale Evaluation: Mechanism of ActionNicole CalpoturaNo ratings yet
- Nursing Diagnosis PneumoniaDocument1 pageNursing Diagnosis PneumoniaPasa ShresthaNo ratings yet
- NCP Room 303 TelarmaDocument2 pagesNCP Room 303 TelarmaasdasdNo ratings yet
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument6 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperiencePauline GarciaNo ratings yet
- University of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisDocument3 pagesUniversity of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisLyn MhoreNo ratings yet
- Assessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentDocument10 pagesAssessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentPamela laquindanumNo ratings yet
- Ncp3 CunananDocument2 pagesNcp3 CunananAbbyNo ratings yet
- Week 3 - MS1 COURSE TASK - CU 3Document2 pagesWeek 3 - MS1 COURSE TASK - CU 302 - DIMAYUGA, BRYANNo ratings yet
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternNicole Genevie MallariNo ratings yet
- Lung Cancer N C P BY BHERU LALDocument2 pagesLung Cancer N C P BY BHERU LALBheru Lal100% (1)
- CopdDocument6 pagesCopdapi-3717941100% (2)
- NCP Format 3 CKD Chronic Kidney Disease DM Diabetes Mellitus NephropathyDocument4 pagesNCP Format 3 CKD Chronic Kidney Disease DM Diabetes Mellitus NephropathySapna thakurNo ratings yet
- Intervensi Ispa Dan Oma FixDocument5 pagesIntervensi Ispa Dan Oma FixRizki ArifNo ratings yet
- Nursing Care Plan Assessment Diagnosis Rationale Planning Intervention Rationale Evaluation IndependentDocument13 pagesNursing Care Plan Assessment Diagnosis Rationale Planning Intervention Rationale Evaluation Independentyanny03No ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaNo ratings yet
- Impaired Gas Exchange PneumoniaDocument2 pagesImpaired Gas Exchange PneumoniaShanice BedecirNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- OSMUN Case Study 1 Part 2Document8 pagesOSMUN Case Study 1 Part 2Jay EstrellaNo ratings yet
- System Careplans - Integummentary SystemDocument39 pagesSystem Careplans - Integummentary SystemNicole DouglasNo ratings yet
- Assessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveDocument6 pagesAssessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveIngrid Eunice ConcordiaNo ratings yet
- Ablog Et Al - Abstract-5Document2 pagesAblog Et Al - Abstract-5clydell joyce masiarNo ratings yet
- Drug Mechanism of Action Indication Contraindication Adverse Effects Nursing Responsibility BetahistineDocument16 pagesDrug Mechanism of Action Indication Contraindication Adverse Effects Nursing Responsibility Betahistineclydell joyce masiarNo ratings yet
- 1 ZOO Course Policies and RequirementsDocument28 pages1 ZOO Course Policies and Requirementsclydell joyce masiarNo ratings yet
- Abstract D1 Ablog Et Al EFFECT OF PSYCHOEDUCATION ON SELF-ESTEEM AND SELF-EFFICACY AMONG COLLEGE STUDENTSDocument2 pagesAbstract D1 Ablog Et Al EFFECT OF PSYCHOEDUCATION ON SELF-ESTEEM AND SELF-EFFICACY AMONG COLLEGE STUDENTSclydell joyce masiarNo ratings yet
- Unit 4: Inference and Its Classification 4.1. On InferenceDocument10 pagesUnit 4: Inference and Its Classification 4.1. On Inferenceclydell joyce masiarNo ratings yet
- Figure 1. Conceptual FrameworkDocument3 pagesFigure 1. Conceptual Frameworkclydell joyce masiarNo ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluationclydell joyce masiarNo ratings yet
- Therapeutic Sheet: Date Specific Action Indications Contraindications Side/Adverse Effects Nsg. ResponsibilitiesDocument11 pagesTherapeutic Sheet: Date Specific Action Indications Contraindications Side/Adverse Effects Nsg. Responsibilitiesclydell joyce masiarNo ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluationclydell joyce masiarNo ratings yet
- NCP Skin IntegityDocument3 pagesNCP Skin Integityclydell joyce masiarNo ratings yet
- Airasia RabbaniDocument4 pagesAirasia RabbaniMohd Razif NizamNo ratings yet
- NYSTATIN-nys Tatin S Us Pens Ion Morton Grove Pharmaceuticals, IncDocument5 pagesNYSTATIN-nys Tatin S Us Pens Ion Morton Grove Pharmaceuticals, IncZeyad A AbdullahNo ratings yet
- Child Abuse and NeglectDocument17 pagesChild Abuse and NeglectClaudiaNo ratings yet
- EUCAST Breakpoints V 2.0 120101Document73 pagesEUCAST Breakpoints V 2.0 120101mermarinarNo ratings yet
- Bronchial AsthmaDocument12 pagesBronchial AsthmaRAMNo ratings yet
- Weekly Home Learning Plan/Tasks English For Academic and Professional PurposesDocument11 pagesWeekly Home Learning Plan/Tasks English For Academic and Professional PurposesAze MamalayanNo ratings yet
- UntitledDocument5 pagesUntitledaisyah afiahNo ratings yet
- Tool For Mapping of 4-17 Yr. Old Children: Last First Middle Age Date of BirthDocument4 pagesTool For Mapping of 4-17 Yr. Old Children: Last First Middle Age Date of BirthAlice GCNo ratings yet
- Acute Stroke Management - CUNEUS 2022Document36 pagesAcute Stroke Management - CUNEUS 2022AsiatiNo ratings yet
- Nebosh HSW Sample Slides Ed2Document14 pagesNebosh HSW Sample Slides Ed2Ronald AranhaNo ratings yet
- Emerging and Reemerging Diseases - Programs and Policies On Communicable DiseasesDocument34 pagesEmerging and Reemerging Diseases - Programs and Policies On Communicable DiseasesTim Dequillo100% (1)
- IPIndianJNeurosci 9 4 186 190Document5 pagesIPIndianJNeurosci 9 4 186 190keerthi.sakthi0794No ratings yet
- CKD CaseDocument2 pagesCKD CasePatricia Kaye Tayag CastroNo ratings yet
- Surgical Management of Maxillary and Mandibular Fractures in An Eastern Bluetongue Skink, Tiliqua Scincoides ScincoidesDocument5 pagesSurgical Management of Maxillary and Mandibular Fractures in An Eastern Bluetongue Skink, Tiliqua Scincoides ScincoidesAndres ArbelaezNo ratings yet
- Detection of Generalized Tonic Clonic Seizures and Falls in Unconstraint Environment Using Smartphone AccelerometerDocument12 pagesDetection of Generalized Tonic Clonic Seizures and Falls in Unconstraint Environment Using Smartphone Accelerometerpathy cocreNo ratings yet
- ANTIDOTE 4th YEARDocument64 pagesANTIDOTE 4th YEARAnu AjiNo ratings yet
- Antidiabetic Potential of Acanthaceae Family: Review ArticleDocument8 pagesAntidiabetic Potential of Acanthaceae Family: Review ArticleWulan Klsb6No ratings yet
- Midterm Exam Iii Nursing EnglishDocument3 pagesMidterm Exam Iii Nursing EnglishAlfriedo 008No ratings yet
- Infants of Women With Diabetes - UpToDateDocument16 pagesInfants of Women With Diabetes - UpToDatethelesphol pascalNo ratings yet
- Funda 1Document4 pagesFunda 1almalateNo ratings yet
- PN Dosing 1-Sheet-FINALDocument3 pagesPN Dosing 1-Sheet-FINALAndreea SasuNo ratings yet
- A Potential Framework Convention For Pandemic Preparedness and ResponseDocument12 pagesA Potential Framework Convention For Pandemic Preparedness and ResponseArgiris KaravouliasNo ratings yet
- MAPEH ReviewerDocument10 pagesMAPEH ReviewerAlthea Lexine P. CorpusNo ratings yet
- Understanding Education For Children With DisabilitiesDocument79 pagesUnderstanding Education For Children With DisabilitiesshafNo ratings yet
- Nutrition & GIT Lower 2021Document115 pagesNutrition & GIT Lower 2021Dietary EamcNo ratings yet
- Exam Cram Cheet SheetDocument2 pagesExam Cram Cheet SheetSheila Stenson-Roberts100% (1)
- Emotion and The Human Brain: Antonio R. DamasioDocument6 pagesEmotion and The Human Brain: Antonio R. DamasioBruno XavierNo ratings yet



































































































Download as docx, pdf, or txt
You might also like
- VSIM Clinical Worksheet 07.10.2020Document6 pagesVSIM Clinical Worksheet 07.10.2020Jackie Griffis100% (1)
- Scalar Wave Laser Protocol ManualDocument40 pagesScalar Wave Laser Protocol ManualAnthony Usera100% (5)
- NCP - Impaired Verbal CommunicationDocument1 pageNCP - Impaired Verbal CommunicationCzarina_May_Tr_429888% (8)
- NCP 1 N 2Document5 pagesNCP 1 N 2Cuttie Anne GalangNo ratings yet
- NCP For Impaired Gas ExchangeDocument2 pagesNCP For Impaired Gas ExchangeSweetie Star94% (16)
- Fatigue NCPDocument2 pagesFatigue NCPclydell joyce masiar100% (6)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationTrisha SuazoNo ratings yet
- NCM 118 SDL#1 - Orcullo 4NFDocument5 pagesNCM 118 SDL#1 - Orcullo 4NFGerelNo ratings yet
- Asthma Nursing Care Plan NCP Ineffective Airway Clearance CompressDocument2 pagesAsthma Nursing Care Plan NCP Ineffective Airway Clearance CompressMargarette GeresNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjectivecammel ramos100% (1)
- NCP Difficulties in BreathingDocument4 pagesNCP Difficulties in BreathingKingJayson Pacman06No ratings yet
- Nursing Care Plan AnemiaDocument3 pagesNursing Care Plan AnemiaNat B. AntipoloNo ratings yet
- CKD Case 2Document16 pagesCKD Case 2Arabylle Maranca AbuelNo ratings yet
- PNNCPDocument2 pagesPNNCPJacky BrightNo ratings yet
- Nursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPDocument2 pagesNursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPLP Benoza100% (2)
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Community Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientDocument4 pagesCommunity Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientKrisianne Mae Lorenzo Francisco100% (1)
- Nursing Care PlanDocument2 pagesNursing Care PlanDenise Garcia MolinaNo ratings yet
- Alteration in OxygenDocument8 pagesAlteration in OxygenBb RabbitNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationJustine Mae A. LoriaNo ratings yet
- NCP Anaphylactic ShockDocument6 pagesNCP Anaphylactic ShockKirstin del CarmenNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- GROUP 8 NCP Patient FDocument12 pagesGROUP 8 NCP Patient FasdasdNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument10 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- Assesment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssesment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- Braga, Patricia 4B (NCM 118)Document4 pagesBraga, Patricia 4B (NCM 118)Jessica BragaNo ratings yet
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternPaolo Anthony GonzalesNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- Septic ShockDocument3 pagesSeptic ShockYuvi Rociandel LUARDONo ratings yet
- Oxygen Administration: Steps RationaleDocument2 pagesOxygen Administration: Steps Rationale2BGrp3Plaza, Anna MaeNo ratings yet
- Work On The Following QuestionsDocument7 pagesWork On The Following QuestionsCenn Dela RosaNo ratings yet
- Cu 4Document3 pagesCu 4Paul SahagunNo ratings yet
- Week 3 - Ms1 Course Task - Cu 3Document2 pagesWeek 3 - Ms1 Course Task - Cu 302 - DIMAYUGA, BRYANNo ratings yet
- Materi Nursing Care PlanDocument1 pageMateri Nursing Care PlanSiti nur Kholifatus samsiyahNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- NCP Hiatal HerniaDocument8 pagesNCP Hiatal HerniaLalaine NadulpitNo ratings yet
- ASSESSMENT NCPDocument4 pagesASSESSMENT NCPjana manaloNo ratings yet
- NCP AsthmaDocument8 pagesNCP Asthmaqweyo yhuNo ratings yet
- NCPDocument7 pagesNCPRuth MontebonNo ratings yet
- Chona NCP 1Document5 pagesChona NCP 1Jan Mark SotoNo ratings yet
- Assessment Planning Intervention Rationale Evaluation: Mechanism of ActionDocument2 pagesAssessment Planning Intervention Rationale Evaluation: Mechanism of ActionNicole CalpoturaNo ratings yet
- Nursing Diagnosis PneumoniaDocument1 pageNursing Diagnosis PneumoniaPasa ShresthaNo ratings yet
- NCP Room 303 TelarmaDocument2 pagesNCP Room 303 TelarmaasdasdNo ratings yet
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument6 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperiencePauline GarciaNo ratings yet
- University of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisDocument3 pagesUniversity of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisLyn MhoreNo ratings yet
- Assessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentDocument10 pagesAssessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentPamela laquindanumNo ratings yet
- Ncp3 CunananDocument2 pagesNcp3 CunananAbbyNo ratings yet
- Week 3 - MS1 COURSE TASK - CU 3Document2 pagesWeek 3 - MS1 COURSE TASK - CU 302 - DIMAYUGA, BRYANNo ratings yet
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternNicole Genevie MallariNo ratings yet
- Lung Cancer N C P BY BHERU LALDocument2 pagesLung Cancer N C P BY BHERU LALBheru Lal100% (1)
- CopdDocument6 pagesCopdapi-3717941100% (2)
- NCP Format 3 CKD Chronic Kidney Disease DM Diabetes Mellitus NephropathyDocument4 pagesNCP Format 3 CKD Chronic Kidney Disease DM Diabetes Mellitus NephropathySapna thakurNo ratings yet
- Intervensi Ispa Dan Oma FixDocument5 pagesIntervensi Ispa Dan Oma FixRizki ArifNo ratings yet
- Nursing Care Plan Assessment Diagnosis Rationale Planning Intervention Rationale Evaluation IndependentDocument13 pagesNursing Care Plan Assessment Diagnosis Rationale Planning Intervention Rationale Evaluation Independentyanny03No ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaNo ratings yet
- Impaired Gas Exchange PneumoniaDocument2 pagesImpaired Gas Exchange PneumoniaShanice BedecirNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- OSMUN Case Study 1 Part 2Document8 pagesOSMUN Case Study 1 Part 2Jay EstrellaNo ratings yet
- System Careplans - Integummentary SystemDocument39 pagesSystem Careplans - Integummentary SystemNicole DouglasNo ratings yet
- Assessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveDocument6 pagesAssessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveIngrid Eunice ConcordiaNo ratings yet
- Ablog Et Al - Abstract-5Document2 pagesAblog Et Al - Abstract-5clydell joyce masiarNo ratings yet
- Drug Mechanism of Action Indication Contraindication Adverse Effects Nursing Responsibility BetahistineDocument16 pagesDrug Mechanism of Action Indication Contraindication Adverse Effects Nursing Responsibility Betahistineclydell joyce masiarNo ratings yet
- 1 ZOO Course Policies and RequirementsDocument28 pages1 ZOO Course Policies and Requirementsclydell joyce masiarNo ratings yet
- Abstract D1 Ablog Et Al EFFECT OF PSYCHOEDUCATION ON SELF-ESTEEM AND SELF-EFFICACY AMONG COLLEGE STUDENTSDocument2 pagesAbstract D1 Ablog Et Al EFFECT OF PSYCHOEDUCATION ON SELF-ESTEEM AND SELF-EFFICACY AMONG COLLEGE STUDENTSclydell joyce masiarNo ratings yet
- Unit 4: Inference and Its Classification 4.1. On InferenceDocument10 pagesUnit 4: Inference and Its Classification 4.1. On Inferenceclydell joyce masiarNo ratings yet
- Figure 1. Conceptual FrameworkDocument3 pagesFigure 1. Conceptual Frameworkclydell joyce masiarNo ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluationclydell joyce masiarNo ratings yet
- Therapeutic Sheet: Date Specific Action Indications Contraindications Side/Adverse Effects Nsg. ResponsibilitiesDocument11 pagesTherapeutic Sheet: Date Specific Action Indications Contraindications Side/Adverse Effects Nsg. Responsibilitiesclydell joyce masiarNo ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluationclydell joyce masiarNo ratings yet
- NCP Skin IntegityDocument3 pagesNCP Skin Integityclydell joyce masiarNo ratings yet
- Airasia RabbaniDocument4 pagesAirasia RabbaniMohd Razif NizamNo ratings yet
- NYSTATIN-nys Tatin S Us Pens Ion Morton Grove Pharmaceuticals, IncDocument5 pagesNYSTATIN-nys Tatin S Us Pens Ion Morton Grove Pharmaceuticals, IncZeyad A AbdullahNo ratings yet
- Child Abuse and NeglectDocument17 pagesChild Abuse and NeglectClaudiaNo ratings yet
- EUCAST Breakpoints V 2.0 120101Document73 pagesEUCAST Breakpoints V 2.0 120101mermarinarNo ratings yet
- Bronchial AsthmaDocument12 pagesBronchial AsthmaRAMNo ratings yet
- Weekly Home Learning Plan/Tasks English For Academic and Professional PurposesDocument11 pagesWeekly Home Learning Plan/Tasks English For Academic and Professional PurposesAze MamalayanNo ratings yet
- UntitledDocument5 pagesUntitledaisyah afiahNo ratings yet
- Tool For Mapping of 4-17 Yr. Old Children: Last First Middle Age Date of BirthDocument4 pagesTool For Mapping of 4-17 Yr. Old Children: Last First Middle Age Date of BirthAlice GCNo ratings yet
- Acute Stroke Management - CUNEUS 2022Document36 pagesAcute Stroke Management - CUNEUS 2022AsiatiNo ratings yet
- Nebosh HSW Sample Slides Ed2Document14 pagesNebosh HSW Sample Slides Ed2Ronald AranhaNo ratings yet
- Emerging and Reemerging Diseases - Programs and Policies On Communicable DiseasesDocument34 pagesEmerging and Reemerging Diseases - Programs and Policies On Communicable DiseasesTim Dequillo100% (1)
- IPIndianJNeurosci 9 4 186 190Document5 pagesIPIndianJNeurosci 9 4 186 190keerthi.sakthi0794No ratings yet
- CKD CaseDocument2 pagesCKD CasePatricia Kaye Tayag CastroNo ratings yet
- Surgical Management of Maxillary and Mandibular Fractures in An Eastern Bluetongue Skink, Tiliqua Scincoides ScincoidesDocument5 pagesSurgical Management of Maxillary and Mandibular Fractures in An Eastern Bluetongue Skink, Tiliqua Scincoides ScincoidesAndres ArbelaezNo ratings yet
- Detection of Generalized Tonic Clonic Seizures and Falls in Unconstraint Environment Using Smartphone AccelerometerDocument12 pagesDetection of Generalized Tonic Clonic Seizures and Falls in Unconstraint Environment Using Smartphone Accelerometerpathy cocreNo ratings yet
- ANTIDOTE 4th YEARDocument64 pagesANTIDOTE 4th YEARAnu AjiNo ratings yet
- Antidiabetic Potential of Acanthaceae Family: Review ArticleDocument8 pagesAntidiabetic Potential of Acanthaceae Family: Review ArticleWulan Klsb6No ratings yet
- Midterm Exam Iii Nursing EnglishDocument3 pagesMidterm Exam Iii Nursing EnglishAlfriedo 008No ratings yet
- Infants of Women With Diabetes - UpToDateDocument16 pagesInfants of Women With Diabetes - UpToDatethelesphol pascalNo ratings yet
- Funda 1Document4 pagesFunda 1almalateNo ratings yet
- PN Dosing 1-Sheet-FINALDocument3 pagesPN Dosing 1-Sheet-FINALAndreea SasuNo ratings yet
- A Potential Framework Convention For Pandemic Preparedness and ResponseDocument12 pagesA Potential Framework Convention For Pandemic Preparedness and ResponseArgiris KaravouliasNo ratings yet
- MAPEH ReviewerDocument10 pagesMAPEH ReviewerAlthea Lexine P. CorpusNo ratings yet
- Understanding Education For Children With DisabilitiesDocument79 pagesUnderstanding Education For Children With DisabilitiesshafNo ratings yet
- Nutrition & GIT Lower 2021Document115 pagesNutrition & GIT Lower 2021Dietary EamcNo ratings yet
- Exam Cram Cheet SheetDocument2 pagesExam Cram Cheet SheetSheila Stenson-Roberts100% (1)
- Emotion and The Human Brain: Antonio R. DamasioDocument6 pagesEmotion and The Human Brain: Antonio R. DamasioBruno XavierNo ratings yet