Download as pdf or txt
You might also like
- Dynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionFrom EverandDynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionRating: 5 out of 5 stars5/5 (2)
- Effect of Knee Position On Hip and Knee Torques During The Barbell SquatDocument5 pagesEffect of Knee Position On Hip and Knee Torques During The Barbell SquatMattNo ratings yet
- An Electromyographic Evaluation of Subdividing Active-Assistive Shoulder Elevation ExercisesDocument9 pagesAn Electromyographic Evaluation of Subdividing Active-Assistive Shoulder Elevation ExercisesJuliano BritoNo ratings yet
- Analysis of The Hamstring Muscle Activation During Two Injury Prevention ExercisesDocument9 pagesAnalysis of The Hamstring Muscle Activation During Two Injury Prevention ExercisesJoeNo ratings yet
- Effects of Fatigue On Stability of Upper Extremity During Bench-Press ExerciseDocument5 pagesEffects of Fatigue On Stability of Upper Extremity During Bench-Press Exerciseyp huangNo ratings yet
- The Effects of Kinesio Taping On Quadriceps Strenth During Isokinetic Exercise in Healthy Non-Athlete WomenDocument6 pagesThe Effects of Kinesio Taping On Quadriceps Strenth During Isokinetic Exercise in Healthy Non-Athlete WomenionNo ratings yet
- 2020 Berckmans Finewire AJSMDocument7 pages2020 Berckmans Finewire AJSMLívia PogettiNo ratings yet
- 2020 Berckmans Finewire AJSMDocument7 pages2020 Berckmans Finewire AJSMMariaNo ratings yet
- Biomechanics of The Knee During Closed Kinetic Chain and Open KineticDocument17 pagesBiomechanics of The Knee During Closed Kinetic Chain and Open KineticArmando NetoNo ratings yet
- 1 s2.0 S1356689X15002635 MainDocument5 pages1 s2.0 S1356689X15002635 Mainayşe numanoğluNo ratings yet
- Brazilian Journal of Physical TherapyDocument10 pagesBrazilian Journal of Physical TherapyLuis DavidNo ratings yet
- TMP EBFDDocument9 pagesTMP EBFDFrontiersNo ratings yet
- How Long Does The Protective Effect On Eccentric Exercise-Induced Muscle Damage Last?Document6 pagesHow Long Does The Protective Effect On Eccentric Exercise-Induced Muscle Damage Last?Ricardo Pereira NevesNo ratings yet
- Accepted ManuscriptDocument40 pagesAccepted ManuscriptDaniel CarcamoNo ratings yet
- Ações ExcentricasDocument5 pagesAções ExcentricasJonatas GomesNo ratings yet
- The Effects of Kinesio-Taping On Quadriceps Strength During Isokinetic Exercise in Healthy Non Athlete WomenDocument6 pagesThe Effects of Kinesio-Taping On Quadriceps Strength During Isokinetic Exercise in Healthy Non Athlete WomenSurya DiatmikaNo ratings yet
- Effects of Squat Training With Different Depths On Lower Limb Muscle VolumesDocument10 pagesEffects of Squat Training With Different Depths On Lower Limb Muscle VolumesjoselucasspNo ratings yet
- 29 - Jpts 2017 341Document4 pages29 - Jpts 2017 341Rafii KhairuddinNo ratings yet
- Effects of Kinesiology Taping On Repositioning Error of The Knee Joint After Quadriceps Muscle FatigueDocument3 pagesEffects of Kinesiology Taping On Repositioning Error of The Knee Joint After Quadriceps Muscle FatigueYoga MatiinuNo ratings yet
- Effects of Contract-Relax Vs Static Stretching On Stretch-Induced Strength Loss and Length-Tension RelationshipDocument6 pagesEffects of Contract-Relax Vs Static Stretching On Stretch-Induced Strength Loss and Length-Tension Relationshipjul yanNo ratings yet
- Effect of Kinesio Taping On Muscle Strength in Athletes - A Pilot StudyDocument4 pagesEffect of Kinesio Taping On Muscle Strength in Athletes - A Pilot StudyErnesto LlorcaNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- Emg Deltoide Diferentes Exercicios Silveira Lima 2013 PDFDocument5 pagesEmg Deltoide Diferentes Exercicios Silveira Lima 2013 PDFAlexandreNo ratings yet
- Hamstrings EstabilizadoresDocument8 pagesHamstrings EstabilizadoresFabiano LacerdaNo ratings yet
- 2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseDocument23 pages2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseFrancisco Antonó Castro WeithNo ratings yet
- J Jelekin 2014 06 002 PDFDocument38 pagesJ Jelekin 2014 06 002 PDFRommel AndresNo ratings yet
- 001 Papar 1 EESSDocument6 pages001 Papar 1 EESSEmilio BurgosNo ratings yet
- The Influence of An Unstable Surface On Trunk and Lower Extremity Muscle Activities During Variable Bridging ExercisesDocument3 pagesThe Influence of An Unstable Surface On Trunk and Lower Extremity Muscle Activities During Variable Bridging ExercisesSulvina IbrahimNo ratings yet
- مقاله اسکاتDocument7 pagesمقاله اسکاتZahra BahadoriNo ratings yet
- Effect of Knee Position On Hip and Knee Torques During The Barbell SquatDocument5 pagesEffect of Knee Position On Hip and Knee Torques During The Barbell SquatNicolás ManonniNo ratings yet
- Comparison Between Back Squat, Romanian Deadlift, and Barbell Hip Thrust For Leg and Hip Muscle Activities During Hip ExtensionDocument7 pagesComparison Between Back Squat, Romanian Deadlift, and Barbell Hip Thrust For Leg and Hip Muscle Activities During Hip ExtensionCristian OyarzoNo ratings yet
- Influence of Pistol Squat On Decline AngDocument10 pagesInfluence of Pistol Squat On Decline Angpedroalmeidaferro17No ratings yet
- The Effect of Thoracic Spine MobilizationDocument4 pagesThe Effect of Thoracic Spine MobilizationEric SimasNo ratings yet
- Borreani 2015Document27 pagesBorreani 2015Eduardo CastilloNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- Antagonist Muscle Coactivation During Isokinetic Knee ExtensioDocument10 pagesAntagonist Muscle Coactivation During Isokinetic Knee ExtensiopredragbozicNo ratings yet
- Jpts 26 855Document2 pagesJpts 26 855Yoga MatiinuNo ratings yet
- Note. This Article Will Be Published in A Forthcoming Issue ofDocument24 pagesNote. This Article Will Be Published in A Forthcoming Issue ofIvan PitrulliNo ratings yet
- Kim Et Al - Emg, Core - 2016Document27 pagesKim Et Al - Emg, Core - 2016Lina M GarciaNo ratings yet
- WORRELL Et Al., 1994Document6 pagesWORRELL Et Al., 1994Ismenia HelenaNo ratings yet
- Rehabilitation Exercises To Induce Balanced Scapular Muscle Activity in An Anti-Gravity PostureDocument4 pagesRehabilitation Exercises To Induce Balanced Scapular Muscle Activity in An Anti-Gravity PostureSAMNo ratings yet
- Effects of Respiratory-Muscle Exercise On Spinal CurvatureDocument6 pagesEffects of Respiratory-Muscle Exercise On Spinal CurvatureChris100% (1)
- 04 - Diferenças Biomecanicas Do Agachamento Bulgaro e Tradicional 2021Document11 pages04 - Diferenças Biomecanicas Do Agachamento Bulgaro e Tradicional 2021alan.consultoriafitnessNo ratings yet
- Escamilla Et Al. Biomechanics of The Knee During Closed Kinetic Chain and Open Kinetic Chain ExercisesDocument14 pagesEscamilla Et Al. Biomechanics of The Knee During Closed Kinetic Chain and Open Kinetic Chain ExercisesMariano RosalesNo ratings yet
- Articulo #30Document8 pagesArticulo #30LAURA CAMILA CUBILLOS VILLAMILNo ratings yet
- The Effect of Different Decline Angles On The Biomechanics of Double Limb Squats and The Implications To Clinical and Training PracticeDocument15 pagesThe Effect of Different Decline Angles On The Biomechanics of Double Limb Squats and The Implications To Clinical and Training Practicesebastian floresNo ratings yet
- 10.1007 s40279 013 0073 6Document16 pages10.1007 s40279 013 0073 6Benjamin LeeNo ratings yet
- Effects of Dynamic StretchingDocument7 pagesEffects of Dynamic StretchingElier Cabán GonzálezNo ratings yet
- Effect of Toe-Spread-Out Exercise On Hallux Valgus Angle and Cross-Sectional Area of Abductor Hallucis Muscle in Subjects With Hallux ValgusDocument4 pagesEffect of Toe-Spread-Out Exercise On Hallux Valgus Angle and Cross-Sectional Area of Abductor Hallucis Muscle in Subjects With Hallux ValgusArchana MohantyNo ratings yet
- Can Hip Joint Position Affect Quadriceps Muscle Responses DuringDocument7 pagesCan Hip Joint Position Affect Quadriceps Muscle Responses DuringjoaomouratrabalhoNo ratings yet
- Obesity CuadricepsDocument5 pagesObesity CuadricepsGonzalo Aguayo AlcayagaNo ratings yet
- Elastico No OmbrosDocument9 pagesElastico No OmbrosallanboxeNo ratings yet
- Activation and Torque Deficits in ACL-Reconstructed Patients 4 Months Post-OperativeDocument15 pagesActivation and Torque Deficits in ACL-Reconstructed Patients 4 Months Post-OperativeEurovision RSNo ratings yet
- Abdominal Hollowing and Bracing StrategiesDocument9 pagesAbdominal Hollowing and Bracing StrategiesLTF. Jesús GutiérrezNo ratings yet
- Biomechanics of Front and Back Squat Exercises: Home Search Collections Journals About Contact Us My IopscienceDocument9 pagesBiomechanics of Front and Back Squat Exercises: Home Search Collections Journals About Contact Us My IopsciencealdoNo ratings yet
- Blazevich Et, Al. 2007 - Treino Concentrico Vs Treino ExcentricoDocument12 pagesBlazevich Et, Al. 2007 - Treino Concentrico Vs Treino ExcentricoFábio LanferdiniNo ratings yet
- Intervalo Combinado de Sprint, Pliométrico e Treinamento de Força em Jogadores de Futebol Adolescentes Efeitos Nas Medidas de Velocidade, Força, Potência, Mudança de Direção e Capacidade AnaeróbiaDocument12 pagesIntervalo Combinado de Sprint, Pliométrico e Treinamento de Força em Jogadores de Futebol Adolescentes Efeitos Nas Medidas de Velocidade, Força, Potência, Mudança de Direção e Capacidade AnaeróbiaSheilani MartinsNo ratings yet
- Infographic Progressing Rehabilitation After InjurDocument2 pagesInfographic Progressing Rehabilitation After InjurSheilani MartinsNo ratings yet
- Starting at The Ground Up Range of Motion.9Document12 pagesStarting at The Ground Up Range of Motion.9Sheilani MartinsNo ratings yet
- Snach+e+Clean+Weightlifting Movements From Full Extension The.2015 SCJDocument4 pagesSnach+e+Clean+Weightlifting Movements From Full Extension The.2015 SCJSheilani MartinsNo ratings yet
- Studyprotocol Open Access: Alexandra Hott, Sigurd Liavaag, Niels Gunnar Juel and Jens Ivar BroxDocument8 pagesStudyprotocol Open Access: Alexandra Hott, Sigurd Liavaag, Niels Gunnar Juel and Jens Ivar BroxSheilani MartinsNo ratings yet
- Síndrome de Compressão Torácica 2Document8 pagesSíndrome de Compressão Torácica 2Sheilani MartinsNo ratings yet
- The Assisted Nordic Hamstring Curl: Exercise TechniqueDocument4 pagesThe Assisted Nordic Hamstring Curl: Exercise TechniqueSheilani MartinsNo ratings yet
- Síndrome de Compressão TorácicaDocument4 pagesSíndrome de Compressão TorácicaSheilani MartinsNo ratings yet
- Flexibility Training ConceptsDocument20 pagesFlexibility Training ConceptsSheilani MartinsNo ratings yet
- Capacidade de Sprints Repetidos - Onde EstamosDocument5 pagesCapacidade de Sprints Repetidos - Onde EstamosSheilani MartinsNo ratings yet
- Capacidade de Sprints Repetidos Parte I - Fatores Que Contribuem para A FadigaDocument23 pagesCapacidade de Sprints Repetidos Parte I - Fatores Que Contribuem para A FadigaSheilani MartinsNo ratings yet
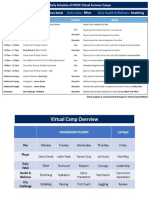
- Sample Daily Schedule Virtual CampDocument2 pagesSample Daily Schedule Virtual CampSheilani MartinsNo ratings yet
- 2014 Pasiakosetal - SportsMed CDocument22 pages2014 Pasiakosetal - SportsMed CSheilani MartinsNo ratings yet
- Journal: Periodization: Period or Question Mark?Document4 pagesJournal: Periodization: Period or Question Mark?Sheilani MartinsNo ratings yet
- Variation in Barbell Position Relative To Shoulder and Foot Anatomical Landmarks Alters Movement EfficiencyDocument13 pagesVariation in Barbell Position Relative To Shoulder and Foot Anatomical Landmarks Alters Movement EfficiencySheilani MartinsNo ratings yet
- Governor and ActuatorDocument36 pagesGovernor and ActuatorPonraj Govindarajan100% (1)
- 100 Questions On Water Biochemistry-1Document19 pages100 Questions On Water Biochemistry-1CnokelvinNo ratings yet
- AP Bio Cram Chart 2021Document1 pageAP Bio Cram Chart 2021Evangeline YaoNo ratings yet
- Design of Terraces 1Document2 pagesDesign of Terraces 1ᜁᜊ ᜀᜎᜆᜂNo ratings yet
- Genetic Engineering and The Intrinsic Value and Integrity of Plants and AnimalsDocument7 pagesGenetic Engineering and The Intrinsic Value and Integrity of Plants and AnimalsCenter for Respect of Life and EnvironmentNo ratings yet
- (S) Topic 1 - IntroductionDocument11 pages(S) Topic 1 - IntroductionKelvin YapNo ratings yet
- Lesson 1Document36 pagesLesson 1Phước NguyễnNo ratings yet
- Markov Decision ProcessDocument11 pagesMarkov Decision ProcessHarpreet Singh BaggaNo ratings yet
- SP Initial 1-5K - ManualDocument37 pagesSP Initial 1-5K - ManualkobochanstoreNo ratings yet
- Crowley - The Crisis in FreemasonryDocument18 pagesCrowley - The Crisis in FreemasonryCelephaïs Press / Unspeakable Press (Leng)100% (4)
- Jan 22 P1R QPDocument36 pagesJan 22 P1R QPAbirNo ratings yet
- The Impact of Inflation On Education: Dr. Jayeeta BhattacharjeeDocument12 pagesThe Impact of Inflation On Education: Dr. Jayeeta BhattacharjeeLiya Mae SantiagoNo ratings yet
- Candy Cos125d 16sDocument21 pagesCandy Cos125d 16srobNo ratings yet
- UntitledDocument4 pagesUntitledGlene NallaNo ratings yet
- MIUX529C: Military SpecificationDocument17 pagesMIUX529C: Military SpecificationJhan Carlos RamosNo ratings yet
- VSP Final ReportDocument53 pagesVSP Final ReportAnand GautamNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsNORFADHLI ARIFNo ratings yet
- Extreme Loading For Structures - WikipediaDocument5 pagesExtreme Loading For Structures - WikipediaEn Iyisi İnşaat MühendisiNo ratings yet
- Functions of MerchandiserDocument26 pagesFunctions of MerchandiseryuktiNo ratings yet
- Coolnomixac 1Document2 pagesCoolnomixac 1Eko AdiNo ratings yet
- SM Project Report - P&GDocument22 pagesSM Project Report - P&GNikhil AjwaniNo ratings yet
- Downloaded From Manuals Search EngineDocument24 pagesDownloaded From Manuals Search EnginekevenNo ratings yet
- Tube To Tube SheetDocument9 pagesTube To Tube Sheetcmpatel_00100% (2)
- Prerequisites From Differential Geometry: 1 Isotopies and Vector FieldsDocument8 pagesPrerequisites From Differential Geometry: 1 Isotopies and Vector FieldsnotafacefuckerNo ratings yet
- 2014 2015 Student Prospectus PDFDocument42 pages2014 2015 Student Prospectus PDFFlorentina EcaterinaNo ratings yet
- Belief and Conditions in Environmental AwarenessDocument28 pagesBelief and Conditions in Environmental AwarenessDanielle Kate MadridNo ratings yet
- A New Mutuel Kerberos Authentication Protocol For Distributed SystemsDocument10 pagesA New Mutuel Kerberos Authentication Protocol For Distributed SystemsRahul prabhaNo ratings yet
- Olokun - The Yoruban Goddess of The Deep Dark Sea - Goddess InspiredDocument10 pagesOlokun - The Yoruban Goddess of The Deep Dark Sea - Goddess InspiredCaetano Rocha50% (2)
- Lab 7b - Bilateral Transfer and Observational LearningDocument3 pagesLab 7b - Bilateral Transfer and Observational Learningapi-448989844No ratings yet
- Principle of Maximum Social AdvantageDocument19 pagesPrinciple of Maximum Social AdvantageAmandeep Singh MankuNo ratings yet