Download as pdf or txt
You might also like
- Whats It Like To Live Without ElectricityDocument7 pagesWhats It Like To Live Without ElectricityYazmin Rios100% (2)
- A SWOT Analysis of McdonaldsDocument5 pagesA SWOT Analysis of Mcdonaldsannesangalang100% (1)
- Contoh Jsa Confined SpaceDocument1 pageContoh Jsa Confined SpaceUnique Gift75% (4)
- NovemberWorkoutCalendar 2019 Funfittcom withSusanaYabarDocument1 pageNovemberWorkoutCalendar 2019 Funfittcom withSusanaYabarLeidy Mosquera100% (1)
- Model Calculations of Aerosol Transmission and Infection Risk of COVID-19 in Indoor EnvironmentsDocument18 pagesModel Calculations of Aerosol Transmission and Infection Risk of COVID-19 in Indoor EnvironmentsAndrés QuinteroNo ratings yet
- Testing Mobile Air Purifiers in A School Classroom: Reducing The Airborne Transmission Risk For Sars-Cov-2Document35 pagesTesting Mobile Air Purifiers in A School Classroom: Reducing The Airborne Transmission Risk For Sars-Cov-2energinnovaNo ratings yet
- Modes of Transmission of Sars-Cov-2 and Evidence For Preventive Behavioral InterventionsDocument9 pagesModes of Transmission of Sars-Cov-2 and Evidence For Preventive Behavioral InterventionsNkosi MNo ratings yet
- Environment International: CorrespondenceDocument7 pagesEnvironment International: CorrespondenceEric CarsonNo ratings yet
- Disinfection Methods Against SARS-CoV-2Document35 pagesDisinfection Methods Against SARS-CoV-2GTNo ratings yet
- Guidance For Otolaryngology Health Care Workers Performing Aerosol Generating Medical Procedures During The COVID-19 PandemicDocument8 pagesGuidance For Otolaryngology Health Care Workers Performing Aerosol Generating Medical Procedures During The COVID-19 PandemicUsuario CyVNo ratings yet
- Transmission of Sars-Cov-2: Implications For Infection Prevention PrecautionsDocument10 pagesTransmission of Sars-Cov-2: Implications For Infection Prevention PrecautionsPaulina AcostaNo ratings yet
- The National Academies PressDocument4 pagesThe National Academies PressjmfercNo ratings yet
- Heating, Ventilation and Air-Conditioning Systems in The Context of COVID-19Document5 pagesHeating, Ventilation and Air-Conditioning Systems in The Context of COVID-19Alex FandaNo ratings yet
- Summary of ThesisDocument2 pagesSummary of ThesisKyo ChihiroNo ratings yet
- 2021 04 21 21255898v2 FullDocument31 pages2021 04 21 21255898v2 FullfrehanyaqNo ratings yet
- Sars-Cov-2 Aerosol Transmission in Schools: The Effectiveness of Different InterventionsDocument18 pagesSars-Cov-2 Aerosol Transmission in Schools: The Effectiveness of Different InterventionseswaynedNo ratings yet
- Distinct Regimes of Particle and Virus Abundance eDocument10 pagesDistinct Regimes of Particle and Virus Abundance eGustavo MiguelNo ratings yet
- Airborne Sars Cov-2Document8 pagesAirborne Sars Cov-2Ikmah FauzanNo ratings yet
- Disinfection Methods Against Sars-Cov-2: A Systematic ReviewDocument34 pagesDisinfection Methods Against Sars-Cov-2: A Systematic ReviewFlori TabacaruNo ratings yet
- Aerodynamic Characteristics and RNA Concentration of SARS-CoV-2 Aerosol in Wuhan Hospitals During COVID-19 OutbreakDocument9 pagesAerodynamic Characteristics and RNA Concentration of SARS-CoV-2 Aerosol in Wuhan Hospitals During COVID-19 OutbreakAleks Guevara PalaciosNo ratings yet
- Ten Reason Airborne Covid19 92Document3 pagesTen Reason Airborne Covid19 92Miguel AgapitoNo ratings yet
- Transmission of Sars-Cov-2 by Inhalation of Respiratory Aerosol in The Skagit Valley Chorale Superspreading EventDocument17 pagesTransmission of Sars-Cov-2 by Inhalation of Respiratory Aerosol in The Skagit Valley Chorale Superspreading EventIgor FerreiraNo ratings yet
- Aerosol DetectionDocument8 pagesAerosol DetectioncristinadoinacroitoruNo ratings yet
- Mick-Murphy2020 Article Aerosol-generatingOtolaryngoloDocument10 pagesMick-Murphy2020 Article Aerosol-generatingOtolaryngoloayuines lassyaniNo ratings yet
- Ten Scientific Reasons in Support of Airborne Transmission of Sars-Cov-2Document3 pagesTen Scientific Reasons in Support of Airborne Transmission of Sars-Cov-2tuanda222No ratings yet
- Ashrae RaspunsDocument3 pagesAshrae RaspunsCTHNo ratings yet
- A. Eiband-Airbornetransmission PDFDocument3 pagesA. Eiband-Airbornetransmission PDFdinda hafniNo ratings yet
- Airborne Transmission Route of COVID-19: Why 2 Meters Be EnoughDocument6 pagesAirborne Transmission Route of COVID-19: Why 2 Meters Be EnoughCamargo Pinto LeonardoNo ratings yet
- RRLDocument5 pagesRRLLauro EspirituNo ratings yet
- Mascaras en Centros de EnseñanzaDocument77 pagesMascaras en Centros de EnseñanzaxomalogaNo ratings yet
- It Is Time To Address Airborne Transmission of Coronavirus Disease 2019 (COVID-19)Document4 pagesIt Is Time To Address Airborne Transmission of Coronavirus Disease 2019 (COVID-19)Putrisuci AndytichaNo ratings yet
- Heating Ventilation Air Conditioning Systems in The Context of COVID 19 First UpdateDocument19 pagesHeating Ventilation Air Conditioning Systems in The Context of COVID 19 First Updatezicus2010No ratings yet
- City and Environment Interactions: Prashant Kumar Lidia MorawskaDocument3 pagesCity and Environment Interactions: Prashant Kumar Lidia MorawskaFelipe PinheiroNo ratings yet
- COVID-19 Superspreader 2021Document6 pagesCOVID-19 Superspreader 2021Ricardo SousaNo ratings yet
- Accepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Document9 pagesAccepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Anonymous 9wHscMNo ratings yet
- COVID-19 and The Ocular Surface A Review of Transmission and Manifestations.Document10 pagesCOVID-19 and The Ocular Surface A Review of Transmission and Manifestations.Nicolás Alejandro López AranedaNo ratings yet
- Protection and Disinfection Policies Against Sars-Cov-2 (Covid-19)Document7 pagesProtection and Disinfection Policies Against Sars-Cov-2 (Covid-19)Muhammad Aufar Rizqi KusumaNo ratings yet
- Airborne SARSCoV2 Weighing The Evidence For Its Role in Community TransmissionJournal of Preventive Medicine and Public HealthDocument2 pagesAirborne SARSCoV2 Weighing The Evidence For Its Role in Community TransmissionJournal of Preventive Medicine and Public HealthJaneth Milagros Cantoral MilianNo ratings yet
- Airborne Transmission of SARS-CoV-2Document3 pagesAirborne Transmission of SARS-CoV-2aranna lalNo ratings yet
- Airborne Transmission of SARS-CoV-2 The World ShouDocument11 pagesAirborne Transmission of SARS-CoV-2 The World ShouAlfian Silvia KrisnasariNo ratings yet
- Medical Hypotheses: SciencedirectDocument5 pagesMedical Hypotheses: SciencedirectRizka DaengNo ratings yet
- Environment International: Lidia Morawska, Junji Cao TDocument3 pagesEnvironment International: Lidia Morawska, Junji Cao TGreysia ManarisipNo ratings yet
- Accepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Document9 pagesAccepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Jeff ReevesNo ratings yet
- Accepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Document9 pagesAccepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Jeff ReevesNo ratings yet
- Alr 22661Document7 pagesAlr 22661Claudio SollarenNo ratings yet
- How Can Airborne Transmission of COVID-19 Indoors Be Minimised?Document7 pagesHow Can Airborne Transmission of COVID-19 Indoors Be Minimised?Arya PrimanandaNo ratings yet
- Comprehensive Review of Mask Utility and Challenges During The COVID-19 PandemicDocument7 pagesComprehensive Review of Mask Utility and Challenges During The COVID-19 PandemicKarinaayu SerinNo ratings yet
- A Mathematical Framework For Estimating Risk of Airborne Transmission of COVID-19 With Application To Face Mask Use and Social DistancingDocument16 pagesA Mathematical Framework For Estimating Risk of Airborne Transmission of COVID-19 With Application To Face Mask Use and Social DistancingPersonalGrowthTipsNo ratings yet
- Impact of HVAC-Systems On The Dispersion of Infectious Aerosols in A Cardiac Intensive Care UnitDocument17 pagesImpact of HVAC-Systems On The Dispersion of Infectious Aerosols in A Cardiac Intensive Care UnitJimmy AnticonaNo ratings yet
- Letter To The Editor: April 2021Document4 pagesLetter To The Editor: April 2021alexNo ratings yet
- 2020 Troeltzschbrothers Covid-19 EngDocument6 pages2020 Troeltzschbrothers Covid-19 Engdamsia-1No ratings yet
- 1 s2.0 S0195670121002619 MainDocument10 pages1 s2.0 S0195670121002619 MainM Arif YudhiantoroNo ratings yet
- Can The New Type of Coronavirus Be Transmitted Via Food and ObjectsDocument10 pagesCan The New Type of Coronavirus Be Transmitted Via Food and Objectsdipoma3612No ratings yet
- Accepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Document9 pagesAccepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19hazemnhNo ratings yet
- Testing Mobile Air Purifiers in A School Classroom - Reducing The Airborne Transmission Risk For SARSDocument15 pagesTesting Mobile Air Purifiers in A School Classroom - Reducing The Airborne Transmission Risk For SARSDhananshu AcharyaNo ratings yet
- Preventive Guidelines For Disinfection and Microbiological Processes During Handling of COVID-19 SamplesDocument5 pagesPreventive Guidelines For Disinfection and Microbiological Processes During Handling of COVID-19 SamplesDaniela Alejandra EstupiñanNo ratings yet
- IPArchCytolHistopatholRes 5 2 111 1151Document6 pagesIPArchCytolHistopatholRes 5 2 111 1151LyonTrioréNo ratings yet
- 2020 Article 475Document6 pages2020 Article 475Karinaayu SerinNo ratings yet
- COVID-19 Dentistry-Related Aspects: A Literature: Concise ReviewDocument6 pagesCOVID-19 Dentistry-Related Aspects: A Literature: Concise ReviewSofiaNo ratings yet
- Estudio de CarrageninaDocument25 pagesEstudio de CarrageninaCarlos MendozaNo ratings yet
- Reducing Transmission of Sars-Cov-2: Kimberly A. Prather, Chia C. Wang, Robert T. SchooleyDocument5 pagesReducing Transmission of Sars-Cov-2: Kimberly A. Prather, Chia C. Wang, Robert T. SchooleyAselya AsanbekovaNo ratings yet
- AEROSOL TRANSMISSION OF SarsDocument20 pagesAEROSOL TRANSMISSION OF SarsAshwini BunkarNo ratings yet
- Testing Mobile Air Purifiers in A School Classroom: Reducing The Airborne Transmission Risk For Sars-Cov-2Document35 pagesTesting Mobile Air Purifiers in A School Classroom: Reducing The Airborne Transmission Risk For Sars-Cov-2energinnovaNo ratings yet
- 6 MODEL-CALIB RiedikerDocument10 pages6 MODEL-CALIB RiedikerenerginnovaNo ratings yet
- Data Sheet DPC310Document2 pagesData Sheet DPC310energinnovaNo ratings yet
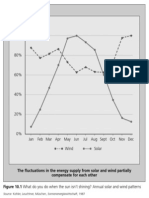
- Figure11 18Document1 pageFigure11 18energinnovaNo ratings yet
- Promoting Renewable Energy: Figure 11.20 Renewables For Off-Grid ApplicationsDocument1 pagePromoting Renewable Energy: Figure 11.20 Renewables For Off-Grid ApplicationsenerginnovaNo ratings yet
- Promoting Renewable Energy: Figure 11.19 Phasing Out NuclearDocument1 pagePromoting Renewable Energy: Figure 11.19 Phasing Out NuclearenerginnovaNo ratings yet
- Collector Area in M: Promoting Renewable EnergyDocument1 pageCollector Area in M: Promoting Renewable EnergyenerginnovaNo ratings yet
- Solar Heat Generator: Cost of Fossil HeatDocument1 pageSolar Heat Generator: Cost of Fossil HeatenerginnovaNo ratings yet
- Promoting Renewable Energy: Industrial FirmDocument1 pagePromoting Renewable Energy: Industrial FirmenerginnovaNo ratings yet
- Figure11 16Document1 pageFigure11 16energinnovaNo ratings yet
- Hydropower Waste and Mine Gas Biomass: Promoting Renewable EnergyDocument1 pageHydropower Waste and Mine Gas Biomass: Promoting Renewable EnergyenerginnovaNo ratings yet
- Why Officer Adam Dreams of The Sun: Promoting Renewable EnergyDocument1 pageWhy Officer Adam Dreams of The Sun: Promoting Renewable EnergyenerginnovaNo ratings yet
- Here, Taking The Example of Solar Thermal Arrays For Rented ApartmentsDocument1 pageHere, Taking The Example of Solar Thermal Arrays For Rented ApartmentsenerginnovaNo ratings yet
- Additional Installed Wind Power Capacity in 2004: Promoting Renewable EnergyDocument1 pageAdditional Installed Wind Power Capacity in 2004: Promoting Renewable EnergyenerginnovaNo ratings yet
- Promoting Renewable Energy: Overall Need For Funding (Depending On Energy Prices)Document1 pagePromoting Renewable Energy: Overall Need For Funding (Depending On Energy Prices)energinnovaNo ratings yet
- Promoting Renewable Energy: Figure 11.11 German Feed-In Rates Abroad: Countries With Feed-In Rates For RenewableDocument1 pagePromoting Renewable Energy: Figure 11.11 German Feed-In Rates Abroad: Countries With Feed-In Rates For RenewableenerginnovaNo ratings yet
- Figure11 12Document1 pageFigure11 12energinnovaNo ratings yet
- Figure10 3Document1 pageFigure10 3energinnovaNo ratings yet
- Supported Collector Area in M 40,000: Promoting Renewable EnergyDocument1 pageSupported Collector Area in M 40,000: Promoting Renewable EnergyenerginnovaNo ratings yet
- Promoting Renewable Energy: Figure 11.9 From The Feed-In Act To The Renewable Energy ActDocument1 pagePromoting Renewable Energy: Figure 11.9 From The Feed-In Act To The Renewable Energy ActenerginnovaNo ratings yet
- Promoting Renewable Energy: (German Market Incentive Programme 2005)Document1 pagePromoting Renewable Energy: (German Market Incentive Programme 2005)energinnovaNo ratings yet
- Figure11 8Document1 pageFigure11 8energinnovaNo ratings yet
- Figure 10.6 The Solar Age: The End of Power Monopolies? The Share of Private PowerDocument1 pageFigure 10.6 The Solar Age: The End of Power Monopolies? The Share of Private PowerenerginnovaNo ratings yet
- Ecological Taxation Reform: Promoting Renewable EnergyDocument1 pageEcological Taxation Reform: Promoting Renewable EnergyenerginnovaNo ratings yet
- Promoting Renewable Energy: Current Energy Research Funding in Millions of Euros (2005-2008)Document1 pagePromoting Renewable Energy: Current Energy Research Funding in Millions of Euros (2005-2008)energinnovaNo ratings yet
- 85,000 Jobs in The Wind Power Sector in Germany (2008) : Concrete Sector Steel SectorDocument1 page85,000 Jobs in The Wind Power Sector in Germany (2008) : Concrete Sector Steel SectorenerginnovaNo ratings yet
- Figure10 4Document1 pageFigure10 4energinnovaNo ratings yet
- Figure10 1Document1 pageFigure10 1energinnovaNo ratings yet
- Figure 10.2 How Much Energy Can Be Stored? Energy Storage With Compressed Air SystemsDocument1 pageFigure 10.2 How Much Energy Can Be Stored? Energy Storage With Compressed Air SystemsenerginnovaNo ratings yet
- Biogas Unit Woodchip-Fired Heating Plant: Current Use and PotentialDocument1 pageBiogas Unit Woodchip-Fired Heating Plant: Current Use and PotentialenerginnovaNo ratings yet
- CAFFEINEDocument2 pagesCAFFEINEVithya RamanathanNo ratings yet
- E - Waste and Its ManagementDocument10 pagesE - Waste and Its ManagementindrapriyaNo ratings yet
- 4.1 Division of WorksDocument32 pages4.1 Division of Worksruhul01No ratings yet
- To Hell and Back DR RawlingsDocument24 pagesTo Hell and Back DR RawlingsF5001100% (2)
- EXAM 2 RationaleDocument1 pageEXAM 2 RationaleSkye M. PetersNo ratings yet
- Putra, 003 - 3035 - I Wayan Adi Pranata - GalleyDocument7 pagesPutra, 003 - 3035 - I Wayan Adi Pranata - Galleyeunike jaequelineNo ratings yet
- Brain DumpDocument59 pagesBrain Dumpruchitac28No ratings yet
- Draft: This Part Is Prepared by Kajal Sapra and Oshadi Puhabhugoda ArachchigedoDocument6 pagesDraft: This Part Is Prepared by Kajal Sapra and Oshadi Puhabhugoda ArachchigedoAmandeep SidhuNo ratings yet
- CPG On Immunization For WomenDocument28 pagesCPG On Immunization For WomenYnoli DiosomitoNo ratings yet
- Chain Pulley Block JsaDocument2 pagesChain Pulley Block JsaAKBAR ALINo ratings yet
- Shannon O'Leary v. New York City Department of Education, Et Al.Document54 pagesShannon O'Leary v. New York City Department of Education, Et Al.Eric SandersNo ratings yet
- True FalseDocument9 pagesTrue FalseHạnh Phan ThiNo ratings yet
- Oral Semaglutide Induces Loss of Body Fat Mass Without Affecting Muscle Mass in Patients With Type 2 DiabetesDocument7 pagesOral Semaglutide Induces Loss of Body Fat Mass Without Affecting Muscle Mass in Patients With Type 2 DiabetesfbonillaNo ratings yet
- Organizational BehaviorDocument6 pagesOrganizational BehaviorprachiNo ratings yet
- 4 PDFDocument11 pages4 PDFHrishikesh BapatNo ratings yet
- Araujo-9788575415986 LibroDocument441 pagesAraujo-9788575415986 LibroMaria Luisa Gutierrez AguileraNo ratings yet
- Do 208 MH Workplace GuidelinesDocument42 pagesDo 208 MH Workplace GuidelinesxavNo ratings yet
- Amagram in 65Document43 pagesAmagram in 65dgshailNo ratings yet
- Indonesian Longitudinal Survey On Mental Health and Social Factors (INDOLUMEN) - Early Findings and ProtocolDocument35 pagesIndonesian Longitudinal Survey On Mental Health and Social Factors (INDOLUMEN) - Early Findings and ProtocolReni Tri AstutiNo ratings yet
- Weight Loss Drugs MDocument2 pagesWeight Loss Drugs MYana PopovaNo ratings yet
- Health Apprehensive Level of Canteen Workers in Western Mindanao State University On Carbon MonoxideDocument10 pagesHealth Apprehensive Level of Canteen Workers in Western Mindanao State University On Carbon Monoxideruth lopezNo ratings yet
- GVHDDocument35 pagesGVHDSaad KhanNo ratings yet
- OCA Circular No. 119-2021 Court Operations Sep 8-30,2021Document2 pagesOCA Circular No. 119-2021 Court Operations Sep 8-30,2021bbysheNo ratings yet
- Evaluasi Program Pemberian Makanan Tambahan Pemulihan (PMT-P) Terhadap Status Gizi Buruk Balita Di Puskesmas Oepoi Kota KupangDocument8 pagesEvaluasi Program Pemberian Makanan Tambahan Pemulihan (PMT-P) Terhadap Status Gizi Buruk Balita Di Puskesmas Oepoi Kota KupangLeni PurbasariNo ratings yet
- 10 1002@aorn 12696Document7 pages10 1002@aorn 12696Salim RumraNo ratings yet
- SBNS Summer Newsletter 2015Document8 pagesSBNS Summer Newsletter 2015Nic RaneteNo ratings yet