Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Andromeda Shock Trial 2020Document3 pagesAndromeda Shock Trial 2020Alejo ZubietaNo ratings yet
- Judicious Utilization of Healthcare Resources .5Document7 pagesJudicious Utilization of Healthcare Resources .5sara shehadaNo ratings yet
- Pantoea Agglomerans - ADocument9 pagesPantoea Agglomerans - AmadelaineNo ratings yet
- Ten Answers To Key Questions For Fluid Management Inintensive CareDocument11 pagesTen Answers To Key Questions For Fluid Management Inintensive CareAndres RiveraNo ratings yet
- Leonel DDocument10 pagesLeonel DFredy DominguezNo ratings yet
- Microbiology and Parasitology Summary and ChartsDocument54 pagesMicrobiology and Parasitology Summary and Chartssciencetopic4No ratings yet
- Critical Care Anesthesiology: Dr. Navid Shafigh Fellowship of Critical Care MedicineDocument54 pagesCritical Care Anesthesiology: Dr. Navid Shafigh Fellowship of Critical Care Medicineamir pouyaNo ratings yet
- Clinical Audit Proposal-2Document18 pagesClinical Audit Proposal-2biniam yohannes100% (2)
- Sofa ScoreDocument6 pagesSofa ScoreNadiah Umniati SyarifahNo ratings yet
- Surgical Critical Care ReviewDocument70 pagesSurgical Critical Care ReviewSteven GodelmanNo ratings yet
- 2020 Ortoleva - Vasoplegia During Cardiopulmonary Bypass Current Literature and Rescue Therapy OptionsDocument10 pages2020 Ortoleva - Vasoplegia During Cardiopulmonary Bypass Current Literature and Rescue Therapy OptionsRizal Muhammad100% (1)
- Anuria, Types & ManagementDocument20 pagesAnuria, Types & Managementapi-3815243100% (2)
- Frando-Detailed Learning Module 7.2.Document15 pagesFrando-Detailed Learning Module 7.2.Ranz Kenneth G. FrandoNo ratings yet
- Golden Hour CCM Arthur Van Zanten IC1Document3 pagesGolden Hour CCM Arthur Van Zanten IC1Sara NicholsNo ratings yet
- SHOCKDocument17 pagesSHOCKChithra Saju100% (1)
- Sepsis Power Point Slide Presentation - The Guidelines - Implementation For The FutureDocument25 pagesSepsis Power Point Slide Presentation - The Guidelines - Implementation For The Futuremontie13No ratings yet
- Advanced Pa Tho Physiology Tree - CellulitisDocument1 pageAdvanced Pa Tho Physiology Tree - CellulitisElyse NavarroNo ratings yet
- Homeopathy and ICUDocument8 pagesHomeopathy and ICUBABLU ROYNo ratings yet
- PG Entrance Surgery MCQsDocument245 pagesPG Entrance Surgery MCQsUsamaArbabNo ratings yet
- Clinical Pharmacokinetics in Burn Patients 1 PDFDocument8 pagesClinical Pharmacokinetics in Burn Patients 1 PDFClaudio Luis VenturiniNo ratings yet
- Abstract Poster ICU Without Wall DR Cerah Wati Paskah PurbaDocument1 pageAbstract Poster ICU Without Wall DR Cerah Wati Paskah PurbaCerah PurbaNo ratings yet
- Equine Synovial Fluid AnalysisDocument18 pagesEquine Synovial Fluid AnalysisHarvey MartinezNo ratings yet
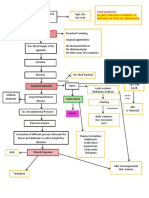
- CPC - Appendicitis (Flowchart)Document1 pageCPC - Appendicitis (Flowchart)Milet NacionalesNo ratings yet
- Surgery Crashcourse PDFDocument545 pagesSurgery Crashcourse PDFjlhotaru100% (1)
- Postoperative Enterocutaneous FistulaDocument10 pagesPostoperative Enterocutaneous FistulaJoon RaynerNo ratings yet
- Neonatal-Perinatal Infections An UpdateDocument215 pagesNeonatal-Perinatal Infections An Updatebromean.cubitos-0qNo ratings yet
- DNB Paediatrics Question PaperDocument37 pagesDNB Paediatrics Question Papermrs raam100% (2)
- 2021 - NEJM - The Evolving Challenge of Infections in CirrhosisDocument14 pages2021 - NEJM - The Evolving Challenge of Infections in CirrhosisHồ Huy HoàngNo ratings yet
- News & Views: Restrictive Fluid Therapy and High-Dose Vitamin C in SepsisDocument2 pagesNews & Views: Restrictive Fluid Therapy and High-Dose Vitamin C in SepsisLAURA ALEJANDRA GONZALEZ MONTOYANo ratings yet
- Ccs InfoDocument13 pagesCcs Info786ss100% (1)