Download as pdf or txt
You might also like
- NBME CMS Forms NotesDocument4 pagesNBME CMS Forms NotesJack Guccione100% (7)
- Common Calls For InternsDocument1 pageCommon Calls For Internstheusuals100% (1)
- Epilepsy Management Plan TemplateDocument2 pagesEpilepsy Management Plan TemplateIPNo ratings yet
- EM Basic - Pocket GuideDocument97 pagesEM Basic - Pocket Guidemainertoo100% (2)
- Word Association PANCEDocument31 pagesWord Association PANCEnevmerka100% (1)
- This Study Resource Was: Assessment & Reasoning Cardiac SystemDocument6 pagesThis Study Resource Was: Assessment & Reasoning Cardiac SystemSharon TanveerNo ratings yet
- ATLSDocument9 pagesATLSAdi Dharmawan100% (7)
- The Radiology Handbook: A Pocket Guide to Medical ImagingFrom EverandThe Radiology Handbook: A Pocket Guide to Medical ImagingRating: 3.5 out of 5 stars3.5/5 (8)
- Septeper 2015 Recall 200 Sba Mrcog Part 1Document49 pagesSepteper 2015 Recall 200 Sba Mrcog Part 1VINOD GUPTA100% (2)
- Grabovoi Numbers For HealingDocument23 pagesGrabovoi Numbers For HealingAna BrunetteNo ratings yet
- Betty Neuman System ModelDocument19 pagesBetty Neuman System ModelLlewro Manlapid100% (1)
- EM Basic Chest Pain: Pet Mac P E T M A CDocument7 pagesEM Basic Chest Pain: Pet Mac P E T M A CAkanksha VermaNo ratings yet
- Acute Care: James Finnie - Senior RotationDocument15 pagesAcute Care: James Finnie - Senior RotationFarhanaNo ratings yet
- Pulmonary Thrombo EmbolismDocument3 pagesPulmonary Thrombo EmbolismTom MallinsonNo ratings yet
- EM Basic-Altered Mental Status (AMS)Document2 pagesEM Basic-Altered Mental Status (AMS)Sara ZareiNo ratings yet
- Inbound 2469239670550275995Document17 pagesInbound 2469239670550275995BALCAC Eloisa Gayle I.No ratings yet
- Anaesthesia ProceduresDocument19 pagesAnaesthesia Proceduresj.duncan123111No ratings yet
- IM ReviewDocument4 pagesIM ReviewPäw YusophNo ratings yet
- Reviewer For DutyDocument4 pagesReviewer For DutyBenedict James BermasNo ratings yet
- Neuro Form 1Document2 pagesNeuro Form 1skylar0% (1)
- Respiratory Paediatrics ExaminationDocument1 pageRespiratory Paediatrics ExaminationRatnahKumar28No ratings yet
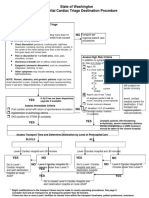
- State of Washington Prehospital Cardiac Triage Destination ProcedureDocument4 pagesState of Washington Prehospital Cardiac Triage Destination ProcedureNanda Dwi Bintoro ZiehenShopNo ratings yet
- NTILS GuideDocument11 pagesNTILS GuideNeil ThomasNo ratings yet
- Assessment of Cvs 2021 Student VersionDocument52 pagesAssessment of Cvs 2021 Student Versionf9qvpqhswrNo ratings yet
- Tetralogy of Fallot - LantiDocument5 pagesTetralogy of Fallot - LantiChristian LantanoNo ratings yet
- Protocol 13: Chest Pain: A&E DoctorDocument4 pagesProtocol 13: Chest Pain: A&E DoctorVanessa HermioneNo ratings yet
- Perfusion, Class 11 ReviewedDocument45 pagesPerfusion, Class 11 ReviewedMelissa GPNo ratings yet
- Merge Live Online Nle Review 2021: Anatomy of The Nle (Nurse Licensure Examination)Document16 pagesMerge Live Online Nle Review 2021: Anatomy of The Nle (Nurse Licensure Examination)Johnmer Avelino100% (1)
- Chest Pain: Sumit Bose, MD PGY-3Document55 pagesChest Pain: Sumit Bose, MD PGY-3Irfan100% (1)
- Sindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Document68 pagesSindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Dafhina Store100% (1)
- Cardio MTB 2:3 Notes DONEDocument10 pagesCardio MTB 2:3 Notes DONESumatt KaurNo ratings yet
- Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument64 pagesDepartemen Kardiologi FK USU RSUP. H. Adam Malik MedanBonitavanyNo ratings yet
- To KnowDocument5 pagesTo KnowDalwadi1No ratings yet
- Cardiopulmonary Ressucitation: Presented by Siwani Rai M.Sc. Nursing-IDocument39 pagesCardiopulmonary Ressucitation: Presented by Siwani Rai M.Sc. Nursing-ISiwani raiNo ratings yet
- Chest Pain Investigation Diagnosis and TreatmentDocument4 pagesChest Pain Investigation Diagnosis and TreatmentHadsabsaNo ratings yet
- Approach To Chest PainDocument52 pagesApproach To Chest PainChris Jardine LiNo ratings yet
- CN 118 - Assessment (Reviewer)Document5 pagesCN 118 - Assessment (Reviewer)Camille SanguyoNo ratings yet
- Pulmonary Embolism - International Emergency Medicine Education ProjectDocument24 pagesPulmonary Embolism - International Emergency Medicine Education ProjectקרוליינהסתםחולםNo ratings yet
- Satjit Bhusri, MD Cardiologist Lenox Hill Hospital: Jeff Chianfagna Rpa-CDocument76 pagesSatjit Bhusri, MD Cardiologist Lenox Hill Hospital: Jeff Chianfagna Rpa-CAjaz JunachNo ratings yet
- Morning Report: Department of Internal MedicineDocument11 pagesMorning Report: Department of Internal MedicineSharly Ayu PuspitaNo ratings yet
- MEGACODEDocument6 pagesMEGACODESafety JNo ratings yet
- NCM 118Document8 pagesNCM 118Zanie CruzNo ratings yet
- Chest Pain - Investigation, Diagnosis and TreatmentDocument5 pagesChest Pain - Investigation, Diagnosis and Treatmentsoumabho paruiNo ratings yet
- Nean Salubre-Ansale, RN: CU, Clinical InstructorDocument23 pagesNean Salubre-Ansale, RN: CU, Clinical InstructorNean Salubre AnsaleNo ratings yet
- Word AssociationDocument27 pagesWord AssociationMilan Kolovrat100% (1)
- (Nelson Hour) The CV System - HX and PEDocument30 pages(Nelson Hour) The CV System - HX and PEJustin Ng SincoNo ratings yet
- IMA Nurse KKV SaifurDocument69 pagesIMA Nurse KKV Saifureva munartyNo ratings yet
- Cardiovascular System: By: Marc Anthony Liao RNDocument59 pagesCardiovascular System: By: Marc Anthony Liao RNloveseeker06No ratings yet
- Chest Pain: LSU Medical Student Clerkship, New Orleans, LADocument56 pagesChest Pain: LSU Medical Student Clerkship, New Orleans, LAGlucose DRglucoseNo ratings yet
- By: DR - Wesam AbdelazizDocument48 pagesBy: DR - Wesam AbdelazizTIRTH GANATRANo ratings yet
- Word AssociationDocument31 pagesWord Associationjr_brewerNo ratings yet
- Arrythmias and Cardiac TumorsDocument30 pagesArrythmias and Cardiac TumorsRabea DiaNo ratings yet
- Back Pain: Group 4Document71 pagesBack Pain: Group 4Cesar Guico Jr.No ratings yet
- NAC Osce NotesDocument34 pagesNAC Osce NotesInAbsentia675% (4)
- Cardiovascular: Stable Angina PectorisDocument2 pagesCardiovascular: Stable Angina PectoriselverineNo ratings yet
- How and When Are Defibrillation and Synchronized Cardioversion Done?Document14 pagesHow and When Are Defibrillation and Synchronized Cardioversion Done?Catherine Dettelbach LakeNo ratings yet
- Reading Reference 3-Approach To Chest PainDocument14 pagesReading Reference 3-Approach To Chest PainVarshini Tamil SelvanNo ratings yet
- Acute Coronary SyndromeDocument36 pagesAcute Coronary SyndromeSiti FatimahNo ratings yet
- UK Medical AbbreviationsDocument5 pagesUK Medical AbbreviationsRNo ratings yet
- Cardiovascular SystemDocument205 pagesCardiovascular Systemizuku midoriyaNo ratings yet
- Chest Pain CBCRDocument7 pagesChest Pain CBCROsuri MapitigamaNo ratings yet
- CVS Case ProformaDocument2 pagesCVS Case ProformaRiyaSingh100% (1)
- Pediatric Cardiovascular System History & ExaminationDocument74 pagesPediatric Cardiovascular System History & Examinationعبدالله Abdullah INo ratings yet
- CLS - Chest Pain ACS 2023Document40 pagesCLS - Chest Pain ACS 2023popaprostu89No ratings yet
- Obgyn ObjectivesDocument4 pagesObgyn ObjectiveshabbouraNo ratings yet
- History Taking For A Patient With SyncopeDocument4 pagesHistory Taking For A Patient With SyncopehabbouraNo ratings yet
- Management of Diabetic IndividualDocument3 pagesManagement of Diabetic IndividualhabbouraNo ratings yet
- ALTERED BOWEL HABITS AND ABDOMINAL PAIN v.2 SIMPLIFIED Med 1Document3 pagesALTERED BOWEL HABITS AND ABDOMINAL PAIN v.2 SIMPLIFIED Med 1habbouraNo ratings yet
- What To Ask:: Infection (LRTI)Document11 pagesWhat To Ask:: Infection (LRTI)habbouraNo ratings yet
- Elderly Patient History TakingDocument5 pagesElderly Patient History TakinghabbouraNo ratings yet
- Prescription Writing - HandoutDocument3 pagesPrescription Writing - HandouthabbouraNo ratings yet
- Udem Paru GEADocument36 pagesUdem Paru GEAAndiBoediartoNo ratings yet
- 10 Health Benefits of Physical Fitness: Reduces The Risk of DiseasesDocument4 pages10 Health Benefits of Physical Fitness: Reduces The Risk of DiseasesEDGAR PALOMANo ratings yet
- Drug Study - Ambroxol, AmpicillinDocument3 pagesDrug Study - Ambroxol, AmpicillinPaul John RutaquioNo ratings yet
- Alzheimer Disease Including Focal Presentations PDFDocument14 pagesAlzheimer Disease Including Focal Presentations PDFpiedrahitasaNo ratings yet
- Spinal Reflex Therapy & Spinal Reflex Analysis: Evidence BasedDocument2 pagesSpinal Reflex Therapy & Spinal Reflex Analysis: Evidence BasedMonikaNo ratings yet
- Navjyoti Suri 84-Herdwick Street Brampton, ON. L6S 6M1 (647) 287 2618Document4 pagesNavjyoti Suri 84-Herdwick Street Brampton, ON. L6S 6M1 (647) 287 2618api-314566363No ratings yet
- (Download PDF) Ketogenic Diet and Metabolic Therapies Expanded Roles in Health and Disease 2Nd Edition Susan A Masino Editor Full Chapter PDFDocument70 pages(Download PDF) Ketogenic Diet and Metabolic Therapies Expanded Roles in Health and Disease 2Nd Edition Susan A Masino Editor Full Chapter PDFnujabneen100% (10)
- Status of Dysphagia After Ischemic StrokeDocument13 pagesStatus of Dysphagia After Ischemic StrokeYi-Sung TsaiNo ratings yet
- Estevan Jimenez Patient Clinical Report ForDocument7 pagesEstevan Jimenez Patient Clinical Report ForIsrael MelloNo ratings yet
- Must-Know Facts About The COVID-19Document7 pagesMust-Know Facts About The COVID-19Yadieli Lismira Vargas del VillarNo ratings yet
- Placenta AccretaDocument5 pagesPlacenta AccretaF3rcitaNo ratings yet
- Schwartz 9th Ed: Chapter Outline: The SpleenDocument22 pagesSchwartz 9th Ed: Chapter Outline: The SpleenKathryn Reunilla100% (1)
- Centers For TherapyDocument2 pagesCenters For TherapyCeline JohnsonNo ratings yet
- Autoanalyzer Dan Manual Menggunakan Amonium Oksalat 1%: Validasi Hasil Pemeriksaan Jumlah Trombosit SecaraDocument4 pagesAutoanalyzer Dan Manual Menggunakan Amonium Oksalat 1%: Validasi Hasil Pemeriksaan Jumlah Trombosit SecaraAnonymous NEsneMqNo ratings yet
- Viral Hepatitis: Kartika Farahdilla Lubna Qatrunada M Ananta WinartoDocument46 pagesViral Hepatitis: Kartika Farahdilla Lubna Qatrunada M Ananta WinartolubnaNo ratings yet
- Types of AnemiaDocument3 pagesTypes of Anemiaflex gyNo ratings yet
- Food PoisoningDocument6 pagesFood PoisoningAby Gift AnnNo ratings yet
- Seminar - Discussion 1Document3 pagesSeminar - Discussion 1api-373572658No ratings yet
- Balido, John Emmanuel A. BSN223/Grp89 Drug Study: 8 G/dayDocument1 pageBalido, John Emmanuel A. BSN223/Grp89 Drug Study: 8 G/dayEmman BalidoNo ratings yet
- Gastroschizis Vs OmfalocelDocument35 pagesGastroschizis Vs OmfalocelElena LicsandruNo ratings yet
- 3 2 1 Code It 6th Edition Green Solutions Manual DOWNLOAD YOUR FILES DownloadDocument131 pages3 2 1 Code It 6th Edition Green Solutions Manual DOWNLOAD YOUR FILES DownloadelizabethNo ratings yet
- Dissolution Specifications For Oral Drug Products (IR, DR, ER) in The USA - A Regulatory PerspectiveDocument6 pagesDissolution Specifications For Oral Drug Products (IR, DR, ER) in The USA - A Regulatory PerspectiveFaisal AbbasNo ratings yet
- CPS Info Dimenhydrinate (Gravol)Document5 pagesCPS Info Dimenhydrinate (Gravol)Ann A.No ratings yet
- Trigeminal NeuralgiaDocument16 pagesTrigeminal NeuralgiaJerry AbleNo ratings yet
- Operation Theater Policies and Procedures ManualDocument33 pagesOperation Theater Policies and Procedures Manualakinrav50% (2)
- Im So Stressed OutDocument2 pagesIm So Stressed OutBrett FieldsNo ratings yet