Download as pdf or txt
You might also like
- Grand Osce ReviewerDocument16 pagesGrand Osce ReviewerBA Ong100% (1)
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- NCP Tissue Perfusion For Pre-EclampsiaDocument2 pagesNCP Tissue Perfusion For Pre-Eclampsiaanreilegarde83% (23)
- 10.7556 Jaoa.2018.177Document2 pages10.7556 Jaoa.2018.177Jihye AhnNo ratings yet
- Piezogenic Pedal PapulesDocument2 pagesPiezogenic Pedal PapulesWalter ChaconNo ratings yet
- Adipose Tissue Remodeling in Lipedema: Adipocyte Death and Concurrent RegenerationDocument6 pagesAdipose Tissue Remodeling in Lipedema: Adipocyte Death and Concurrent RegenerationAlberto Martínez MartínNo ratings yet
- Lower Extremity LymphedemaDocument8 pagesLower Extremity LymphedemaGunduz AgaNo ratings yet
- Ultrastructure of Epidermolysis V. Epidermolysis Simplex LocalisataDocument5 pagesUltrastructure of Epidermolysis V. Epidermolysis Simplex LocalisataJyotirmayeeNo ratings yet
- A Case of Ehlers Danlos Syndrome Associated With Cleft Lip and Palate Okamura 1984Document6 pagesA Case of Ehlers Danlos Syndrome Associated With Cleft Lip and Palate Okamura 1984elmancuernoNo ratings yet
- Morel Lavellee Lession Diagnostic and ManaganementDocument11 pagesMorel Lavellee Lession Diagnostic and ManaganementGuillermo Chacon AcevedoNo ratings yet
- Pushed Elbow: Grace Mafel P. Lucero - BSPT 2020Document4 pagesPushed Elbow: Grace Mafel P. Lucero - BSPT 2020keshNo ratings yet
- 510-Texto Del Artículo-2208-1-10-20100303Document4 pages510-Texto Del Artículo-2208-1-10-20100303Oussama MouhNo ratings yet
- Practice: Lichen AmyloidosisDocument1 pagePractice: Lichen AmyloidosismutmainnahNo ratings yet
- Berk 2012Document17 pagesBerk 2012abdoh hassanNo ratings yet
- Jurnal 1Document16 pagesJurnal 1Faisal Fitrah NasutionNo ratings yet
- 2022 06 Lymphatic Function and Anatomy in Early Stages of LipedemaDocument10 pages2022 06 Lymphatic Function and Anatomy in Early Stages of LipedemaAndreaNo ratings yet
- Sickle Cell AnemiaDocument2 pagesSickle Cell AnemiaDonjeta AbaziNo ratings yet
- 15 Rectal Prolapse - Libre PathologyDocument3 pages15 Rectal Prolapse - Libre PathologyfadoNo ratings yet
- (03241750 - Acta Medica Bulgarica) Klippel-Trenaunay Syndrome Involving Upper Limb and Chest Wall - A Case Report and Review of The LiteratureDocument4 pages(03241750 - Acta Medica Bulgarica) Klippel-Trenaunay Syndrome Involving Upper Limb and Chest Wall - A Case Report and Review of The LiteratureTeodorNo ratings yet
- Lipedema An Inherited Condition 2010Document7 pagesLipedema An Inherited Condition 2010cure lipedema100% (1)
- 16 DDDocument3 pages16 DDOktavia firnandaNo ratings yet
- Rheumatoid Arthritis: InflammatoryDocument6 pagesRheumatoid Arthritis: InflammatoryAlyssa BatasNo ratings yet
- Heritable Collagen Disorders: The Paradigm of The Ehlers-Danlos SyndromeDocument6 pagesHeritable Collagen Disorders: The Paradigm of The Ehlers-Danlos SyndromeMiguel SantosNo ratings yet
- Javt 14 I 2 P 86Document5 pagesJavt 14 I 2 P 86Bhayu RizallinoorNo ratings yet
- Swelling of The Legs and Feet: AetiologyDocument12 pagesSwelling of The Legs and Feet: AetiologyNelly ElizabethNo ratings yet
- De Quervain Tenosynovitis of The WristDocument8 pagesDe Quervain Tenosynovitis of The Wristrani_zNo ratings yet
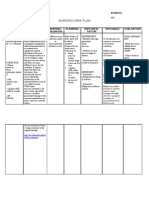
- Nuevo - NCP (Module 1)Document3 pagesNuevo - NCP (Module 1)Nuevo, Kayesha E.No ratings yet
- Charcot Foot - An Update PDFDocument6 pagesCharcot Foot - An Update PDFgamalramadiNo ratings yet
- Mortier 1996Document10 pagesMortier 1996dad dzd adaNo ratings yet
- Antinuclear, Antibodies in A Man. Shoulder Pain, Pleural Effusion, and PositiveDocument4 pagesAntinuclear, Antibodies in A Man. Shoulder Pain, Pleural Effusion, and PositiveandreasgiannNo ratings yet
- Acute Limb IschemicDocument3 pagesAcute Limb IschemicmarisahanaNo ratings yet
- Heritable Collagen Disorders: The Paradigm of The Ehlers-Danlos SyndromeDocument6 pagesHeritable Collagen Disorders: The Paradigm of The Ehlers-Danlos SyndromeAide SeanezNo ratings yet
- Widespread Livedoid VasculopathyDocument4 pagesWidespread Livedoid VasculopathyKata TölgyesiNo ratings yet
- Lichen Striatus On AdultDocument4 pagesLichen Striatus On Adultmustafa566512345No ratings yet
- Connective Tissue FinalsDocument3 pagesConnective Tissue FinalsVon HippoNo ratings yet
- Rare TumorDocument2 pagesRare Tumorannada nambiarNo ratings yet
- Irvine 1996Document3 pagesIrvine 1996Ali AmokraneNo ratings yet
- Ehlers-Danlos Syndrome: Differential Diagnoses & Workup Treatment & Medication Follow-Up MultimediaDocument10 pagesEhlers-Danlos Syndrome: Differential Diagnoses & Workup Treatment & Medication Follow-Up MultimediasravanbrahmaNo ratings yet
- Ortho Exam Offtag Notes Houseman KKM MalaysiaDocument8 pagesOrtho Exam Offtag Notes Houseman KKM MalaysianuurmursyiidahmdNo ratings yet
- Intraosseous Lipomas: Radlologic and Pathologic Manifestations'Document6 pagesIntraosseous Lipomas: Radlologic and Pathologic Manifestations'GeniaaldafitriaasgenNo ratings yet
- Caudal Duplication SyndromeDocument3 pagesCaudal Duplication Syndromekhumaira1982No ratings yet
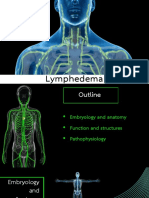
- Lymphedema: Natthaphong Jirojananukul 4 Year Medical Student Phichit Medical CenterDocument26 pagesLymphedema: Natthaphong Jirojananukul 4 Year Medical Student Phichit Medical CenterPuthiput ChotsutaworakulNo ratings yet
- Myelopathy Hand: Two or ThreeDocument5 pagesMyelopathy Hand: Two or ThreereyNo ratings yet
- Linician Pdate: Management of Deep Vein Thrombosis of The Upper ExtremityDocument7 pagesLinician Pdate: Management of Deep Vein Thrombosis of The Upper ExtremityhestyNo ratings yet
- Steatocystoma Multiplex Suppurativa: Case Report of A Rare ConditionDocument3 pagesSteatocystoma Multiplex Suppurativa: Case Report of A Rare ConditionMeteor_SlaveNo ratings yet
- Case Report: Concomitant Gout and Rheumatoid Arthritis - A CaseDocument2 pagesCase Report: Concomitant Gout and Rheumatoid Arthritis - A CasealifNo ratings yet
- Cutis Laxa Syndrome in Siblings FinalDocument4 pagesCutis Laxa Syndrome in Siblings FinalSunil MulgundNo ratings yet
- Chapter 36Document3 pagesChapter 36Samantha QuintoNo ratings yet
- Leg Edema Assessment and ManagementDocument11 pagesLeg Edema Assessment and Managementastraeax pandaNo ratings yet
- Aafp Carpal Tunnel SyndromeDocument7 pagesAafp Carpal Tunnel Syndromehauhau hauraNo ratings yet
- 2.-Midterms_Cardiovascular-DisordersDocument39 pages2.-Midterms_Cardiovascular-DisordersSteph CaronanNo ratings yet
- Warty Dyskeratoma As A Cutaneous Horn of The Mons PubisDocument3 pagesWarty Dyskeratoma As A Cutaneous Horn of The Mons PubisDomenica BourneNo ratings yet
- BreastDocument20 pagesBreastRana WaelNo ratings yet
- Sic Fracture AgainDocument5 pagesSic Fracture AgainEzra Miguel DarundayNo ratings yet
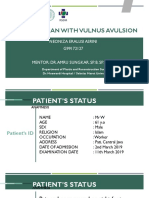
- Preskas Bedah Plastik NeonizaDocument30 pagesPreskas Bedah Plastik NeonizaRaNo ratings yet
- Steatocystoma Multiplex Presenting As Acral Subcutaneous NodulesDocument2 pagesSteatocystoma Multiplex Presenting As Acral Subcutaneous Noduleshendra asusNo ratings yet
- The Treatment of Lymphoedema by Complex Physical Therapy: Original ArticleDocument5 pagesThe Treatment of Lymphoedema by Complex Physical Therapy: Original ArticleVladislav KotovNo ratings yet
- 4 - Peripheral VascularDocument14 pages4 - Peripheral Vascularkyla.navarroNo ratings yet
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)