Download as xlsx, pdf, or txt
You might also like
- Catch-Up Ri Immunization Activity MicroplanDocument1 pageCatch-Up Ri Immunization Activity MicroplanFima JandulNo ratings yet
- Public Health Nursing 8X13Document11 pagesPublic Health Nursing 8X13RUIZ JAKE CANCILLER. VELARDENo ratings yet
- Integrated Essential Maternal and Newborn CareDocument8 pagesIntegrated Essential Maternal and Newborn Carekhatedeleon100% (1)
- Importance of Ethics To The ProfessionDocument9 pagesImportance of Ethics To The ProfessionNin SalvacionNo ratings yet
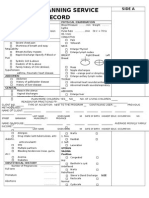
- Family Planning Service RecordDocument3 pagesFamily Planning Service RecordRJay Mon Marcos100% (2)
- Human Resource For Health (HRH) Evaluation 2020: Rural Health Unit Staff Behavioral RatingDocument17 pagesHuman Resource For Health (HRH) Evaluation 2020: Rural Health Unit Staff Behavioral RatingSeriel Tismo100% (1)
- Primary Health Care 2 1232967837997879 3Document42 pagesPrimary Health Care 2 1232967837997879 3JL CalvinNo ratings yet
- Artificial Family Planning Methods Artificial Family Planning MethodsDocument33 pagesArtificial Family Planning Methods Artificial Family Planning MethodsJullienne Ysabelle AngNo ratings yet
- Department of Health ProgramsDocument14 pagesDepartment of Health ProgramsJan Kristel A. QuijanoNo ratings yet
- Immunization: Expanded Program On Immunization (EPI)Document4 pagesImmunization: Expanded Program On Immunization (EPI)3amabelle arevaloNo ratings yet
- Reflection Paper About Philippine Healthcare Delivery SystemDocument2 pagesReflection Paper About Philippine Healthcare Delivery SystemTWINKLE MAE EGAY100% (1)
- HandwashingDocument6 pagesHandwashingKhemz Dalde Lim100% (1)
- Week 1 CoparDocument9 pagesWeek 1 CoparSansaiNo ratings yet
- CP-PHC 1 Removal ExamDocument6 pagesCP-PHC 1 Removal ExamJuana I. Dela Cruz100% (1)
- Pabasa Sa NutrisyonDocument2 pagesPabasa Sa NutrisyonRenita Gacosta CamposanoNo ratings yet
- Executive Order No. 51Document54 pagesExecutive Order No. 51Sheika Caballero IndananNo ratings yet
- Expanded Program On ImmunizationDocument4 pagesExpanded Program On ImmunizationKrizle AdazaNo ratings yet
- I. National Objectives For Health 2005 - 2010 Department of HealthDocument7 pagesI. National Objectives For Health 2005 - 2010 Department of Healthjonalyn badeNo ratings yet
- FHSISDocument14 pagesFHSISSam Raven AndresNo ratings yet
- MNCHNDocument45 pagesMNCHNAnn Margareth Salazar-ManaloNo ratings yet
- Barangay Health Center Services and DOH ProgramsDocument7 pagesBarangay Health Center Services and DOH ProgramsKristil Chavez100% (1)
- 10 Doh Programs: Prepared By: Dhonnalyn A. Caballero, RNDocument28 pages10 Doh Programs: Prepared By: Dhonnalyn A. Caballero, RNAnne Geleen BariasNo ratings yet
- Magna Carta For Public Health WorkersDocument24 pagesMagna Carta For Public Health WorkersMichelle BigcasNo ratings yet
- Phil HealthDocument45 pagesPhil Healthkym anne surmionNo ratings yet
- Community Diagnosis NCM 113 2Document63 pagesCommunity Diagnosis NCM 113 2Jewenson SalvadorNo ratings yet
- Benefits of Family Planning in The PhilippinesDocument6 pagesBenefits of Family Planning in The PhilippinesYaniNo ratings yet
- Ilem - Dispelling Myths, Correcting Misconceptions in Family PlanningDocument21 pagesIlem - Dispelling Myths, Correcting Misconceptions in Family PlanningaishiellcastilloNo ratings yet
- Booklet-Health Centre Simple Guide For Reaching Every PurokDocument38 pagesBooklet-Health Centre Simple Guide For Reaching Every PurokchateNo ratings yet
- Health Care Delivery System Lecture Handout PDFDocument9 pagesHealth Care Delivery System Lecture Handout PDFelle bello100% (1)
- NCM 104 - M6 - DOH Programs Related To Family HealthDocument4 pagesNCM 104 - M6 - DOH Programs Related To Family HealthJollan Marie Buenvenida0% (1)
- Buntis Congress Report 2021Document24 pagesBuntis Congress Report 2021Giselle ArenasNo ratings yet
- Factors Affecting Drug ActionDocument16 pagesFactors Affecting Drug ActionBagya VetriNo ratings yet
- Narrative Report ShadowingDocument18 pagesNarrative Report ShadowingThriska Ravven Resurreccion100% (1)
- PGD NotesDocument22 pagesPGD NotesMae AbabonNo ratings yet
- BHW TRAINING Neonate and Infant HealthDocument24 pagesBHW TRAINING Neonate and Infant HealthWilma BeraldeNo ratings yet
- 3.3 Integrated Management of Childhood Illness PDFDocument11 pages3.3 Integrated Management of Childhood Illness PDFVernonDimalNo ratings yet
- EPI - AND - IMCI - Docx Filename - UTF-8''EPI AND IMCIDocument14 pagesEPI - AND - IMCI - Docx Filename - UTF-8''EPI AND IMCIYvonne Carmel Aguilar SunigaNo ratings yet
- Lecture 1 Family PlanningDocument84 pagesLecture 1 Family PlanningAlfie Adam Ramillano100% (4)
- Partial CHN211 Week 7Document16 pagesPartial CHN211 Week 7Via Kristel ZapantaNo ratings yet
- Micronutrient Program - Department of HealthDocument3 pagesMicronutrient Program - Department of HealthMelvin MarzanNo ratings yet
- DOTS Program For TB: Department of HealthDocument11 pagesDOTS Program For TB: Department of HealthCarissa De Luzuriaga-BalariaNo ratings yet
- The Healthcare Delivery System PDFDocument89 pagesThe Healthcare Delivery System PDFAlex Larraga100% (1)
- DOH ProgramsDocument52 pagesDOH ProgramsAizelle Nicole OrdoñezNo ratings yet
- Nurs 05: Community Health Nursing 1 Community Health Nursing of Individual and Family As ClientDocument23 pagesNurs 05: Community Health Nursing 1 Community Health Nursing of Individual and Family As ClientToyour EternityNo ratings yet
- National Immunization Program: Manual of Procedures Booklet 7Document32 pagesNational Immunization Program: Manual of Procedures Booklet 7Blue PielagoNo ratings yet
- Ra 9288 Basis For Questionnaire PDFDocument22 pagesRa 9288 Basis For Questionnaire PDFHolden Mandapat ValdezNo ratings yet
- Record of Actual Delivery HandledDocument2 pagesRecord of Actual Delivery HandledPatricia Ann Salazar RnNo ratings yet
- Ao2021 0045Document14 pagesAo2021 0045che_c812125No ratings yet
- Learning Guide PHC 2Document20 pagesLearning Guide PHC 2Niña Amato100% (1)
- Prenatal CardDocument2 pagesPrenatal CardMandeep SinghNo ratings yet
- Decent Work AgendaDocument3 pagesDecent Work AgendaSarahFatimaNo ratings yet
- CHN DOH ProgramsDocument158 pagesCHN DOH Programsjudd wilson100% (1)
- Department of Health: Malaria Control ProgramDocument6 pagesDepartment of Health: Malaria Control ProgramTechnoShindoNo ratings yet
- 2 A Healthy CommunityDocument12 pages2 A Healthy CommunityJmarie Brillantes PopiocoNo ratings yet
- Quiz 2Document15 pagesQuiz 2Francis Rafael PadillaNo ratings yet
- Doh Health Programs (Child Program)Document64 pagesDoh Health Programs (Child Program)Wilma Nierva BeraldeNo ratings yet
- Expanded Program On Immunization CHNDocument4 pagesExpanded Program On Immunization CHNgeralynroseNo ratings yet
- Aquino Health AgendaDocument41 pagesAquino Health AgendaJannine Mae Zaragosa MosquisaNo ratings yet
- Dispensing Report 2018 (ComPack)Document2 pagesDispensing Report 2018 (ComPack)NanRe Gacus Yan-OneNo ratings yet
- HPN DM RegistryDocument9 pagesHPN DM RegistryBorbe ClauNo ratings yet
- DOH MAINTENANCE MEDICINES UTILIZATION REPORTDocument7 pagesDOH MAINTENANCE MEDICINES UTILIZATION REPORTaba mojosNo ratings yet
- Front Page Profiling Salvador 2020 UpdatedDocument5 pagesFront Page Profiling Salvador 2020 UpdatedSeriel TismoNo ratings yet
- Family Planning 2020Document70 pagesFamily Planning 2020Seriel TismoNo ratings yet
- Maternal Care 2019Document7 pagesMaternal Care 2019Seriel TismoNo ratings yet
- Section D. Oral Health Care and Services: For The Month OfDocument2 pagesSection D. Oral Health Care and Services: For The Month OfSeriel TismoNo ratings yet
- Section H. Morbidity Diseases ReportDocument5 pagesSection H. Morbidity Diseases ReportSeriel TismoNo ratings yet
- HRH 2018 Report FormsDocument5 pagesHRH 2018 Report FormsSeriel TismoNo ratings yet
- I. Municipal Profile: Service Delivery Network Directory: Province of LeyteDocument2 pagesI. Municipal Profile: Service Delivery Network Directory: Province of LeyteSeriel TismoNo ratings yet
- Morbidity Dse FormDocument3 pagesMorbidity Dse FormSeriel Tismo100% (1)
- A.BHS Canlingga: Total Population: 4,471 No. of Nhts HH: 489 No. of NON-NHTS HH: 780Document2 pagesA.BHS Canlingga: Total Population: 4,471 No. of Nhts HH: 489 No. of NON-NHTS HH: 780Seriel TismoNo ratings yet
- A.BHS Abaca: TOTAL POPULATION: 5135 No. of NHTS HH: 729 No. of NON-NHTS HH: 533Document2 pagesA.BHS Abaca: TOTAL POPULATION: 5135 No. of NHTS HH: 729 No. of NON-NHTS HH: 533Seriel TismoNo ratings yet
- OCTOBER 2018: Nurse Deployment Project (NDP) Monthly AccomplishmentDocument3 pagesOCTOBER 2018: Nurse Deployment Project (NDP) Monthly AccomplishmentSeriel TismoNo ratings yet
- Masterlist 0-59 Children FormDocument1 pageMasterlist 0-59 Children FormSeriel TismoNo ratings yet
- VIII. Pharmacies in Dagami, Leyte: Name of Pharmacy Address Name of Pharmacist Contact Number Open HoursDocument1 pageVIII. Pharmacies in Dagami, Leyte: Name of Pharmacy Address Name of Pharmacist Contact Number Open HoursSeriel TismoNo ratings yet
- PharmaciesDocument1 pagePharmaciesSeriel TismoNo ratings yet
- A. BHS CANSAMADADocument2 pagesA. BHS CANSAMADASeriel TismoNo ratings yet
- A. BHS CANLINGGADocument2 pagesA. BHS CANLINGGASeriel TismoNo ratings yet
- III. Spot Map of The Health Facilities in Dagami, LeyteDocument13 pagesIII. Spot Map of The Health Facilities in Dagami, LeyteSeriel TismoNo ratings yet
- Private Health FacilitiesDocument1 pagePrivate Health FacilitiesSeriel TismoNo ratings yet
- II. Health Facilities in Dagami, Leyte: Name and Distance of THE Nearest Referral Facility (KM)Document2 pagesII. Health Facilities in Dagami, Leyte: Name and Distance of THE Nearest Referral Facility (KM)Seriel TismoNo ratings yet
- Office of The Provincial Governor: Republic of The Philippines Province of Davao OrientalDocument2 pagesOffice of The Provincial Governor: Republic of The Philippines Province of Davao OrientalSeriel TismoNo ratings yet
- Covid - Brgy ResolutionDocument1 pageCovid - Brgy ResolutionSeriel TismoNo ratings yet
- Updates On The Implementation of Health Reforms and The Millennium Development GoalsDocument31 pagesUpdates On The Implementation of Health Reforms and The Millennium Development GoalsSeriel TismoNo ratings yet
- 1.1 Contact TracingDocument20 pages1.1 Contact TracingSeriel TismoNo ratings yet
- dm2020 0186 Interim Guidelines On Operations of Converted P and P Spaces Into TTMF PDFDocument27 pagesdm2020 0186 Interim Guidelines On Operations of Converted P and P Spaces Into TTMF PDFSeriel TismoNo ratings yet
- Zone II, Sogod Southern Leyte 6606 PhilippinesDocument2 pagesZone II, Sogod Southern Leyte 6606 PhilippinesSeriel TismoNo ratings yet
- Republic of The Philippines: Department of Health Eastern Visayas Center For Health DevelopmentDocument13 pagesRepublic of The Philippines: Department of Health Eastern Visayas Center For Health DevelopmentSeriel TismoNo ratings yet
- Clearance Form: - Antonio O. Ida, MD, MPHDocument4 pagesClearance Form: - Antonio O. Ida, MD, MPHSeriel TismoNo ratings yet
- Enrollment Form: Personal InformationDocument3 pagesEnrollment Form: Personal InformationSeriel TismoNo ratings yet
- 12.1 Capdev Synthesis 8122020Document46 pages12.1 Capdev Synthesis 8122020Seriel TismoNo ratings yet
- Defectos Cardiacos Diagnostico PrenatalDocument12 pagesDefectos Cardiacos Diagnostico PrenataldavidNo ratings yet
- Androgel 1% Ciii: (Testosterone Gel)Document4 pagesAndrogel 1% Ciii: (Testosterone Gel)The CedarNo ratings yet
- ASSISTING IN BLOOD TRANSFUSION TransDocument3 pagesASSISTING IN BLOOD TRANSFUSION TransVida RoseNo ratings yet
- Descripcion CodigoDocument90 pagesDescripcion Codigolorena barbaranNo ratings yet
- MOCKBOARD PART 3 Ready To PrintDocument7 pagesMOCKBOARD PART 3 Ready To PrintJayrald CruzadaNo ratings yet
- IDEXX CBC Chem ExplainedDocument38 pagesIDEXX CBC Chem Explainedmmatthew74No ratings yet
- What Is Sunscreen? Tips For Applying Sunscreen Sun SafetyDocument2 pagesWhat Is Sunscreen? Tips For Applying Sunscreen Sun SafetyadmassuNo ratings yet
- MPNST Pleiomorphic MRDocument30 pagesMPNST Pleiomorphic MRBian PutriNo ratings yet
- DefibrillationDocument9 pagesDefibrillationJara Maris Moreno BudionganNo ratings yet
- Iv Drip IsoxilanDocument1 pageIv Drip IsoxilannierbobierNo ratings yet
- BpadDocument27 pagesBpadnikitabhattarai20No ratings yet
- Anti ParkinsonsDocument4 pagesAnti ParkinsonsMichaela BernadasNo ratings yet
- Beat CancerDocument114 pagesBeat CancerGeorge Dragoi100% (9)
- Blood Transfusion GuidelineDocument402 pagesBlood Transfusion GuidelineAdam Razi0% (1)
- Music For Pain Relief - Binaural Beats Instant Download PDFDocument1 pageMusic For Pain Relief - Binaural Beats Instant Download PDFIoannis ManNo ratings yet
- Electrocardiography I C P: N Linical RacticeDocument57 pagesElectrocardiography I C P: N Linical RacticewidyamarisNo ratings yet
- Acute Hepatopancreatic Necrosis DiseaseDocument6 pagesAcute Hepatopancreatic Necrosis DiseaseZulkisam PramudiaNo ratings yet
- Thalidomide AssignmentDocument2 pagesThalidomide AssignmentMorganNo ratings yet
- Erode HopsitalsDocument374 pagesErode Hopsitalsdeva nesanNo ratings yet
- Blood Transfusion TeachingDocument18 pagesBlood Transfusion Teachingapi-277522722No ratings yet
- Nursing Care of Patients With Digestive & Gastrointestinal DisordersDocument29 pagesNursing Care of Patients With Digestive & Gastrointestinal DisordersjoreyneeNo ratings yet
- Makalah Bahasa Inggris (Jantung)Document12 pagesMakalah Bahasa Inggris (Jantung)Nia Mldyni100% (1)
- 1st Internal Assessment Examination. Dept of PhysiologyDocument2 pages1st Internal Assessment Examination. Dept of PhysiologyIshan KalraNo ratings yet
- J Neurol Neurosurg Psychiatry-2000-Newton-433-41Document10 pagesJ Neurol Neurosurg Psychiatry-2000-Newton-433-41Joy SanjayaNo ratings yet
- EFN - PPTX 3Document9 pagesEFN - PPTX 3Suheni Khotimah IndrianiNo ratings yet
- Using Voice Change As An Indicator of Dysphagia A Systematic ReviewDocument13 pagesUsing Voice Change As An Indicator of Dysphagia A Systematic ReviewSandra Liliana Sosa SabogalNo ratings yet
- Cagayan Valley Medical Center Department of RadiologyDocument72 pagesCagayan Valley Medical Center Department of RadiologySofia Kezia Apostol CabaroNo ratings yet
- PDF Clinical Guide To Cardiology 1St Edition Christian Fielder Camm Ebook Full ChapterDocument53 pagesPDF Clinical Guide To Cardiology 1St Edition Christian Fielder Camm Ebook Full Chapternolan.gold619100% (3)
- February 2 0 0 9 1: - THE RotarianDocument16 pagesFebruary 2 0 0 9 1: - THE RotarianjperdigaoNo ratings yet
- Laporan Kegiatan Packing Dan Pengantaran Sampel TCM Ke Puskesmas Temindung TAHUN 2022Document6 pagesLaporan Kegiatan Packing Dan Pengantaran Sampel TCM Ke Puskesmas Temindung TAHUN 2022Leha SabrinaNo ratings yet