Download as pdf or txt
You might also like
- ENACb 1Document166 pagesENACb 1DarrylpnzNo ratings yet
- A Requiem To Mother EarthDocument5 pagesA Requiem To Mother EarthSandra SabuNo ratings yet
- Airport Literature StudyDocument15 pagesAirport Literature StudySoundar Rajan100% (2)
- Infectious Diseases: Ratio of Monocytes To Lymphocytes in Peripheral Blood in Patients Diagnosed With Active TuberculosisDocument7 pagesInfectious Diseases: Ratio of Monocytes To Lymphocytes in Peripheral Blood in Patients Diagnosed With Active TuberculosisMario GintingNo ratings yet
- Research Article Analysis of Cases With Cerebrospinal Fluid Characteristics Similar To Tuberculous MeningitisDocument8 pagesResearch Article Analysis of Cases With Cerebrospinal Fluid Characteristics Similar To Tuberculous MeningitisRivaldy BobihuNo ratings yet
- Chapter IIDocument2 pagesChapter IIDian Abdurrahman MathondangNo ratings yet
- Medip, IJCMPH-7363 ODocument9 pagesMedip, IJCMPH-7363 OMohd Yaseen TippuNo ratings yet
- 1 PBDocument4 pages1 PBAnonymous fL37gV33aNo ratings yet
- Acta Med Iran 2013 51 2 113 118 PDFDocument6 pagesActa Med Iran 2013 51 2 113 118 PDFbreNo ratings yet
- Platelet in DengueDocument5 pagesPlatelet in Denguekarina nilasariNo ratings yet
- Diagnostic Potential Of 16 Kda (Hspx, Α-Crystalline) Antigen For Serodiagnosis Of TuberculosisDocument7 pagesDiagnostic Potential Of 16 Kda (Hspx, Α-Crystalline) Antigen For Serodiagnosis Of TuberculosispouralNo ratings yet
- Seizures in Adults With Bacterial MeningitisDocument9 pagesSeizures in Adults With Bacterial MeningitiselaNo ratings yet
- JR2 IntanDocument7 pagesJR2 IntanCitra DewiNo ratings yet
- MLR Untuk Deteksi TB AktifDocument7 pagesMLR Untuk Deteksi TB AktifDwika AudiyanandaNo ratings yet
- Cryptococcal Infection in Plhiv: Series of 12 Cases at The Laboratory of Mohammed Vi University Hospital of MarrakechDocument6 pagesCryptococcal Infection in Plhiv: Series of 12 Cases at The Laboratory of Mohammed Vi University Hospital of MarrakechIJAR JOURNALNo ratings yet
- Ijccm 26 67 2 2Document4 pagesIjccm 26 67 2 2alfanNo ratings yet
- Neuroasia 2017 22 (1) 015Document9 pagesNeuroasia 2017 22 (1) 015Mazin Al-TahirNo ratings yet
- 2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)Document6 pages2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- A Diagnostic Rule For Tuberculous Meningitis: Rashmi Kumar, S N Singh, Neera KohliDocument4 pagesA Diagnostic Rule For Tuberculous Meningitis: Rashmi Kumar, S N Singh, Neera KohliAri WirantariNo ratings yet
- COHORT - TB MenigealDocument11 pagesCOHORT - TB MenigealYA MAAPNo ratings yet
- 647 3316 2 PBDocument4 pages647 3316 2 PBHabibur RahmanNo ratings yet
- Jurnal AsliDocument8 pagesJurnal AsliDwi PurwantiNo ratings yet
- Diagnostic Value of Cytological and Microbiological Methods in Cryptococcal MeningitisDocument9 pagesDiagnostic Value of Cytological and Microbiological Methods in Cryptococcal MeningitisAngelica Maria Rueda SerranoNo ratings yet
- 72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientDocument7 pages72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientFaras ArinalNo ratings yet
- Pi Is 1201971213002142Document5 pagesPi Is 1201971213002142melisaberlianNo ratings yet
- TuberculosisDocument5 pagesTuberculosislittlecandiesNo ratings yet
- The Diagnostic Value of Neutrophil CD64 in Detection of Sepsis in ChildrenDocument5 pagesThe Diagnostic Value of Neutrophil CD64 in Detection of Sepsis in ChildrenrinaviviaudianaNo ratings yet
- G G Scholar: Pubmed CentralDocument6 pagesG G Scholar: Pubmed CentralIkhsan FebriansyahNo ratings yet
- Appropriate Use of Polymerase Chain ReacDocument5 pagesAppropriate Use of Polymerase Chain ReacCarlos Alberto Martinez FloresNo ratings yet
- Thwaites 2004Document11 pagesThwaites 2004Navisa HaifaNo ratings yet
- Incidence and Outcome of Progressive Multifocal Leukoencephalopathy Over 20 Years of The Swiss HIV Cohort StudyDocument8 pagesIncidence and Outcome of Progressive Multifocal Leukoencephalopathy Over 20 Years of The Swiss HIV Cohort StudyziocorvoNo ratings yet
- Definite (Microbiologically Confirmed) Tuberculous Meningitis: Predictors and Prognostic ImpactDocument7 pagesDefinite (Microbiologically Confirmed) Tuberculous Meningitis: Predictors and Prognostic ImpactAngelica Maria Rueda SerranoNo ratings yet
- 12 OA Evaluation of Febrile Thrombocytopenia CasesDocument5 pages12 OA Evaluation of Febrile Thrombocytopenia CasesVimal NishadNo ratings yet
- Tuberculomas of The Brain With and Without Associated Meningitis: A Cohort of 28 Cases Treated With Anti-Tuberculosis Drugs at A Tertiary Care CentreDocument4 pagesTuberculomas of The Brain With and Without Associated Meningitis: A Cohort of 28 Cases Treated With Anti-Tuberculosis Drugs at A Tertiary Care CentreDestyNo ratings yet
- Al-Azhar Assiut Medical Journal Aamj, Vol 13, No 4, October 2015 Suppl-2Document6 pagesAl-Azhar Assiut Medical Journal Aamj, Vol 13, No 4, October 2015 Suppl-2Vincentius Michael WilliantoNo ratings yet
- 148-Article Text-695-1-10-20180529Document5 pages148-Article Text-695-1-10-20180529fio rentiniNo ratings yet
- Penyakit KawasakiDocument7 pagesPenyakit KawasakiAnonymous kieXEbsGeNo ratings yet
- Autoimmune Causes of Encephalitis Syndrome in Thailand: Prospective Study of 103 PatientsDocument9 pagesAutoimmune Causes of Encephalitis Syndrome in Thailand: Prospective Study of 103 PatientsLily Dian AgungNo ratings yet
- Extrapulmonary Tuberculosis Comparative Analysis of Diagnostic Modalities Used in A Tertiary Healthcare SettingDocument2 pagesExtrapulmonary Tuberculosis Comparative Analysis of Diagnostic Modalities Used in A Tertiary Healthcare SettingBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- 1 s2.0 S1876034117301818 Main PDFDocument5 pages1 s2.0 S1876034117301818 Main PDFdiyanNo ratings yet
- Epilepsia - 2009 - Modi - New Onset Seizures in HIV Seizure Semiology CD4 Counts and Viral LoadsDocument4 pagesEpilepsia - 2009 - Modi - New Onset Seizures in HIV Seizure Semiology CD4 Counts and Viral LoadsBoyke SitompulNo ratings yet
- Neurologic Cytomegalovirus Complications in Patients With Aids: Retrospective Review of 13 Cases and Review of The LiteratureDocument6 pagesNeurologic Cytomegalovirus Complications in Patients With Aids: Retrospective Review of 13 Cases and Review of The LiteratureriskyNo ratings yet
- Monografia MeningitisDocument4 pagesMonografia MeningitisJulian GomezNo ratings yet
- International Journal of Infectious DiseasesDocument6 pagesInternational Journal of Infectious DiseasesQuỳnh Nguyễn Thị NhưNo ratings yet
- Neurological Manifestations of HIV Infection: Mohammed MZ, Venugopal KDocument6 pagesNeurological Manifestations of HIV Infection: Mohammed MZ, Venugopal KSadam Yondaime AriesNo ratings yet
- Brucellosis DCDocument6 pagesBrucellosis DCbrahim brahimNo ratings yet
- Clinical and Radiographic Features of Cryptococcal Neoformans Meningitis-Associated Immune Reconstitution Inflammatory SyndromeDocument7 pagesClinical and Radiographic Features of Cryptococcal Neoformans Meningitis-Associated Immune Reconstitution Inflammatory SyndromeWendi IochNo ratings yet
- Presentation, Etiology, and Outcome of Brain Infections in An Indonesian HospitalDocument15 pagesPresentation, Etiology, and Outcome of Brain Infections in An Indonesian HospitalANISA RIFKA RIDHONo ratings yet
- 32 165 1 PB PDFDocument5 pages32 165 1 PB PDFKennyShelva266No ratings yet
- Sdarticle 8Document6 pagesSdarticle 8Riddhi GandhiNo ratings yet
- Predictors of Spontaneous Bleeding in DengueDocument4 pagesPredictors of Spontaneous Bleeding in DengueSawettachai JaitaNo ratings yet
- Bhat 2016Document6 pagesBhat 2016andrian dwiNo ratings yet
- Encefalitis Por DengueDocument7 pagesEncefalitis Por DengueKev Jose Ruiz RojasNo ratings yet
- Eritema Nodoso y AsociacionesDocument6 pagesEritema Nodoso y AsociacionesGuada SosaNo ratings yet
- JurnalDocument5 pagesJurnalgustina mariantiNo ratings yet
- Central Nervous System Infection Following Allogeneic Hematopoietic Stem Cell TransplantationDocument7 pagesCentral Nervous System Infection Following Allogeneic Hematopoietic Stem Cell Transplantationadilla kusumaNo ratings yet
- 10 Hiperplasia Suprarrenal CongenitaDocument9 pages10 Hiperplasia Suprarrenal CongenitaTchacNo ratings yet
- Autonomic Neuropathy in Patients With HIV: Course, Impact of Disease Stage, and MedicationDocument6 pagesAutonomic Neuropathy in Patients With HIV: Course, Impact of Disease Stage, and MedicationkarinarakhmaNo ratings yet
- Artritis Séptica 27ago2023Document10 pagesArtritis Séptica 27ago2023José Alejandro Rivera JaramilloNo ratings yet
- Clinical Presentation of Acute Bacterial Meningitis Andc.s.f. Analysis of Attending Opdpatients in A Tertiary Care Hospital Kanpur, IndiaDocument6 pagesClinical Presentation of Acute Bacterial Meningitis Andc.s.f. Analysis of Attending Opdpatients in A Tertiary Care Hospital Kanpur, IndiaIJAR JOURNALNo ratings yet
- HIV Hemicorea CNS Histoplasmosis 2016Document3 pagesHIV Hemicorea CNS Histoplasmosis 2016Juan Salazar PajaresNo ratings yet
- Euro J of Neurology - 2022 - Mecklenburg - The Spectrum of Central Nervous System Involvement in Whipple S DiseaseDocument13 pagesEuro J of Neurology - 2022 - Mecklenburg - The Spectrum of Central Nervous System Involvement in Whipple S DiseaseNeuropsi SigloXXINo ratings yet
- Auto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementFrom EverandAuto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementPetros EfthimiouNo ratings yet
- NIH Public Access: Author ManuscriptDocument23 pagesNIH Public Access: Author ManuscriptntnquynhproNo ratings yet
- Immune Reconstitution Inflammatory Syndrome in HIV Infected Late Presenters Starting Integrase Inhibitor Containing Antiretroviral TherapyDocument10 pagesImmune Reconstitution Inflammatory Syndrome in HIV Infected Late Presenters Starting Integrase Inhibitor Containing Antiretroviral TherapyntnquynhproNo ratings yet
- Ni Hms 316844Document15 pagesNi Hms 316844ntnquynhproNo ratings yet
- Approach To Pancytopenia: Moderator - DR Vishal Gupta MD Medicine Presented By-Dr Narendra Singh Resident Doctor 2Document35 pagesApproach To Pancytopenia: Moderator - DR Vishal Gupta MD Medicine Presented By-Dr Narendra Singh Resident Doctor 2ntnquynhproNo ratings yet
- HIV and Immune Reconstitution Inflammatory Syndrome HIV IRISDocument8 pagesHIV and Immune Reconstitution Inflammatory Syndrome HIV IRISntnquynhproNo ratings yet
- Majorarticle: Hiv/AidsDocument8 pagesMajorarticle: Hiv/AidsntnquynhproNo ratings yet
- Cryptococcal Lung DiseaseDocument7 pagesCryptococcal Lung DiseasentnquynhproNo ratings yet
- Cryptococcus Neoformans-Host Interactions Determin PDFDocument21 pagesCryptococcus Neoformans-Host Interactions Determin PDFntnquynhproNo ratings yet
- Research ArticleDocument7 pagesResearch ArticlentnquynhproNo ratings yet
- Mec R2018Document227 pagesMec R2018Kishore Kumar RNo ratings yet
- ManvantaraDocument3 pagesManvantaraafterragnarokNo ratings yet
- Basic Presentation SkillsDocument20 pagesBasic Presentation Skills11Rula SabithaTB100% (1)
- Owner: PT. Baker Hughes User: Cok Gede Reza Description: Modified Safety Pin, Add. Handrail & Add. Anti Slip Step Stair at Pressure Test BayDocument3 pagesOwner: PT. Baker Hughes User: Cok Gede Reza Description: Modified Safety Pin, Add. Handrail & Add. Anti Slip Step Stair at Pressure Test BayMuhammad AlpianNo ratings yet
- Case Study of WapdaDocument34 pagesCase Study of WapdaImran Chaudhry100% (1)
- RPT CasesDocument13 pagesRPT CasesSNLTNo ratings yet
- NT Seq DatabaseDocument4 pagesNT Seq DatabaseDevinder KaurNo ratings yet
- Schiavi Enc Met Page015Document1 pageSchiavi Enc Met Page015Adel AdelNo ratings yet
- BEL PE Question Papers For ECE With Answers - 6 Knowledge AddaDocument14 pagesBEL PE Question Papers For ECE With Answers - 6 Knowledge AddaVishwanand ThombareNo ratings yet
- Tiny Talk 2 Teacher's BookDocument15 pagesTiny Talk 2 Teacher's BookAtena RaeisiNo ratings yet
- Cults and Temples of The Middle World (FG&G)Document77 pagesCults and Temples of The Middle World (FG&G)Paul SavvyNo ratings yet
- PQR As Run SheetDocument2 pagesPQR As Run SheetAhmed ElsharkawNo ratings yet
- 1 s2.0 S0264127522004105 MainDocument11 pages1 s2.0 S0264127522004105 MainAsimov RiyazNo ratings yet
- Chapter 20 Practice TestDocument19 pagesChapter 20 Practice TestCorei'Ana Conrad0% (1)
- 5 25 17 Migraines PowerPointDocument40 pages5 25 17 Migraines PowerPointSaifi AlamNo ratings yet
- Green Building Toward Construction Sustainability: Energy Efficiency With Material and Design AspectsDocument11 pagesGreen Building Toward Construction Sustainability: Energy Efficiency With Material and Design AspectsghchgNo ratings yet
- Industrial RoboticsDocument77 pagesIndustrial RoboticsIslam Fouad100% (4)
- Therapeutic Diet Manual: DIRECTIVE #4311Document27 pagesTherapeutic Diet Manual: DIRECTIVE #4311DuNo ratings yet
- South Africa Hard Copy Lit 2Document20 pagesSouth Africa Hard Copy Lit 2Jennifer Española BernalNo ratings yet
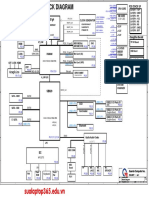
- Da0bl7mb6d0 Rev DDocument44 pagesDa0bl7mb6d0 Rev DFerreira da CunhaNo ratings yet
- Delhi Public School, Greater Noida Pre-Mid Term Exam Class X Mathematics SESSION 2020-21 Set 1 MM: 40 Time: 1.5 Hours InstructionsDocument3 pagesDelhi Public School, Greater Noida Pre-Mid Term Exam Class X Mathematics SESSION 2020-21 Set 1 MM: 40 Time: 1.5 Hours InstructionsAnishikaNo ratings yet
- Stages of SleepDocument2 pagesStages of SleepCamilia Hilmy FaidahNo ratings yet
- HPB21-0457 FINAL Submittal 09-07-2021 - Ritz Sagamore LOIDocument13 pagesHPB21-0457 FINAL Submittal 09-07-2021 - Ritz Sagamore LOIthe next miamiNo ratings yet
- SCM and TQM: by Junaid ShaheedDocument8 pagesSCM and TQM: by Junaid ShaheedjunaidsNo ratings yet
- Law of Mother Earth BoliviaDocument3 pagesLaw of Mother Earth Boliviarahul banerjeeNo ratings yet
- ST200HDocument2 pagesST200HAnjana DissanayakaNo ratings yet
- Directory of SMEs in India-2012 EditionDocument7,115 pagesDirectory of SMEs in India-2012 EditionNilesh RanaNo ratings yet