Download as pdf or txt
You might also like
- Whiteside - Ligament BalancingDocument117 pagesWhiteside - Ligament Balancingrosa_grausNo ratings yet
- Use of Cement in Hip Arthroplasty-Blankstein2020Document9 pagesUse of Cement in Hip Arthroplasty-Blankstein2020Mohan DesaiNo ratings yet
- Unicompartmental Knee ArthroplastyDocument230 pagesUnicompartmental Knee ArthroplastyMohan Desai100% (2)
- Anchorage SeminarDocument14 pagesAnchorage Seminarঅরূপরতনবিশ্বাসNo ratings yet
- Koop Man 2014Document12 pagesKoop Man 2014Elizabeth CominaNo ratings yet
- 33 PDFDocument9 pages33 PDFluis fernando del río espinozaNo ratings yet
- Slight Femoral Under-Correction Versus Neutral Alignment in Total Knee Arthroplasty With Preoperative Varus Knees: A Comparative StudyDocument8 pagesSlight Femoral Under-Correction Versus Neutral Alignment in Total Knee Arthroplasty With Preoperative Varus Knees: A Comparative Studyfebyan yohanesNo ratings yet
- Technology in ArthroplastyDocument10 pagesTechnology in Arthroplastybá anh ngôNo ratings yet
- Bankart VS Tratamiento ConservadorDocument7 pagesBankart VS Tratamiento ConservadorMaría IsabelNo ratings yet
- Art:10.1007/s00402 011 1328 ZDocument10 pagesArt:10.1007/s00402 011 1328 Zbenife8420No ratings yet
- Ligamentizacion HT Grafts After ACLDocument10 pagesLigamentizacion HT Grafts After ACLLuisa MendozaNo ratings yet
- Component Placement Accuracy in Unicompartmental KneeDocument3 pagesComponent Placement Accuracy in Unicompartmental Kneeswastik baratNo ratings yet
- Learning From The Learning Curve in Tota PDFDocument7 pagesLearning From The Learning Curve in Tota PDFcarl marxNo ratings yet
- Active Knee Extension Test Excellent Reliability PDFDocument5 pagesActive Knee Extension Test Excellent Reliability PDFSahithya MNo ratings yet
- Kinematic Analysis of A Six-Degree-Of-Freedom Model Based On ISB Recommendation A Repeatability Analysis and Comparison With Convetional Gait ModelDocument9 pagesKinematic Analysis of A Six-Degree-Of-Freedom Model Based On ISB Recommendation A Repeatability Analysis and Comparison With Convetional Gait ModelLaura VNo ratings yet
- 2023 Steele Et Al Reference Values For Videofluoroscopic Measures of Swallowing An UpdateDocument21 pages2023 Steele Et Al Reference Values For Videofluoroscopic Measures of Swallowing An Updatemackay00917No ratings yet
- A Preclinical Method For Evaluating The Kinematics - 2019 - Medical EngineeringDocument7 pagesA Preclinical Method For Evaluating The Kinematics - 2019 - Medical EngineeringEzgi PelitNo ratings yet
- Kinematic Gait Analysis of Workers Exposed To KneeDocument7 pagesKinematic Gait Analysis of Workers Exposed To KneeSamNo ratings yet
- A Pervasive Sensing Approach To Automatic Assessment of Trunk Coordination Using Mobile DevicesDocument18 pagesA Pervasive Sensing Approach To Automatic Assessment of Trunk Coordination Using Mobile DevicesZilu LiangNo ratings yet
- ACL Tibial Fixation MedthodsDocument8 pagesACL Tibial Fixation MedthodsCleff FlowersNo ratings yet
- Jain 2013Document15 pagesJain 2013Mohan DesaiNo ratings yet
- Os Suportes Externos Melhoram o Equilíbrio Dinâmico em Pacientes Com Instabilidade Crônica Do Tornozelo - Uma Meta-AnáliseDocument19 pagesOs Suportes Externos Melhoram o Equilíbrio Dinâmico em Pacientes Com Instabilidade Crônica Do Tornozelo - Uma Meta-AnáliseThiago Penna ChavesNo ratings yet
- PQ Art 47900-10Document5 pagesPQ Art 47900-10Luan BastosNo ratings yet
- Which Trunk Inclination Directions Best Predict Multidirectional-Seated Limits of Stability Among Individuals With Spinal Cord Injury?Document8 pagesWhich Trunk Inclination Directions Best Predict Multidirectional-Seated Limits of Stability Among Individuals With Spinal Cord Injury?Chanapass DenduangNo ratings yet
- GR Up: SM Orthopedics & Muscular SystemDocument6 pagesGR Up: SM Orthopedics & Muscular SystemValerie BpNo ratings yet
- Pi Is 0883540322007379Document6 pagesPi Is 0883540322007379Debangshu KumarNo ratings yet
- Gait & PostureDocument8 pagesGait & PostureEhrik Javier Huamancaja PalominoNo ratings yet
- Ni Hms 574840Document19 pagesNi Hms 574840felix_the_meowNo ratings yet
- Does Preoperative Diagnosis Impact Patient Outcomes Following Reverse Total Shoulder Arthroplasty? A Systematic ReviewDocument13 pagesDoes Preoperative Diagnosis Impact Patient Outcomes Following Reverse Total Shoulder Arthroplasty? A Systematic ReviewcesarmgaytanmedinaNo ratings yet
- 10 1016@j Arthro 2006 07 006Document8 pages10 1016@j Arthro 2006 07 006YoshitaNo ratings yet
- Allograft Vs Autograft 2022Document11 pagesAllograft Vs Autograft 2022Ahmed MortadaNo ratings yet
- Four Corner Fusion Vs PRCDocument6 pagesFour Corner Fusion Vs PRC79rdhsygngNo ratings yet
- Functional Quadriceps Reconstruction 3D Gait - 2022 - Journal of Plastic ReconDocument14 pagesFunctional Quadriceps Reconstruction 3D Gait - 2022 - Journal of Plastic Recon56xmfwv4pjNo ratings yet
- Jurnal Uts CTDocument10 pagesJurnal Uts CTBUDINo ratings yet
- 3D Motion Reliability of Occipital Condylar Glide Testing From ConceptDocument6 pages3D Motion Reliability of Occipital Condylar Glide Testing From ConceptGustavo Adolfo GarciaNo ratings yet
- Sagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsDocument5 pagesSagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsVizaNo ratings yet
- Is Postural Platform Suited To Study Correlations Between The Masticatory System and Body PostureDocument8 pagesIs Postural Platform Suited To Study Correlations Between The Masticatory System and Body PostureAndreaVanoyMartinNo ratings yet
- Automatic Planning Tools For Lumbar Pedicle Screws PDFDocument14 pagesAutomatic Planning Tools For Lumbar Pedicle Screws PDFThang Tran ThanhNo ratings yet
- Cervical Lordosis in Asymptomatic Individuals: A Meta-AnalysisDocument7 pagesCervical Lordosis in Asymptomatic Individuals: A Meta-Analysismona khosraviNo ratings yet
- Definitions and Consequences oDocument11 pagesDefinitions and Consequences oNova KartikaNo ratings yet
- Implant-Bone Load Transfer Mechanisms in Complete-Arch Prostheses Supported by Four Implants: A Three-Dimensional Finite Element ApproachDocument13 pagesImplant-Bone Load Transfer Mechanisms in Complete-Arch Prostheses Supported by Four Implants: A Three-Dimensional Finite Element ApproachMR GOKCHENNo ratings yet
- Hook Plate Fixation For Acute Unstable Distal Clavicle Fracture: A Systematic Review and Meta-AnalysisDocument6 pagesHook Plate Fixation For Acute Unstable Distal Clavicle Fracture: A Systematic Review and Meta-AnalysisFillipe AgraNo ratings yet
- 2018 Selflearningcomputers LafageDocument7 pages2018 Selflearningcomputers LafageShweta ShirsatNo ratings yet
- Total Knee Replacement Modifies The Preoperative Tibial Torsion Angle - Similar Results Between Computer-Assisted and Standard TechniqueDocument9 pagesTotal Knee Replacement Modifies The Preoperative Tibial Torsion Angle - Similar Results Between Computer-Assisted and Standard TechniqueJoko TriwardonoNo ratings yet
- Gaitan 1 PDFDocument12 pagesGaitan 1 PDFDeborah SalinasNo ratings yet
- Is Reconstruction The Best Management Strategy For Anterior CruciateDocument9 pagesIs Reconstruction The Best Management Strategy For Anterior CruciateItai IzhakNo ratings yet
- Physical Therapy in Sport: Gulcan Harput, Hande Guney-Deniz, John Nyland, Yavuz KocabeyDocument10 pagesPhysical Therapy in Sport: Gulcan Harput, Hande Guney-Deniz, John Nyland, Yavuz KocabeyNaara LibNo ratings yet
- 1 s2.0 S1877065718300915 Main PDFDocument1 page1 s2.0 S1877065718300915 Main PDFKasra AlborziNo ratings yet
- Art - Equilibrio y PropiocepcionDocument7 pagesArt - Equilibrio y PropiocepcionYuLyChNo ratings yet
- Management Thoracic Pain 2019Document9 pagesManagement Thoracic Pain 2019Lotte WeggemanNo ratings yet
- The Journal of ArthroplastyDocument8 pagesThe Journal of Arthroplasty阿欧有怪兽No ratings yet
- SRM Orbital reconDocument14 pagesSRM Orbital reconMGM Oral SurgeryNo ratings yet
- Prótese No JoelhoDocument17 pagesPrótese No JoelhoPaula SampaioNo ratings yet
- Acl PDFDocument11 pagesAcl PDFDaniela CasabonaNo ratings yet
- 1 s2.0 S0021929015001931 MainDocument7 pages1 s2.0 S0021929015001931 MainceliaNo ratings yet
- Nr9 Reliabil AdvPhys 2004Document12 pagesNr9 Reliabil AdvPhys 2004Cleber PimentaNo ratings yet
- Gait & Posture: Erik A. Wikstrom, Kimberly A. Fournier, Patrick O. MckeonDocument5 pagesGait & Posture: Erik A. Wikstrom, Kimberly A. Fournier, Patrick O. MckeonMonikaNo ratings yet
- 1 s2.0 S2468294221000605 MainDocument7 pages1 s2.0 S2468294221000605 MainVishal BasuNo ratings yet
- Evaluation of Tilt-Correction of Anteversion On Anteroposterior Pelvic Radiographs in Total Hip ArthroplastyDocument12 pagesEvaluation of Tilt-Correction of Anteversion On Anteroposterior Pelvic Radiographs in Total Hip ArthroplastytripodegrandeNo ratings yet
- 3 - Lie 2022 Systematic Review and Metaanalysis Graftless Sinus ElevationDocument11 pages3 - Lie 2022 Systematic Review and Metaanalysis Graftless Sinus ElevationLamis MagdyNo ratings yet
- The Accuracy of Digital Templating in Uncemented Total Hip ArthroplastyDocument6 pagesThe Accuracy of Digital Templating in Uncemented Total Hip Arthroplastyson leNo ratings yet
- Fang WH. US Guided Knee Injections More Accurate Blind Inject. Review Randomized Controlled TrialsDocument11 pagesFang WH. US Guided Knee Injections More Accurate Blind Inject. Review Randomized Controlled TrialsJavier MartinNo ratings yet
- Gait & Posture: Full Length ArticleDocument7 pagesGait & Posture: Full Length ArticleMKNo ratings yet
- The SAGES Manual of Colorectal SurgeryFrom EverandThe SAGES Manual of Colorectal SurgeryPatricia SyllaNo ratings yet
- Coronal Alignment Knee ReviewDocument8 pagesCoronal Alignment Knee ReviewMohan DesaiNo ratings yet
- Coronal Alignment - Historical Review, Future DirectionDocument6 pagesCoronal Alignment - Historical Review, Future DirectionMohan DesaiNo ratings yet
- Robotic Alignment of KneeDocument8 pagesRobotic Alignment of KneeMohan DesaiNo ratings yet
- ABS 21685 LondheDocument13 pagesABS 21685 LondheMohan DesaiNo ratings yet
- MOM hypersensitivity-2058-5241-EOR-22-0036Document14 pagesMOM hypersensitivity-2058-5241-EOR-22-0036Mohan DesaiNo ratings yet
- Learning Curve & Time Taken For The Robotic KneeDocument5 pagesLearning Curve & Time Taken For The Robotic KneeMohan DesaiNo ratings yet
- ABS 22461 AkagawaDocument13 pagesABS 22461 AkagawaMohan DesaiNo ratings yet
- Jaaos D 1Document10 pagesJaaos D 1Mohan DesaiNo ratings yet
- Metaanalysis Distal End Radius Volar Plate Vs Conservative2058 5241 EOR 22 0022Document9 pagesMetaanalysis Distal End Radius Volar Plate Vs Conservative2058 5241 EOR 22 0022Mohan DesaiNo ratings yet
- Jain 2013Document15 pagesJain 2013Mohan DesaiNo ratings yet
- Hospital Administratin Control RoomDocument9 pagesHospital Administratin Control RoomMohan DesaiNo ratings yet
- Reconstruction Options and Outcomes For Acetabular Bone Loss in Revision Hip ArthroplastyDocument7 pagesReconstruction Options and Outcomes For Acetabular Bone Loss in Revision Hip ArthroplastyMohan DesaiNo ratings yet
- WHO UHL IHS IPC 2023.2 EngDocument7 pagesWHO UHL IHS IPC 2023.2 EngMohan DesaiNo ratings yet
- Acetabular Column Screws 2014Document7 pagesAcetabular Column Screws 2014Mohan DesaiNo ratings yet
- Medical Students Perceptions of Their Development of Soft Skills Part II The Development of Soft Skills Through Guiding and GrowingDocument6 pagesMedical Students Perceptions of Their Development of Soft Skills Part II The Development of Soft Skills Through Guiding and GrowingMohan DesaiNo ratings yet
- Bone Specific Alkaline PhophataseDocument6 pagesBone Specific Alkaline PhophataseMohan DesaiNo ratings yet
- What Are Soft Skills?Document1 pageWhat Are Soft Skills?Mohan DesaiNo ratings yet
- COVID 19 & Orthopedic Related Articles Till April 2021 Pgs 118Document119 pagesCOVID 19 & Orthopedic Related Articles Till April 2021 Pgs 118Mohan DesaiNo ratings yet
- Lean Thinking - WikipediaDocument1 pageLean Thinking - WikipediaMohan DesaiNo ratings yet
- Recent Review Articles On Osteomalacia From Different Journals 25Document68 pagesRecent Review Articles On Osteomalacia From Different Journals 25Mohan DesaiNo ratings yet
- Reverse Shoulder Arthroplasty: How To Manage Failure: April 2018Document13 pagesReverse Shoulder Arthroplasty: How To Manage Failure: April 2018Mohan DesaiNo ratings yet
- Mechanical Complications and Fractures After Reverse Shoulder Arthroplasty Related To Different Design Types and Their Rates: Part IDocument12 pagesMechanical Complications and Fractures After Reverse Shoulder Arthroplasty Related To Different Design Types and Their Rates: Part IMohan DesaiNo ratings yet
- Abdullah AlNuaim-2Document36 pagesAbdullah AlNuaim-2Mohan DesaiNo ratings yet
- DePuy Trephine ReamersDocument7 pagesDePuy Trephine ReamersMohan DesaiNo ratings yet
- Brief Review: Theory and Practice of Minimal Fresh Gas Flow AnesthesiaDocument13 pagesBrief Review: Theory and Practice of Minimal Fresh Gas Flow AnesthesiaMohan DesaiNo ratings yet
- Surface and Human Anatomy NotesDocument9 pagesSurface and Human Anatomy NotesCharisa Antonette HuelvaNo ratings yet
- BNYS SyllabusDocument260 pagesBNYS SyllabusBalagovind T PNo ratings yet
- Swimming For All - Swimming For Life ManualDocument24 pagesSwimming For All - Swimming For Life ManualVasudeva Singh DubeyNo ratings yet
- The Pelvic Lift: Theme and Variations: Mary BondDocument6 pagesThe Pelvic Lift: Theme and Variations: Mary Bondbackch9011No ratings yet
- Physical ExaminationDocument39 pagesPhysical ExaminationprashanthNo ratings yet
- Ratcliffe 1976. A Revision of The Genus Strategus DynastinaeDocument115 pagesRatcliffe 1976. A Revision of The Genus Strategus Dynastinaesebastian ferrerNo ratings yet
- Phylogenetic and Biogeographic Analysis of The Neotropical Annual Fish Genus Simpsonichthys (Cyprinodontiformes: Rivulidae)Document12 pagesPhylogenetic and Biogeographic Analysis of The Neotropical Annual Fish Genus Simpsonichthys (Cyprinodontiformes: Rivulidae)Felipe BuenoNo ratings yet
- Mnemonics For Medical PGEntranceDocument145 pagesMnemonics For Medical PGEntranceCharan RebelNo ratings yet
- Kiut BMS 2.1 IntroDocument39 pagesKiut BMS 2.1 IntroAbdulyNo ratings yet
- Journal of Orthopaedic Surgery and ResearchDocument6 pagesJournal of Orthopaedic Surgery and ResearchDewye SartikaNo ratings yet
- Neuroscience For Neurosurgeons (Feb 29, 2024) - (110883146X) - (Cambridge University Press) 1st Edition Farhana AkterDocument70 pagesNeuroscience For Neurosurgeons (Feb 29, 2024) - (110883146X) - (Cambridge University Press) 1st Edition Farhana Akterwillie.keith106100% (8)
- Removable Denture Prosthetics - Technical Protocol PDFDocument42 pagesRemovable Denture Prosthetics - Technical Protocol PDFDaniel DidiNo ratings yet
- Ankle: FracturesDocument87 pagesAnkle: FracturesrifkialbanaNo ratings yet
- Jurnal Sendi Dan Macam JointDocument13 pagesJurnal Sendi Dan Macam JointN Nur AriniNo ratings yet
- 11rhinoplasty SurgicalAnatomyDocument49 pages11rhinoplasty SurgicalAnatomySanooj SeyedNo ratings yet
- Ankle Lateral Ligaments LFTC ComplexDocument11 pagesAnkle Lateral Ligaments LFTC ComplexRaymond WinNo ratings yet
- Anatomy Past Paper QuestionsDocument8 pagesAnatomy Past Paper QuestionsSheraz JanjuaNo ratings yet
- Ficha para Inventario de HuesosDocument24 pagesFicha para Inventario de HuesosAntony CevallosNo ratings yet
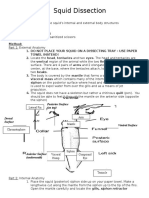
- Squid DissectionDocument3 pagesSquid Dissectionapi-297841438100% (1)
- Venous and Lymphatic Drainage of The Lower LimbDocument26 pagesVenous and Lymphatic Drainage of The Lower LimbEmmanuel IshiomaNo ratings yet
- Anatomy PenisDocument7 pagesAnatomy PenisalexNo ratings yet
- Week 01 - General AnatomyDocument17 pagesWeek 01 - General AnatomyTamene TekileNo ratings yet
- Barouk Countersink Screw From Biomet PDFDocument36 pagesBarouk Countersink Screw From Biomet PDFJacob DoughertyNo ratings yet
- Taxonomic Revision of The Genus CrassicrusDocument32 pagesTaxonomic Revision of The Genus CrassicrusJosé Arturo S. TéllezNo ratings yet
- Patterns of Premature Physeal Arrest:: MR Imaging of 111 ChildrenDocument6 pagesPatterns of Premature Physeal Arrest:: MR Imaging of 111 Childrenjose pablo reyes ortizNo ratings yet
- 2014 @radiologylib William E Morgan Spinal MRI For MusculoskeletalDocument117 pages2014 @radiologylib William E Morgan Spinal MRI For MusculoskeletalkinexNo ratings yet
- Pautas Anatómicas para La Inserción de Minitornillos: Sitios PalatinosDocument11 pagesPautas Anatómicas para La Inserción de Minitornillos: Sitios PalatinosValery V JaureguiNo ratings yet
- Anatomical PositionsDocument18 pagesAnatomical PositionsAnji JoguilonNo ratings yet