Download as pdf or txt
You might also like
- Detailed Lesson Plan in English IV - COMPOUND SENTENCEDocument12 pagesDetailed Lesson Plan in English IV - COMPOUND SENTENCEMadhie Gre Dela Provi94% (16)
- Astm C 423Document12 pagesAstm C 423Abhinav AcharyaNo ratings yet
- Environmental Impact Assessment ModuleDocument39 pagesEnvironmental Impact Assessment ModuleJoshua Landoy100% (2)
- Part 11 Metal Detector Manual PDFDocument24 pagesPart 11 Metal Detector Manual PDFOrlando Melipillan100% (1)
- Simulation-Based Training in EchocardiographyDocument5 pagesSimulation-Based Training in EchocardiographyCristianaBgdnNo ratings yet
- Guidelines For Perioperative Care in Esophagectomy Enhanced Recovery After Surgery (ERAS®) Society Recommendations.Document32 pagesGuidelines For Perioperative Care in Esophagectomy Enhanced Recovery After Surgery (ERAS®) Society Recommendations.FlorNo ratings yet
- Manejo Da Disfagia X Ausculta Cervical - Confiabilidade e Validade Comparando Com Fees 2023Document10 pagesManejo Da Disfagia X Ausculta Cervical - Confiabilidade e Validade Comparando Com Fees 2023anarafaNo ratings yet
- Artigo Set 2023Document12 pagesArtigo Set 2023Sofia Adão da FonsecaNo ratings yet
- Jurnal 8 RadiologiiiiDocument10 pagesJurnal 8 RadiologiiiiEvan SilalahiNo ratings yet
- 8894 Jacobs2017Document11 pages8894 Jacobs2017Fahrizal Al-fatihNo ratings yet
- V82no1 - 4 DREDocument2 pagesV82no1 - 4 DREJohnSmithNo ratings yet
- Sistematización de Un Programa de Entrenamiento en Endoscopía Digestiva Alta Diagnóstica en Ambiente Simulado y Curvas de Aprendizaje en Pacientes Reales.Document6 pagesSistematización de Un Programa de Entrenamiento en Endoscopía Digestiva Alta Diagnóstica en Ambiente Simulado y Curvas de Aprendizaje en Pacientes Reales.David Schnettler RodriguezNo ratings yet
- Proactive Medicine: The "UCI 30," An Ultrasound-Based Clinical Initiative From The University of California, IrvineDocument6 pagesProactive Medicine: The "UCI 30," An Ultrasound-Based Clinical Initiative From The University of California, Irvineelectron_glowNo ratings yet
- Radiotherapy Quality Assurance in The PORTEC 3 TROG 08 - 2021 - Clinical OncolDocument7 pagesRadiotherapy Quality Assurance in The PORTEC 3 TROG 08 - 2021 - Clinical OncolAns BarrungNo ratings yet
- Synopsis FinalDocument10 pagesSynopsis FinalGEORGE HONNALLINo ratings yet
- Article Print 4772Document9 pagesArticle Print 4772Hidayatun NazzaNo ratings yet
- Guidance and Standards For Breast Cancer Care in EDocument7 pagesGuidance and Standards For Breast Cancer Care in ECristina BadeaNo ratings yet
- 2guia en EmbarazoDocument13 pages2guia en EmbarazoCecilia Quispe JaureguiNo ratings yet
- EUR 16261 Quality Criteria PaediatricsDocument71 pagesEUR 16261 Quality Criteria PaediatricsCamila De Mello BuzzattoNo ratings yet
- 1 s2.0 S1078817417301360 MainDocument6 pages1 s2.0 S1078817417301360 MainTitinNo ratings yet
- Kang2015 KimDocument14 pagesKang2015 KimIkram LyaNo ratings yet
- Does The Number of Operating Specialists Influence The Conversion Rate and Outcomes After Laparoscopic Colorectal Cancer Surgery?Document7 pagesDoes The Number of Operating Specialists Influence The Conversion Rate and Outcomes After Laparoscopic Colorectal Cancer Surgery?Yassine BahrNo ratings yet
- Novices May Be Trained To Screen For Abdominal Aortic Aneurysms Using Ultrasound. Cardiovasc UltrasoundDocument8 pagesNovices May Be Trained To Screen For Abdominal Aortic Aneurysms Using Ultrasound. Cardiovasc UltrasoundesmoesNo ratings yet
- Endoscopic Skills Training in A Simulated Clinical.8Document6 pagesEndoscopic Skills Training in A Simulated Clinical.8Alberto Kenyo Riofrio PalaciosNo ratings yet
- Coursebook-Echoscopy ch30Document23 pagesCoursebook-Echoscopy ch30Сергей СадовниковNo ratings yet
- Training in Clinical RadiologyDocument12 pagesTraining in Clinical RadiologyAnoop TitusNo ratings yet
- 070.2017.DesJardin - Near Peer Point of CareUltrasoundDocument9 pages070.2017.DesJardin - Near Peer Point of CareUltrasoundSergio San Juan DertkigilNo ratings yet
- Pathways To EndosDocument3 pagesPathways To EndosMustafa Ismael NayyefNo ratings yet
- Ketelaars2018 Article ABCDEOfPrehospitalUltrasonograDocument18 pagesKetelaars2018 Article ABCDEOfPrehospitalUltrasonograPedito PicapiedraNo ratings yet
- Zastita Od Jonizirajuceg Zracenja-Ful Tekst-94-101Document8 pagesZastita Od Jonizirajuceg Zracenja-Ful Tekst-94-101Meris JugadorNo ratings yet
- Cardoso 2014Document18 pagesCardoso 2014Cristina ViaplanaNo ratings yet
- Surgeon-Performed Ultrasound As A Diagnostic Tool in AppendicitisDocument6 pagesSurgeon-Performed Ultrasound As A Diagnostic Tool in Appendicitisansar ahmedNo ratings yet
- Validation of Instruments For The Assessment of Dysphagia Due To Malignancy of The EsophagusDocument8 pagesValidation of Instruments For The Assessment of Dysphagia Due To Malignancy of The EsophagusLarissa MeloNo ratings yet
- Zaborowski - A Systematic Review of Oncological Outcomes After Nipple SparingDocument8 pagesZaborowski - A Systematic Review of Oncological Outcomes After Nipple SparinglucenaxNo ratings yet
- 2012 Quality in Screening Colonoscopy Position Statement PDFDocument12 pages2012 Quality in Screening Colonoscopy Position Statement PDFMadalina StoicescuNo ratings yet
- Comprehensive Geriatric Assessment (Article) - 1Document10 pagesComprehensive Geriatric Assessment (Article) - 1porkodimptNo ratings yet
- Laparoscopic Versus Open Pediatric Inguinal Hernia RepairDocument15 pagesLaparoscopic Versus Open Pediatric Inguinal Hernia Repairmelon segerNo ratings yet
- Module 1: Basic: Early Pregnancy (8 - 12 Weeks) UltrasoundDocument7 pagesModule 1: Basic: Early Pregnancy (8 - 12 Weeks) UltrasoundpuspaNo ratings yet
- Complications of ColonosDocument19 pagesComplications of ColonosFanny PritaningrumNo ratings yet
- Four Risk of Malignancy Indices in Evaluation of Pelvic MassesDocument8 pagesFour Risk of Malignancy Indices in Evaluation of Pelvic MassesherryNo ratings yet
- 3 PDFDocument7 pages3 PDFAhmad SutriNo ratings yet
- Summative Assessments Are More Powerful Drivers of Student Learning Than Resource Intensive Teaching FormatsDocument10 pagesSummative Assessments Are More Powerful Drivers of Student Learning Than Resource Intensive Teaching FormatsMega ArfiyantiNo ratings yet
- 1 s2.0 S0167814013003393 MainDocument6 pages1 s2.0 S0167814013003393 MainAlix DuboisNo ratings yet
- Lectura 3 - Algoritmo de Movilización Temprana.Document18 pagesLectura 3 - Algoritmo de Movilización Temprana.PilarSolanoPalominoNo ratings yet
- ESGO PG Ovarian Cancer Surgery A6 V04 PressDocument16 pagesESGO PG Ovarian Cancer Surgery A6 V04 Press9dc4zvr5vcNo ratings yet
- PARS Reader's Digest - Apr 2013Document12 pagesPARS Reader's Digest - Apr 2013info8673No ratings yet
- Diagnostic Delay MoroccoDocument5 pagesDiagnostic Delay MoroccoOmaima ElyounsiNo ratings yet
- 19Document11 pages19呂宜家No ratings yet
- Local Validation of An Anastomosis Leakage Score Niklas Holmlov 2020Document13 pagesLocal Validation of An Anastomosis Leakage Score Niklas Holmlov 2020drelvNo ratings yet
- Obstetric and Gynecologic Ultrasound Curriculum and Competency Assessment in Residency Training Programs: Consensus ReportDocument39 pagesObstetric and Gynecologic Ultrasound Curriculum and Competency Assessment in Residency Training Programs: Consensus ReportOngky AristianNo ratings yet
- Ladegaardbaun 2021Document11 pagesLadegaardbaun 2021andianto.indrawanNo ratings yet
- Sagesorg-Guidelines For The Use of Laparoscopy During PregnancyDocument32 pagesSagesorg-Guidelines For The Use of Laparoscopy During PregnancyLuis Acosta CumberbatchNo ratings yet
- Curriculum For MPDocument11 pagesCurriculum For MPGezim HodolliNo ratings yet
- Acr Practice Parameter For The Performance of Fluoroscopic Contrast Enema Examination in AdultsDocument8 pagesAcr Practice Parameter For The Performance of Fluoroscopic Contrast Enema Examination in AdultsHercules RianiNo ratings yet
- Preeclampsia Diagnosis and Treatment OptionsDocument14 pagesPreeclampsia Diagnosis and Treatment OptionsPanji Agung KhrisnaNo ratings yet
- Abc3 EsmoDocument18 pagesAbc3 EsmoGerson Mejia ViaNo ratings yet
- Wiles2017 Article ManagementAndFollow-upOfGallblDocument11 pagesWiles2017 Article ManagementAndFollow-upOfGallblTrần Quốc KhánhNo ratings yet
- Efficacy of An Ultrasound Trai PDFDocument15 pagesEfficacy of An Ultrasound Trai PDFAnida IzzNo ratings yet
- Chatoor Organising A Clinical Service For Patients With Pelvic Floor DisordersDocument10 pagesChatoor Organising A Clinical Service For Patients With Pelvic Floor DisordersDavion StewartNo ratings yet
- Early Predictors For Intubation-Surfactant-Extubation Failure in Preterm Infants With Neonatal Respiratory Distress Syndrome: A Systematic ReviewDocument13 pagesEarly Predictors For Intubation-Surfactant-Extubation Failure in Preterm Infants With Neonatal Respiratory Distress Syndrome: A Systematic ReviewPhilipe VieiraNo ratings yet
- Strength and Endurance Training in The Treatment of Lung Cancer Patients in Stages IIIA-IIIB-IVDocument7 pagesStrength and Endurance Training in The Treatment of Lung Cancer Patients in Stages IIIA-IIIB-IVFRANCISCO JAVIER TABILO SAEZNo ratings yet
- Multiparametric Ultrasound Diagnosis of Breast DiseasesFrom EverandMultiparametric Ultrasound Diagnosis of Breast DiseasesGennady T. SukhikhNo ratings yet
- Lee 2004Document15 pagesLee 2004Inryuu ZenNo ratings yet
- Jurnal 4 122Document5 pagesJurnal 4 122Inryuu ZenNo ratings yet
- Jurnal 2 (2019)Document11 pagesJurnal 2 (2019)Inryuu ZenNo ratings yet
- JMSCR Vol - 07 - Issue - 06 - Page 33-38 - JuneDocument6 pagesJMSCR Vol - 07 - Issue - 06 - Page 33-38 - JuneInryuu ZenNo ratings yet
- Case Report: Psoriasis Vulgaris in Children - Case PresentationDocument5 pagesCase Report: Psoriasis Vulgaris in Children - Case PresentationInryuu ZenNo ratings yet
- Jurnal 1 (2020)Document10 pagesJurnal 1 (2020)Inryuu ZenNo ratings yet
- Paederus Dermatitis: Environmental Risk Factors, Clinical Features, and ManagementDocument7 pagesPaederus Dermatitis: Environmental Risk Factors, Clinical Features, and ManagementInryuu ZenNo ratings yet
- Co Existence of Juvenile Dermatomyositis and Psoriasis Vulgaris With Fungal Infection: A Case Report and Literature ReviewDocument4 pagesCo Existence of Juvenile Dermatomyositis and Psoriasis Vulgaris With Fungal Infection: A Case Report and Literature ReviewInryuu ZenNo ratings yet
- Abdominal Ultrasound For Pediatric Blunt Trauma FAST Is Not Always BetterDocument3 pagesAbdominal Ultrasound For Pediatric Blunt Trauma FAST Is Not Always BetterInryuu ZenNo ratings yet
- Abdominal Ultrasound Findings of Tumor-Forming Hepatic Malignant LymphomaDocument8 pagesAbdominal Ultrasound Findings of Tumor-Forming Hepatic Malignant LymphomaInryuu ZenNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundInryuu ZenNo ratings yet
- APA-AP - Activity 3-Emerging Ethical and Policy Issues of STSDocument36 pagesAPA-AP - Activity 3-Emerging Ethical and Policy Issues of STSJOHN MARTIN APA-APNo ratings yet
- Naamlp 2002 ProceedDocument578 pagesNaamlp 2002 ProceedRussell HartillNo ratings yet
- A 182Document20 pagesA 182Thomas100% (1)
- Teachers' Interview PDFDocument38 pagesTeachers' Interview PDFlalitNo ratings yet
- Andrea Kaneb - Group - 15Document4 pagesAndrea Kaneb - Group - 15Sibi KrishnaNo ratings yet
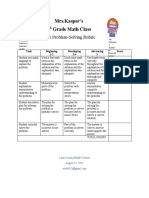
- Problemsolving RubricDocument1 pageProblemsolving Rubricapi-560491685No ratings yet
- Eastron Electronic Co., LTDDocument2 pagesEastron Electronic Co., LTDasd qweNo ratings yet
- LG+47ln5700 47ln570t 47ln570y 47ln5710 Chassis lb33bDocument119 pagesLG+47ln5700 47ln570t 47ln570y 47ln5710 Chassis lb33bmidominguez0% (1)
- Peptides and Proteins: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument30 pagesPeptides and Proteins: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Lec 1 Introduction Slides 1 20 MergedDocument153 pagesLec 1 Introduction Slides 1 20 MergedNeeraj VarmaNo ratings yet
- Permanent Magnet GuidelineDocument32 pagesPermanent Magnet GuidelineJaime FalaganNo ratings yet
- ESSAYDocument7 pagesESSAYKaren OliveraNo ratings yet
- Toward The Efficient Impact Frontier: FeaturesDocument6 pagesToward The Efficient Impact Frontier: Featuresguramios chukhrukidzeNo ratings yet
- Informe Sobre El Manejo de CostasDocument88 pagesInforme Sobre El Manejo de CostasMetro Puerto RicoNo ratings yet
- Decision Trees and Boosting: Helge Voss (MPI-K, Heidelberg) TMVA WorkshopDocument30 pagesDecision Trees and Boosting: Helge Voss (MPI-K, Heidelberg) TMVA WorkshopAshish TiwariNo ratings yet
- Indias Gold Market Reform and GrowthDocument149 pagesIndias Gold Market Reform and GrowthtmeygmvzjfnkqcwhgpNo ratings yet
- Muhammad Fauzi-855677765-Fizz Hotel Lombok-HOTEL - STANDALONEDocument1 pageMuhammad Fauzi-855677765-Fizz Hotel Lombok-HOTEL - STANDALONEMuhammad Fauzi AndriansyahNo ratings yet
- BlueStack Platform Marketing PlanDocument10 pagesBlueStack Platform Marketing PlanFıratcan KütükNo ratings yet
- Alarm Security Pic - Google ShoppingDocument1 pageAlarm Security Pic - Google Shoppingleeleeleebc123No ratings yet
- Service Manual - NEC Versa 2700 Series LaptopDocument130 pagesService Manual - NEC Versa 2700 Series LaptopToan NguyenNo ratings yet
- HUAWEI - SUN2000-20-40KTL-M3-UserManual GCADocument102 pagesHUAWEI - SUN2000-20-40KTL-M3-UserManual GCAReardon MetalsNo ratings yet
- How To Download A Windows 10 ISO File - PCWorldDocument3 pagesHow To Download A Windows 10 ISO File - PCWorldRajeev BatraNo ratings yet
- Reflection Paper On "Legal Research, Legal Writing, and Legal Analysis: Putting Law School Into Practice" by Suzanne RoweDocument2 pagesReflection Paper On "Legal Research, Legal Writing, and Legal Analysis: Putting Law School Into Practice" by Suzanne RoweRobert Jay Regz Pastrana IINo ratings yet
- Sustainable Consumption Production in India - AnalysisDocument8 pagesSustainable Consumption Production in India - Analysisanon_794541559No ratings yet
- Current ElectricityDocument93 pagesCurrent ElectricitySurya SNo ratings yet
- Form 137Document2 pagesForm 137Raymund BondeNo ratings yet