Download as pdf or txt
You might also like
- Renal Nursing ReviewerDocument8 pagesRenal Nursing ReviewerGeraldine Waje100% (2)
- ESRD Case Analysis - Group 4Document34 pagesESRD Case Analysis - Group 4Sean Jeffrey J. FentressNo ratings yet
- Orientation ScheduleDocument6 pagesOrientation ScheduleNur Shafiqa Clancy RajitNo ratings yet
- Advances in Membrane Science and TechnologyDocument326 pagesAdvances in Membrane Science and TechnologyKhuram Maqsood100% (3)
- Bbraun Dialog+ Datasheet PDFDocument2 pagesBbraun Dialog+ Datasheet PDFBertha DuránNo ratings yet
- Study of Etiology, Clinical Profile and Outcome of Acute Kidney (AKI) in Medical Intensive Care UnitDocument4 pagesStudy of Etiology, Clinical Profile and Outcome of Acute Kidney (AKI) in Medical Intensive Care UnitDavid Al HavizNo ratings yet
- A Study To Assess Changes in The Hematological Profile in Chronic Kidney DiseaseDocument3 pagesA Study To Assess Changes in The Hematological Profile in Chronic Kidney Diseasemandhalanarshimlu48141No ratings yet
- Study of Clinical Profile of Patient With Acute Kidney DiseaseDocument7 pagesStudy of Clinical Profile of Patient With Acute Kidney DiseaseIJAR JOURNALNo ratings yet
- Research Article: Incidence and Risk Factors For Early Acute Kidney Injury in Nonsurgical Patients: A Cohort StudyDocument9 pagesResearch Article: Incidence and Risk Factors For Early Acute Kidney Injury in Nonsurgical Patients: A Cohort StudyAbdul RahimNo ratings yet
- Risk Factors For Mortality in Acute Kidney InjuryDocument6 pagesRisk Factors For Mortality in Acute Kidney Injuryredouane bennaiNo ratings yet
- Kim-1 in CPBDocument6 pagesKim-1 in CPBkhaerul_fkuhNo ratings yet
- Acute Kidney Injury: Current Concepts and New Insights: Key WordsDocument5 pagesAcute Kidney Injury: Current Concepts and New Insights: Key WordsIHNo ratings yet
- Study of Etiology LALAJUNDocument3 pagesStudy of Etiology LALAJUNDavid Al HavizNo ratings yet
- Clinical Profile and Predictors of Renal Failure in Eme - 2022 - African JournalDocument5 pagesClinical Profile and Predictors of Renal Failure in Eme - 2022 - African JournalHajji AhmedNo ratings yet
- Artificial Intelligence in Healthcare: A ReviewDocument7 pagesArtificial Intelligence in Healthcare: A ReviewIJPS : A Pharmaceutical JournalNo ratings yet
- Prevention and Management of Acute Kidney InjuryDocument30 pagesPrevention and Management of Acute Kidney InjuryIren DawsonNo ratings yet
- Acute Kidney Injury An UpdateDocument9 pagesAcute Kidney Injury An Updatekarol fernandezNo ratings yet
- Irnf 45 2166531Document9 pagesIrnf 45 2166531Romina Belen Mendez PerezNo ratings yet
- Tgi Erc 3Document10 pagesTgi Erc 3Adrian LaimeNo ratings yet
- CKD PDFDocument7 pagesCKD PDFniaNo ratings yet
- Hepatitis B KronikDocument15 pagesHepatitis B KronikSiti NcitNo ratings yet
- Identification of Precipitating Factors in Hepatic Encephalopathy Patients at Liaquat University Hospital JamshoroDocument6 pagesIdentification of Precipitating Factors in Hepatic Encephalopathy Patients at Liaquat University Hospital JamshoroApotik ApotekNo ratings yet
- 1 Ajaz 2012Document4 pages1 Ajaz 2012Olivia Valentine LekiNo ratings yet
- Risk Factors For Acute Kidney Injury in Acute Pancreatitis: Riginal RticleDocument6 pagesRisk Factors For Acute Kidney Injury in Acute Pancreatitis: Riginal RticleDavid Sebastian Boada PeñaNo ratings yet
- Jurnal VaskularDocument5 pagesJurnal VaskulardrelvNo ratings yet
- Lec - S32 Injuria RenalDocument8 pagesLec - S32 Injuria RenalEvelyn EstradaNo ratings yet
- Electrolyte Imbalance in CKD PatientsDocument4 pagesElectrolyte Imbalance in CKD PatientsEditor IJTSRDNo ratings yet
- Jabak Et Al 2022 Management of Acute Diarrhea in The Emergency Department of A Tertiary Care University Medical CenterDocument10 pagesJabak Et Al 2022 Management of Acute Diarrhea in The Emergency Department of A Tertiary Care University Medical CenteranakmaidNo ratings yet
- Treatment of Acute Kidney InjuryDocument18 pagesTreatment of Acute Kidney Injuryqayyum consultantfpscNo ratings yet
- FuroDocument9 pagesFurodonadoguillermoNo ratings yet
- 1 s2.0 S1051227616301789 MainDocument7 pages1 s2.0 S1051227616301789 MainResearch OfficeNo ratings yet
- Pancytopenia A Clinico Hematological StudyDocument6 pagesPancytopenia A Clinico Hematological StudyUci Rahmadhani MNo ratings yet
- A Descriptive Study To Assess The Quality of Life of Patients Undergoing Hemodialysis in Sharda Hospital, Greater NoidaDocument7 pagesA Descriptive Study To Assess The Quality of Life of Patients Undergoing Hemodialysis in Sharda Hospital, Greater NoidaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 154-The Frequency and Aetiology of Repeated Kidney Injury Episodes Determine The Degree of Renal DamageDocument2 pages154-The Frequency and Aetiology of Repeated Kidney Injury Episodes Determine The Degree of Renal DamageCarlos Martinez SalgadoNo ratings yet
- Clinical Profile of Patients With Obstructive Jaundice: A Surgeon's PerspectivesDocument5 pagesClinical Profile of Patients With Obstructive Jaundice: A Surgeon's Perspectivessitoxpadang ceriaNo ratings yet
- Steroid-AssociatedSideEffectsinPatients WithPrimaryProteinuricKidneyDiseaseDocument9 pagesSteroid-AssociatedSideEffectsinPatients WithPrimaryProteinuricKidneyDiseaseIndah SolehaNo ratings yet
- Adler 2015Document7 pagesAdler 2015nathaliepichardoNo ratings yet
- International Journal of Infectious Diseases: Signe M. Sørensen, Henrik C. Schønheyder, Henrik NielsenDocument5 pagesInternational Journal of Infectious Diseases: Signe M. Sørensen, Henrik C. Schønheyder, Henrik NielsenNur Syamsiah MNo ratings yet
- Clinical Predictors of Renal Non-Recovery in ARDSDocument10 pagesClinical Predictors of Renal Non-Recovery in ARDSRayCassidyNo ratings yet
- Diagnosis and Treatment of Acute Kidney Injury in PediatricsDocument13 pagesDiagnosis and Treatment of Acute Kidney Injury in PediatricsagungNo ratings yet
- Protein Energy Malnutrition in CKD PatientsDocument4 pagesProtein Energy Malnutrition in CKD PatientsEditor IJTSRDNo ratings yet
- Early TIPS Versus Endoscopic Therapy For Secondary Prophylaxis After Management of Acute Esophageal Variceal Bleeding in Cirrhotic Patients: A Meta-Analysis of Randomized Controlled TrialsDocument26 pagesEarly TIPS Versus Endoscopic Therapy For Secondary Prophylaxis After Management of Acute Esophageal Variceal Bleeding in Cirrhotic Patients: A Meta-Analysis of Randomized Controlled Trialsray liNo ratings yet
- Pathological Profile and Recovery Rate in Patients With Drug-Induced Acute Kidney Injury: A Retrospective Study From North-East IndiaDocument7 pagesPathological Profile and Recovery Rate in Patients With Drug-Induced Acute Kidney Injury: A Retrospective Study From North-East IndiaIJAR JOURNALNo ratings yet
- A Study of Clinical Profile and Predictors of Poor Outcome in Snake Bite Induced Acute Kidney InjuryDocument6 pagesA Study of Clinical Profile and Predictors of Poor Outcome in Snake Bite Induced Acute Kidney InjuryIJAR JOURNALNo ratings yet
- A Retrospective Cohort Study On The Clinical Outcomes of Patients Admitted To Intensive Care Units With DysnatremiaDocument10 pagesA Retrospective Cohort Study On The Clinical Outcomes of Patients Admitted To Intensive Care Units With DysnatremiaEdo RezaprasgaNo ratings yet
- Effect of Comprehensive Nursing Strategies On Thirst Distress Management Among The Patients With Chronic Kidney Disease (CKD)Document6 pagesEffect of Comprehensive Nursing Strategies On Thirst Distress Management Among The Patients With Chronic Kidney Disease (CKD)yanuar esthoNo ratings yet
- Research Paper On Polycystic Kidney DiseaseDocument4 pagesResearch Paper On Polycystic Kidney Diseaseafeeotove100% (1)
- Pancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoDocument6 pagesPancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoYeni PuspitasariNo ratings yet
- Prerenalacutekidneyinjury 2020Document9 pagesPrerenalacutekidneyinjury 2020diana ramirezNo ratings yet
- Ijn 27 440Document6 pagesIjn 27 440Arun SedhainNo ratings yet
- Renal Outcomes Following Intravenous Contrast Administration in Patients With Acute Kidney Injury: A Multi-Site Retrospective Propensity-Adjusted AnalysisDocument11 pagesRenal Outcomes Following Intravenous Contrast Administration in Patients With Acute Kidney Injury: A Multi-Site Retrospective Propensity-Adjusted AnalysisYo Me100% (1)
- Chronic Kidney Disease in The Emergency Centre: A Prospective Observational StudyDocument7 pagesChronic Kidney Disease in The Emergency Centre: A Prospective Observational StudyHana Hikma FaizaNo ratings yet
- Renal Biopsy of Dogs and CatsDocument12 pagesRenal Biopsy of Dogs and CatsfrankyNo ratings yet
- Clinical Outcomes and Mortality in Elderly Peritoneal Dialysis PatientsDocument6 pagesClinical Outcomes and Mortality in Elderly Peritoneal Dialysis PatientsbayuNo ratings yet
- Bjs 11429Document10 pagesBjs 11429Pablo García HumérezNo ratings yet
- Determinants Influencing Length of Icu Stay in Renal Transplant Recipients Undergoing General AnaesthesiaDocument8 pagesDeterminants Influencing Length of Icu Stay in Renal Transplant Recipients Undergoing General AnaesthesiaIJAR JOURNALNo ratings yet
- Quality of Life of Caregivers and Patients On Peritoneal DialysisDocument7 pagesQuality of Life of Caregivers and Patients On Peritoneal Dialysisandrada14No ratings yet
- GastroprofilaxisDocument8 pagesGastroprofilaxisDaniel Alejandro Lecaros BarríaNo ratings yet
- Periop AKIDocument12 pagesPeriop AKINavjot KaurNo ratings yet
- Acute Kidney Injury - Final Draft (08 January 2011)Document58 pagesAcute Kidney Injury - Final Draft (08 January 2011)Mary-kate HengNo ratings yet
- Journal For MEdical WardDocument8 pagesJournal For MEdical WardValcrist BalderNo ratings yet
- Predicting Risk of Recurrent Acute Kidney Injury: A Systematic ReviewDocument8 pagesPredicting Risk of Recurrent Acute Kidney Injury: A Systematic ReviewJhon JeffreyNo ratings yet
- Incidence and Characteristics of Acute Kidney Injury in Severe Diabetic KetoacidosisDocument6 pagesIncidence and Characteristics of Acute Kidney Injury in Severe Diabetic KetoacidosisMarcelliaNo ratings yet
- Version of Record Doi: 10.1002/HEP.31884Document84 pagesVersion of Record Doi: 10.1002/HEP.31884Thien Nhan MaiNo ratings yet
- Core Concepts in Acute Kidney InjuryFrom EverandCore Concepts in Acute Kidney InjurySushrut S. WaikarNo ratings yet
- Brentuximab Vedotin - Handout - 1mar2016 PDFDocument5 pagesBrentuximab Vedotin - Handout - 1mar2016 PDFAkhileshNo ratings yet
- Payslip For The Month of Aug-2020: Sahyadri Hospitals LTD (SHL Academics)Document1 pagePayslip For The Month of Aug-2020: Sahyadri Hospitals LTD (SHL Academics)AkhileshNo ratings yet
- Life Insurance Corporation of IndiaDocument1 pageLife Insurance Corporation of IndiaAkhileshNo ratings yet
- Indian Income Tax Return Acknowledgement: Do Not Send This Acknowledgement To CPC, BengaluruDocument1 pageIndian Income Tax Return Acknowledgement: Do Not Send This Acknowledgement To CPC, BengaluruAkhileshNo ratings yet
- Statement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument5 pagesStatement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceAkhileshNo ratings yet
- Cranial Nerve Palsies Following Head Injury: Duncan D Mugala, Mwila M, Benaya Chibale, Womba KadochiDocument6 pagesCranial Nerve Palsies Following Head Injury: Duncan D Mugala, Mwila M, Benaya Chibale, Womba KadochiAkhileshNo ratings yet
- Sample Size CalculationDocument52 pagesSample Size CalculationAkhileshNo ratings yet
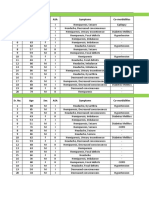
- Burr Hole Group Sr. No. Age Sex ASA Symptoms Co-MorbiditiesDocument18 pagesBurr Hole Group Sr. No. Age Sex ASA Symptoms Co-MorbiditiesAkhileshNo ratings yet
- Sample Size CalculationDocument53 pagesSample Size CalculationAkhileshNo ratings yet
- Embryonal Tumors of The Central Nervous System: Robert Y. Shih, LTC, MC, USA Kelly K. Koeller, MDDocument17 pagesEmbryonal Tumors of The Central Nervous System: Robert Y. Shih, LTC, MC, USA Kelly K. Koeller, MDAkhileshNo ratings yet
- 1 Principles of HemodialysisDocument5 pages1 Principles of HemodialysisZaid Alfaathih100% (2)
- Protocol TPEDocument19 pagesProtocol TPEPatricia TamasNo ratings yet
- Course in The Ward: DialysisDocument4 pagesCourse in The Ward: DialysisRayjundie EstradaNo ratings yet
- Day 1Document55 pagesDay 1ivancalderon867374No ratings yet
- Dialysis Disequilibrium SyndromeDocument7 pagesDialysis Disequilibrium Syndromesatyagraha84No ratings yet
- CGHS RatesDocument41 pagesCGHS RatesNagesh RaoNo ratings yet
- NURS FPX 6021 Assessment 2 Change Strategy and ImplementationDocument6 pagesNURS FPX 6021 Assessment 2 Change Strategy and Implementationjoohnsmith070No ratings yet
- Chapter54 Management of Patients With Kidney DisordersDocument40 pagesChapter54 Management of Patients With Kidney Disordersjericho dinglasanNo ratings yet
- 5 - Cleaning and Disinfection of Dialysis Water Equipment - Final - 2012Document7 pages5 - Cleaning and Disinfection of Dialysis Water Equipment - Final - 2012Denisse Ro100% (1)
- The 4 Types of Dialysis Access - Azura Vascular CareDocument14 pagesThe 4 Types of Dialysis Access - Azura Vascular CarevwyldrNo ratings yet
- Nutr 409 Case StudyDocument8 pagesNutr 409 Case Studyapi-301024560No ratings yet
- What Is Kidney (Renal) Failure?: Female Urinary TractDocument6 pagesWhat Is Kidney (Renal) Failure?: Female Urinary TractthenameisvijayNo ratings yet
- Agua BPDocument3 pagesAgua BPEdgar Condori MendozaNo ratings yet
- Calibration ManualDocument56 pagesCalibration ManualMaxence Kouessi100% (1)
- Checklist of Adult 2 - 2023-FinalDocument36 pagesChecklist of Adult 2 - 2023-FinalAhmed YasserNo ratings yet
- Vascular Access Type, Inflammatory Markers, and Mortality in Incident Hemodialysis PatientsDocument18 pagesVascular Access Type, Inflammatory Markers, and Mortality in Incident Hemodialysis PatientsYulius DonyNo ratings yet
- Essential Notes in Internal Medicine - 1st EdDocument163 pagesEssential Notes in Internal Medicine - 1st EdEhsanullah HikmatNo ratings yet
- Plasma Refilling in HemodialysDocument4 pagesPlasma Refilling in Hemodialysahmed AlayoudNo ratings yet
- MDT AI Patent ApplicationDocument21 pagesMDT AI Patent ApplicationCharles GrossNo ratings yet
- CKD MedscapeDocument65 pagesCKD MedscapeLuses Shantia HaryantoNo ratings yet
- Hemodialysis Central Venous Catheter STH ProtocolDocument2 pagesHemodialysis Central Venous Catheter STH ProtocolNor HilaliahNo ratings yet
- Dual Bicarb STD Install ManualDocument26 pagesDual Bicarb STD Install ManualIsLaM RaGaBNo ratings yet
- 6008 CARE System Technical Fact SheetDocument6 pages6008 CARE System Technical Fact SheetJéssica OinonenNo ratings yet
- In Summary of Discharge TeachingDocument2 pagesIn Summary of Discharge Teachingdalaginding clophNo ratings yet
- AAI Medical Scheme Help Book PDFDocument34 pagesAAI Medical Scheme Help Book PDFsukanto85No ratings yet