Download as pdf or txt
You might also like
- Record Sheet, Year 1: Please Submit These Record Sheets To Your Instructor After Completing The Simulation. Thank You!Document5 pagesRecord Sheet, Year 1: Please Submit These Record Sheets To Your Instructor After Completing The Simulation. Thank You!Randi Kosim SiregarNo ratings yet
- Awesome Engineering Activities For Kids - 50+ Exciting STEAM Projects To Design and Build (Awesome STEAM Activities For Kids)Document227 pagesAwesome Engineering Activities For Kids - 50+ Exciting STEAM Projects To Design and Build (Awesome STEAM Activities For Kids)Leonardo Rodrigues86% (7)
- Primarchs DatasheetsDocument24 pagesPrimarchs DatasheetsJosiah Young1100% (5)
- Dynamic Imaging of The Fetal Heart Using Metric Optimized GatingDocument19 pagesDynamic Imaging of The Fetal Heart Using Metric Optimized GatingdpnairNo ratings yet
- 247 2014 Article 3164Document7 pages247 2014 Article 3164Fahmil AgungNo ratings yet
- MapseDocument6 pagesMapseRaul GascueñaNo ratings yet
- PRedice CV Mortality With CT Nat Comm 2021Document9 pagesPRedice CV Mortality With CT Nat Comm 2021Guilherme Taborda RibasNo ratings yet
- Multiparametric Whole Body MRI With Diffusion Weighted Imaging - 2018 - AcademiDocument10 pagesMultiparametric Whole Body MRI With Diffusion Weighted Imaging - 2018 - AcademiRicardo MirandaNo ratings yet
- Applications of Routine Cardiac Mri Pulse Sequences - A Contemporary ReviewDocument5 pagesApplications of Routine Cardiac Mri Pulse Sequences - A Contemporary ReviewDimitar KosturkovNo ratings yet
- Advanced Assessment of Cardiac Morphology and Prediction of Gene Carriage by CMR in Hypertrophic Cardiomyopathy The Hcmnet Ucl CollaborationDocument3 pagesAdvanced Assessment of Cardiac Morphology and Prediction of Gene Carriage by CMR in Hypertrophic Cardiomyopathy The Hcmnet Ucl CollaborationAfreen BegumNo ratings yet
- Frosted DesignDocument11 pagesFrosted Designhoormohameed2019No ratings yet
- Hypertonic Saline Attenuates Cord Swelling and Edema in Experimental Cord Injury - Experimental (2009) PDFDocument7 pagesHypertonic Saline Attenuates Cord Swelling and Edema in Experimental Cord Injury - Experimental (2009) PDFCoal CoalyNo ratings yet
- Ef 42Document7 pagesEf 42rhegi isdiara FairuzNo ratings yet
- Methods For Normalization of Hippocampal VolumesDocument7 pagesMethods For Normalization of Hippocampal VolumesmarkecbNo ratings yet
- Zuva MuzachimDocument6 pagesZuva MuzachimZuva MuzachimNo ratings yet
- Kaleem 2017Document12 pagesKaleem 2017Rajalingam BossNo ratings yet
- Validation of A Semiautomated Volumetric Approach For Fetal Neurosonography Using 5DCNS in Clinical DataDocument7 pagesValidation of A Semiautomated Volumetric Approach For Fetal Neurosonography Using 5DCNS in Clinical DataVishnu priya kokkulaNo ratings yet
- Electrocardiography: Selection The Positions Measuring LocationsDocument14 pagesElectrocardiography: Selection The Positions Measuring LocationsSivaRaman JayaramanNo ratings yet
- 1.01. Asian Consortium On Radiation Dose of Pediatric CardiacDocument12 pages1.01. Asian Consortium On Radiation Dose of Pediatric Cardiacfaizahameliar08No ratings yet
- Magnetic Resonance Imaging and Cardiac Pacemaker Safety at 1.5-TeslaDocument10 pagesMagnetic Resonance Imaging and Cardiac Pacemaker Safety at 1.5-TeslaCălin RoxanaNo ratings yet
- Intelligent SMOTE Based Machine Learning Classi Cation For Fetal State On Cardiotocography DatasetDocument17 pagesIntelligent SMOTE Based Machine Learning Classi Cation For Fetal State On Cardiotocography DatasetIfat TalukdarNo ratings yet
- 1 s2.0 S0140673618324905 MainDocument9 pages1 s2.0 S0140673618324905 Mainprizankenny10No ratings yet
- 1369 Full PDFDocument9 pages1369 Full PDFIqbal AbdillahNo ratings yet
- 006 - A Prospective, Comparative Analysis of Inhibin-B, AMH and 3D US Determinants of Ovarian Reserve in The Prediction of Poor Response To COSDocument10 pages006 - A Prospective, Comparative Analysis of Inhibin-B, AMH and 3D US Determinants of Ovarian Reserve in The Prediction of Poor Response To COSAripinSyarifudinNo ratings yet
- Cerebral Blood Flow by Arterial Spin Labeling in Poststroke DementiaDocument7 pagesCerebral Blood Flow by Arterial Spin Labeling in Poststroke DementiaNovita WulandariNo ratings yet
- EJMCM - Volume 9 - Issue 3 - Pages 5157-5169Document13 pagesEJMCM - Volume 9 - Issue 3 - Pages 5157-5169AjeetalbertNo ratings yet
- Synthbraingrow: Synthetic Diffusion Brain Aging For Longitudinal Mri Data Generation in Young PeopleDocument10 pagesSynthbraingrow: Synthetic Diffusion Brain Aging For Longitudinal Mri Data Generation in Young PeopleJason VoorheesNo ratings yet
- SkewnessDocument5 pagesSkewnessNandhini Paramasivam100% (1)
- F QRSDocument9 pagesF QRSaisyah hamzakirNo ratings yet
- Quantification in Cardiac MRI Advances in Image Acquisition and ProcessingDocument14 pagesQuantification in Cardiac MRI Advances in Image Acquisition and ProcessingLY SovantolaNo ratings yet
- Computers in Biology and Medicine: Shuicai Wu, Yanni Shen, Zhuhuang Zhou, Lan Lin, Yanjun Zeng, Xiaofeng GaoDocument6 pagesComputers in Biology and Medicine: Shuicai Wu, Yanni Shen, Zhuhuang Zhou, Lan Lin, Yanjun Zeng, Xiaofeng GaoRIDAKORDOR KAMAR,BIOMEDICAL(19-23) Vel Tech, ChennaiNo ratings yet
- 10.1016@S0140 67361931721 0Document7 pages10.1016@S0140 67361931721 0Oana DrăganNo ratings yet
- Deep Learning Predicts Hip Fracture Using Confounding Patient and Healthcare VariablesDocument17 pagesDeep Learning Predicts Hip Fracture Using Confounding Patient and Healthcare VariablesChrisNo ratings yet
- THE 19th CONGRESS OF THE ROMANIAN SOCIETY OF ANATOMY - v4 PDFDocument241 pagesTHE 19th CONGRESS OF THE ROMANIAN SOCIETY OF ANATOMY - v4 PDFGeorgiana ZahariaNo ratings yet
- TAMANHODAPELVERENALDocument5 pagesTAMANHODAPELVERENALantonio bernardesNo ratings yet
- Ss PDFDocument7 pagesSs PDFCălin RoxanaNo ratings yet
- Chong 2015Document5 pagesChong 2015yaniNo ratings yet
- Shore2018 RX PelvisDocument6 pagesShore2018 RX PelvismiguelpaillalefgutierrezNo ratings yet
- Pediatric Cardiology: Normal ECG Standards For Infants and ChildrenDocument9 pagesPediatric Cardiology: Normal ECG Standards For Infants and ChildrenRafael garciaNo ratings yet
- Goto MTLWechsler NeuroRad2011Document6 pagesGoto MTLWechsler NeuroRad2011Charu RaghavanNo ratings yet
- Art:10.1007/s00330 015 3805 1Document8 pagesArt:10.1007/s00330 015 3805 1Mihaela ToaderNo ratings yet
- Machine-Learning Algorithms To Automate Morphological and Functional Assessments in 2D EchocardiographyDocument9 pagesMachine-Learning Algorithms To Automate Morphological and Functional Assessments in 2D EchocardiographyLandon GrayNo ratings yet
- Diagnosis of Foetal Vein of Galen Aneurysmal Malformation by Ultrasound Combined With Magnetic Resonance Imaging: A Case SeriesDocument6 pagesDiagnosis of Foetal Vein of Galen Aneurysmal Malformation by Ultrasound Combined With Magnetic Resonance Imaging: A Case SeriesMega SeptianaNo ratings yet
- Brain PaperDocument5 pagesBrain PaperQanza AzamNo ratings yet
- Prehospital Electroencephalography To Detect Traumatic Brain Injury During Helicopter Transport: A Pilot Observational Cohort StudyDocument9 pagesPrehospital Electroencephalography To Detect Traumatic Brain Injury During Helicopter Transport: A Pilot Observational Cohort Study7mqvrxktsmNo ratings yet
- From EHG Signals UsingDocument6 pagesFrom EHG Signals UsingAkbar aliNo ratings yet
- Fetal DisritmiaDocument18 pagesFetal DisritmiaSebastian ChandraNo ratings yet
- Quantification of Stenotic Mitral Valve Area With Magnetic Resonance Imaging and Comparison With Doppler UltrasoundDocument5 pagesQuantification of Stenotic Mitral Valve Area With Magnetic Resonance Imaging and Comparison With Doppler UltrasoundRyanNo ratings yet
- Predicting Surgical Complications in Patients Undergoing Elective Adult Spinal Deformity Procedures Using Machine LearningDocument9 pagesPredicting Surgical Complications in Patients Undergoing Elective Adult Spinal Deformity Procedures Using Machine LearningDr-Rabia AlmamalookNo ratings yet
- T - P D U I R E: Hree Dimensional and Ower Oppler Ltrasonography in Nfertility and Eproductive NdocrinologyDocument6 pagesT - P D U I R E: Hree Dimensional and Ower Oppler Ltrasonography in Nfertility and Eproductive NdocrinologyAripinSyarifudinNo ratings yet
- Unstructured Data ManagementDocument6 pagesUnstructured Data ManagementSandhya SharmaNo ratings yet
- Deep Learning For MR Angiography: Automated Detection of Cerebral AneurysmsDocument8 pagesDeep Learning For MR Angiography: Automated Detection of Cerebral AneurysmseditingjuryNo ratings yet
- Algorithms 08 00395Document12 pagesAlgorithms 08 00395venkayammaNo ratings yet
- Research Article: Heart Disease Prediction Based On The Embedded Feature Selection Method and Deep Neural NetworkDocument9 pagesResearch Article: Heart Disease Prediction Based On The Embedded Feature Selection Method and Deep Neural NetworkHADIS FEIZINo ratings yet
- Alacam2008 2 2Document23 pagesAlacam2008 2 2John JonesNo ratings yet
- Pi Is 0300957221001544Document8 pagesPi Is 0300957221001544Peter ThaiNo ratings yet
- ECG Pediátrico InterpretaçãoDocument10 pagesECG Pediátrico InterpretaçãoNITACORDEIRONo ratings yet
- Image Processing and Visualization TopicsDocument16 pagesImage Processing and Visualization TopicsBradda Derru Nesta MarleyNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and Researchrhegi isdiara FairuzNo ratings yet
- Automatic Measurement of Fetal Femur Length in Ultrasound Images: A Comparison of Random Forest Regression Model and SegnetDocument16 pagesAutomatic Measurement of Fetal Femur Length in Ultrasound Images: A Comparison of Random Forest Regression Model and SegnetSharifahobaid AlrashidiNo ratings yet
- 11C MetioninaDocument8 pages11C MetioninaPUIGCOZARNo ratings yet
- Computed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideFrom EverandComputed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideNo ratings yet
- BB and B MIT Award 2020 Application FormDocument6 pagesBB and B MIT Award 2020 Application FormdpnairNo ratings yet
- Boxplot ExplanationDocument2 pagesBoxplot ExplanationdpnairNo ratings yet
- COEX Clover Drone Kit SpecificationDocument1 pageCOEX Clover Drone Kit SpecificationdpnairNo ratings yet
- Way To Zero Defect: Prepared by VishnuDocument9 pagesWay To Zero Defect: Prepared by VishnudpnairNo ratings yet
- Laser Cut Model Plane 3d Puzzle DXF Free Download PDFDocument1 pageLaser Cut Model Plane 3d Puzzle DXF Free Download PDFdpnairNo ratings yet
- Unit 2 TransformationDocument8 pagesUnit 2 TransformationdpnairNo ratings yet
- Dynamic Imaging of The Fetal Heart Using Metric Optimized GatingDocument19 pagesDynamic Imaging of The Fetal Heart Using Metric Optimized GatingdpnairNo ratings yet
- Sewing Section: Technical/Production Team SopDocument4 pagesSewing Section: Technical/Production Team SopdpnairNo ratings yet
- Booked By: Guest (Guest) Printed On: 01/08/2017 At: 12:59:57: E-Ticket/Reservation VoucherDocument8 pagesBooked By: Guest (Guest) Printed On: 01/08/2017 At: 12:59:57: E-Ticket/Reservation VoucherdpnairNo ratings yet
- Ibg Jordan Inspection Report AnalysisDocument6 pagesIbg Jordan Inspection Report AnalysisdpnairNo ratings yet
- Cutting Section: Technichal Team'S S.O.PDocument5 pagesCutting Section: Technichal Team'S S.O.PdpnairNo ratings yet
- Layout InlineDocument62 pagesLayout InlinedpnairNo ratings yet
- SOP1Document2 pagesSOP1dpnairNo ratings yet
- Ibg Jordan: Unit 1 Section Packing Date 9-FebDocument6 pagesIbg Jordan: Unit 1 Section Packing Date 9-FebdpnairNo ratings yet
- Cellular Layout: Case StudyDocument7 pagesCellular Layout: Case StudydpnairNo ratings yet
- Ibg Jordan Unit I-Daily Cost Report July'14Document1 pageIbg Jordan Unit I-Daily Cost Report July'14dpnairNo ratings yet
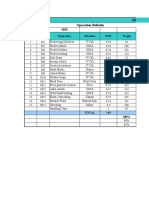
- Ibg Jordan Operation Bulletin Style #102: SL# Code Operation Machine SMV TargetDocument11 pagesIbg Jordan Operation Bulletin Style #102: SL# Code Operation Machine SMV TargetdpnairNo ratings yet
- Domain: PeriodDocument21 pagesDomain: PerioddpnairNo ratings yet
- CM Analysis: Ibg JordanDocument6 pagesCM Analysis: Ibg JordandpnairNo ratings yet
- Summary-Unit 1 Factors January February March April MAYDocument13 pagesSummary-Unit 1 Factors January February March April MAYdpnairNo ratings yet
- International British Garments Skill Matrix Analysis: Operation Process Rating % Result Remarks Target AchievedDocument8 pagesInternational British Garments Skill Matrix Analysis: Operation Process Rating % Result Remarks Target AchieveddpnairNo ratings yet
- Design and Development of Unmanned Aerial Vehicle (Drone) For Civil ApplicationsDocument16 pagesDesign and Development of Unmanned Aerial Vehicle (Drone) For Civil ApplicationsdpnairNo ratings yet
- Cost Per Minute 2013Document76 pagesCost Per Minute 2013dpnairNo ratings yet
- Cost Per Minute Till May 2014Document86 pagesCost Per Minute Till May 2014dpnairNo ratings yet
- File 2Document36 pagesFile 2dpnairNo ratings yet
- Itch Mechanisms and ManagementDocument464 pagesItch Mechanisms and ManagementGaurav JaswalNo ratings yet
- 2021 HhhhhhhterqasdwqwDocument1 page2021 HhhhhhhterqasdwqwHassan KhanNo ratings yet
- MTM Lab (Metrology Part) - Spring 2021Document12 pagesMTM Lab (Metrology Part) - Spring 2021Rahul Raghunath BodankiNo ratings yet
- Testbank ch01Document14 pagesTestbank ch01HườngNo ratings yet
- EScan Corporate 360 UGDocument601 pagesEScan Corporate 360 UG11F10 RUCHITA MAARANNo ratings yet
- Peek - POLYETHER ETHER KETONEDocument58 pagesPeek - POLYETHER ETHER KETONEBryan Jesher Dela Cruz100% (1)
- COOKERY 9 Q3.Mod1Document5 pagesCOOKERY 9 Q3.Mod1Jessel Mejia Onza100% (4)
- ITSM Gap Analysis TemplateDocument57 pagesITSM Gap Analysis TemplateSuresh RajamaniNo ratings yet
- Compiler Construction LabDocument11 pagesCompiler Construction LabSunny0% (1)
- Working With MongoDB - 518Document11 pagesWorking With MongoDB - 518Sivaraman AlagappanNo ratings yet
- 1.the Perception of Local Street Food VendorsDocument28 pages1.the Perception of Local Street Food VendorsJay Vince Agpoon MendozaNo ratings yet
- AKS32-33 TebrDocument4 pagesAKS32-33 TebrtaupiqNo ratings yet
- Detailed Lesson Plan in English For Grade 7-I. ObjectivesDocument6 pagesDetailed Lesson Plan in English For Grade 7-I. ObjectivesAra OngNo ratings yet
- Ghinea Gabriela Nouella and Manea Madalina ElenaDocument25 pagesGhinea Gabriela Nouella and Manea Madalina ElenaAlexandria Firdaus Al-farisyNo ratings yet
- Final Project On Employee EngagementDocument97 pagesFinal Project On Employee EngagementSanju DurgapalNo ratings yet
- 3987 SDS (GHS) - I-ChemDocument4 pages3987 SDS (GHS) - I-ChemAmirHakimRusliNo ratings yet
- Fizika RadiologijaDocument9 pagesFizika RadiologijaBorislav TapavičkiNo ratings yet
- Invoice: PT - Sitc IndonesiaDocument1 pageInvoice: PT - Sitc IndonesiaMuhammad SyukurNo ratings yet
- Machining of Bezier Curve by Macro ProgrammingDocument7 pagesMachining of Bezier Curve by Macro ProgrammingAtul ChauhanNo ratings yet
- Distribution Channel of AMULDocument13 pagesDistribution Channel of AMULMeet JivaniNo ratings yet
- ESD122 2-Channel ESD Protection Diode For USB Type-C and HDMI 2.0Document27 pagesESD122 2-Channel ESD Protection Diode For USB Type-C and HDMI 2.0H tavangarNo ratings yet
- Submarine Diesel EngineDocument106 pagesSubmarine Diesel EngineDharma Gita Surya PrayogaNo ratings yet
- Torrent WorkingDocument7 pagesTorrent WorkingsirmadamstudNo ratings yet
- 2intro To LLMDDocument2 pages2intro To LLMDKristal ManriqueNo ratings yet
- SSP 666 Audi A8 Type 4N Infotainment and Audi ConnectDocument72 pagesSSP 666 Audi A8 Type 4N Infotainment and Audi Connectylk1No ratings yet
- Eaton DX-RT 6000 VA (Long Back UP) 1x1 UPS SystemDocument4 pagesEaton DX-RT 6000 VA (Long Back UP) 1x1 UPS SystemPhaniNo ratings yet
- The Bishop ScoreDocument3 pagesThe Bishop ScoreJheanAlphonsineT.MeansNo ratings yet