Download as pdf or txt
You might also like
- The Sleep Technician Guide: Practical Aspects of Sleep DiagnosticDocument0 pagesThe Sleep Technician Guide: Practical Aspects of Sleep Diagnosticsg1964No ratings yet
- Biofeedback An Evidence Based Approach in Clinical Practice: January 2009Document12 pagesBiofeedback An Evidence Based Approach in Clinical Practice: January 2009bastianusjuatmadjaNo ratings yet
- Tmpa535 TMPDocument6 pagesTmpa535 TMPFrontiersNo ratings yet
- Biofeedback Improves Activities of The Lower Limb After Stroke A Systematic ReviewDocument11 pagesBiofeedback Improves Activities of The Lower Limb After Stroke A Systematic ReviewDatta Srihari NaiduNo ratings yet
- Poststroke Fatigue 2012Document11 pagesPoststroke Fatigue 2012RuiNo ratings yet
- TaubCragoUswatte CIMTreview RehabPsy98Document20 pagesTaubCragoUswatte CIMTreview RehabPsy98RazvanRotaruNo ratings yet
- PIIS1360859220300231Document12 pagesPIIS1360859220300231Максим ВикторовичNo ratings yet
- 2013 Motivational 2Document7 pages2013 Motivational 2Harm op den AkkerNo ratings yet
- Functional Assessment in Physiotherapy. A Literature Review: Europa Medicophysica January 2008Document18 pagesFunctional Assessment in Physiotherapy. A Literature Review: Europa Medicophysica January 2008Yeshvi sNo ratings yet
- Jurnal Musculoskeletal System 2Document14 pagesJurnal Musculoskeletal System 2miraNo ratings yet
- Improvement of Dynamic Respiration Monitoring ThroDocument11 pagesImprovement of Dynamic Respiration Monitoring ThroKevin De PaulaNo ratings yet
- Steps That Count: Pedometer-Measured Physical Activity, Self-Reported Physical Activity and Current Guidelines-How Do They Relate?Document9 pagesSteps That Count: Pedometer-Measured Physical Activity, Self-Reported Physical Activity and Current Guidelines-How Do They Relate?Edmar MejiaNo ratings yet
- Audiffren Andr 2015Document31 pagesAudiffren Andr 2015Jan VybíralNo ratings yet
- The Measurement of Sedentary Patterns and Behavior PDFDocument15 pagesThe Measurement of Sedentary Patterns and Behavior PDFJajatNo ratings yet
- A Primer On Functional Analysis: Jerome Yoman Life Skills ResourceDocument16 pagesA Primer On Functional Analysis: Jerome Yoman Life Skills ResourceGuerrero NataliaNo ratings yet
- Journal Article Review BHS202. Nicole SantamariaDocument8 pagesJournal Article Review BHS202. Nicole SantamarianicolesantamriaNo ratings yet
- The Role of Biofeedback in Stroke Rehabilitation: Past and Future DirectionsDocument9 pagesThe Role of Biofeedback in Stroke Rehabilitation: Past and Future Directionsnandhini raguNo ratings yet
- SteeleDocument14 pagesSteelearnold22tangerangNo ratings yet
- Biofeedback NewDocument16 pagesBiofeedback NewSANYA KUNDRA dpsruNo ratings yet
- WilhelmPerrez2013 Ahistoryofresearchcoductedindailylife PDFDocument80 pagesWilhelmPerrez2013 Ahistoryofresearchcoductedindailylife PDFJanica GavinoNo ratings yet
- WilhelmPerrez2013 Ahistoryofresearchcoductedindailylife PDFDocument80 pagesWilhelmPerrez2013 Ahistoryofresearchcoductedindailylife PDFJanica GavinoNo ratings yet
- Clinical TVA - Based StudiesDocument18 pagesClinical TVA - Based StudiesChristian HeitmannNo ratings yet
- Physical Therapy Tests in Stroke RehabilitationDocument22 pagesPhysical Therapy Tests in Stroke Rehabilitationmehdi.chlif4374No ratings yet
- Development of An Ergonomically Designed Drafting Table and Chair For Engineering Students of Lpu LagunaDocument13 pagesDevelopment of An Ergonomically Designed Drafting Table and Chair For Engineering Students of Lpu LagunaMR BASICNo ratings yet
- tmp5D49 TMPDocument8 pagestmp5D49 TMPFrontiersNo ratings yet
- ENBM001: Biomedical Engineering Daniel Verdi Do AmaranteDocument50 pagesENBM001: Biomedical Engineering Daniel Verdi Do AmarantePeter Jay CorrosNo ratings yet
- The Bobath Concept inDocument12 pagesThe Bobath Concept inCedricFernandezNo ratings yet
- Plasqui 2012 Aspects of Activity Behavior AsDocument8 pagesPlasqui 2012 Aspects of Activity Behavior AsCarlos RodriguezNo ratings yet
- GPAQDocument6 pagesGPAQChibi ChanNo ratings yet
- Artical No 1 PDFDocument15 pagesArtical No 1 PDFShankranand TiwariNo ratings yet
- Using Physiological Measures To Evaluate User Experience of Mobile ApplicationsDocument11 pagesUsing Physiological Measures To Evaluate User Experience of Mobile ApplicationsFatima IsiakaNo ratings yet
- s00586 010 1543 2Document11 pagess00586 010 1543 2mohamed hazemNo ratings yet
- Sensorimotor Integration For FunctionalDocument17 pagesSensorimotor Integration For FunctionalFuncionalidad DiversaNo ratings yet
- MCQ 2Document9 pagesMCQ 2Munni KNo ratings yet
- Wearable Movement Sensors For RehabilitationDocument6 pagesWearable Movement Sensors For RehabilitationTom DisveldNo ratings yet
- Larsen MonitoresEjercicio BMJ 2022Document15 pagesLarsen MonitoresEjercicio BMJ 2022camila gomezNo ratings yet
- Biofeedback in Rehabilitation: Review Open AccessDocument11 pagesBiofeedback in Rehabilitation: Review Open AccessNistara Singh ChawlaNo ratings yet
- Neuropsychologia: SciencedirectDocument13 pagesNeuropsychologia: SciencedirectFernando GomesNo ratings yet
- OTB 520 - Week 9 Lecture 2 - Brunnstrom and NDT PDFDocument23 pagesOTB 520 - Week 9 Lecture 2 - Brunnstrom and NDT PDFDuaa AlwawiNo ratings yet
- A Short Questionnaire For The Assessment of Quality of Life in Patients With Chronic Obstructive Pulmonary Disease: Psychometric Properties of VQ11Document11 pagesA Short Questionnaire For The Assessment of Quality of Life in Patients With Chronic Obstructive Pulmonary Disease: Psychometric Properties of VQ11elonaNo ratings yet
- Comparative Analysis of Dynamic External Factors On The Body BehaviorDocument4 pagesComparative Analysis of Dynamic External Factors On The Body BehaviorAd FelixNo ratings yet
- Benefits of OBI For Upper ExterityDocument11 pagesBenefits of OBI For Upper Exteritysarawu9911No ratings yet
- Jette - 1989Document5 pagesJette - 1989Vanessa WittmayerNo ratings yet
- S Nie Scho SCHW 2005 Psychology HealthDocument19 pagesS Nie Scho SCHW 2005 Psychology HealthJip van AmerongenNo ratings yet
- WilhelmPerrez2013 AhistoryofresearchcoductedindailylifeDocument80 pagesWilhelmPerrez2013 AhistoryofresearchcoductedindailylifeDaniel San Martín CanteroNo ratings yet
- 273-Article Text-515-1-10-20190606Document6 pages273-Article Text-515-1-10-20190606Ardhyan ArdhyanNo ratings yet
- Adaptación Española Del Environmental Reward Observation Scale (Eros)Document14 pagesAdaptación Española Del Environmental Reward Observation Scale (Eros)Midori KobayashiNo ratings yet
- Foundations of Movement AnalysisDocument31 pagesFoundations of Movement AnalysisKavithaNo ratings yet
- Determining The Posture and Vibration Frequency THDocument7 pagesDetermining The Posture and Vibration Frequency THBeto VidalNo ratings yet
- Books Media-: Clinical Assessment Procedures in Physical TherapyDocument1 pageBooks Media-: Clinical Assessment Procedures in Physical Therapybrain jackNo ratings yet
- Breathing Movements of The Chest and Abdominal Wall in Healthy SubjectsDocument10 pagesBreathing Movements of The Chest and Abdominal Wall in Healthy SubjectsAnandhu GNo ratings yet
- Systematic Observation in Clinical PsychologyDocument4 pagesSystematic Observation in Clinical PsychologyVaniladie AliaNo ratings yet
- 1 Year: - ECG Reading Exercise (NOT DONE)Document1 page1 Year: - ECG Reading Exercise (NOT DONE)noneNo ratings yet
- Mechanisms of Action of Lumbar Supports: A Systematic ReviewDocument12 pagesMechanisms of Action of Lumbar Supports: A Systematic ReviewyohanNo ratings yet
- O Fortalecimento Combinado Do Abdutor Do Quadril e Do Rotador Externo e o Alongamento Do Rotador Interno Do Quadril Melhoram A Dor e A Função em Pacientes Com Síndrome Da Dor Femoropatelar Um EnsaiDocument6 pagesO Fortalecimento Combinado Do Abdutor Do Quadril e Do Rotador Externo e o Alongamento Do Rotador Interno Do Quadril Melhoram A Dor e A Função em Pacientes Com Síndrome Da Dor Femoropatelar Um EnsaiLeticia ZaniniiNo ratings yet
- Applied Behavior Analysis (ABA)Document22 pagesApplied Behavior Analysis (ABA)Ravi Varakala86% (7)
- 2010 - Rating Scales For Low Back Pain - Longo Et Al PDFDocument64 pages2010 - Rating Scales For Low Back Pain - Longo Et Al PDFA CNo ratings yet
- Technologies Used in Parkinson'S DiseaseDocument12 pagesTechnologies Used in Parkinson'S DiseaseDuka 1122No ratings yet
- A Study Into The Mediating Effect of Gamification On Self-Efficacy, Perceived BehaviouralDocument57 pagesA Study Into The Mediating Effect of Gamification On Self-Efficacy, Perceived Behaviouralkiwi DaiNo ratings yet
- Tutorial Mat Elastic Iac PDFDocument25 pagesTutorial Mat Elastic Iac PDFIulia CostacheNo ratings yet
- Disabled Village Children: A Guide For Community Health Workers, Rehabilitation Workers, and FamiliesDocument85 pagesDisabled Village Children: A Guide For Community Health Workers, Rehabilitation Workers, and FamiliesIulia CostacheNo ratings yet
- Fisa Tehnica Scula DebavurareDocument3 pagesFisa Tehnica Scula DebavurareIulia CostacheNo ratings yet
- Fisa Tehnica Scula DebavurareDocument3 pagesFisa Tehnica Scula DebavurareIulia CostacheNo ratings yet
- Manual Post de Stocare Scule PDFDocument81 pagesManual Post de Stocare Scule PDFIulia CostacheNo ratings yet
- Fisa Tehica Post de Stocare Scule 2Document1 pageFisa Tehica Post de Stocare Scule 2Iulia CostacheNo ratings yet
- Fisa Tehnica QC-5 Interfata MecanicaDocument1 pageFisa Tehnica QC-5 Interfata MecanicaIulia CostacheNo ratings yet
- Irbp R: PositionerDocument2 pagesIrbp R: PositionerIulia CostacheNo ratings yet
- Fltru Reg PresuneDocument1 pageFltru Reg PresuneIulia CostacheNo ratings yet
- Motoman Hp20D-6: Handling & General Applications With The HP-seriesDocument2 pagesMotoman Hp20D-6: Handling & General Applications With The HP-seriesIulia CostacheNo ratings yet
- Flyer Robot EPX Series E 06.2015 13 PDFDocument8 pagesFlyer Robot EPX Series E 06.2015 13 PDFIulia CostacheNo ratings yet
- Increasing The Robot's Working Area High Speed - Short Cycle Time Direct or Slewing DriveDocument2 pagesIncreasing The Robot's Working Area High Speed - Short Cycle Time Direct or Slewing DriveIulia CostacheNo ratings yet
- Flexible Lab Automation With The MOTOMAN CSDA10FDocument4 pagesFlexible Lab Automation With The MOTOMAN CSDA10FIulia CostacheNo ratings yet
- V Rep1Document51 pagesV Rep1Iulia CostacheNo ratings yet
- Compact Style Precise Servo Technology: Technical Data DK-250 DK-500 DK-1000 DK-1500 DK-2500Document1 pageCompact Style Precise Servo Technology: Technical Data DK-250 DK-500 DK-1000 DK-1500 DK-2500Iulia CostacheNo ratings yet
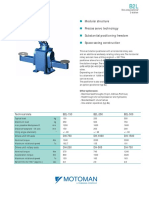
- Modular Structure Precise Servo Technology Substantial Positioning Freedom Space Saving ConstructionDocument2 pagesModular Structure Precise Servo Technology Substantial Positioning Freedom Space Saving ConstructionIulia CostacheNo ratings yet
- Compact Style Precise Servo Technology Substantial Positioning Freedom Space Saving ConstructionDocument2 pagesCompact Style Precise Servo Technology Substantial Positioning Freedom Space Saving ConstructionIulia CostacheNo ratings yet
- V Rep6Document30 pagesV Rep6Iulia CostacheNo ratings yet
- Modular Structure Precise Servo Technology Substantial Positioning Freedom Space Saving ConstructionDocument2 pagesModular Structure Precise Servo Technology Substantial Positioning Freedom Space Saving ConstructionIulia CostacheNo ratings yet
- 511E - 18 - CrossRollerRing COMPLETDocument56 pages511E - 18 - CrossRollerRing COMPLETIulia CostacheNo ratings yet
- Boubekri Et Al - 2014 - Impact of Windows and Daylight Exposure On Overall Health and Sleep Quality ofDocument9 pagesBoubekri Et Al - 2014 - Impact of Windows and Daylight Exposure On Overall Health and Sleep Quality ofDr.QiuNo ratings yet
- A Systematic Review of Circadian Function, Chronotype and Chronotherapy in Attention Deficit Hyperactivity DisorderDocument19 pagesA Systematic Review of Circadian Function, Chronotype and Chronotherapy in Attention Deficit Hyperactivity DisorderPAULANo ratings yet
- Nursing Students' Sleep Patterns and Perceptions of Safe Practice During Their Entree To Shift WorkDocument7 pagesNursing Students' Sleep Patterns and Perceptions of Safe Practice During Their Entree To Shift WorkshaviraNo ratings yet
- Test Bank For Pathophysiology Concepts of Human Disease 1st Edition Matthew Sorenson Lauretta Quinn Diane KleinDocument21 pagesTest Bank For Pathophysiology Concepts of Human Disease 1st Edition Matthew Sorenson Lauretta Quinn Diane Kleinedwardfrostxpybgdctkr100% (27)
- Fatigue Management Guide For General Aviation OperatorsDocument96 pagesFatigue Management Guide For General Aviation OperatorsAZOLWAY TRAVEL AGENTNo ratings yet
- Music Therapy As A Potential Intervention For Sleep ImprovementDocument9 pagesMusic Therapy As A Potential Intervention For Sleep ImprovementPaolo BertoliniNo ratings yet
- Bedtime Routines For Young ChildrenDocument6 pagesBedtime Routines For Young ChildrenmithaNo ratings yet
- Sleep Health Reciprocal Regulation of Sleep and Innate ImmunityDocument27 pagesSleep Health Reciprocal Regulation of Sleep and Innate ImmunityPolly MollyNo ratings yet
- Actiwatch Spec Sheet PDFDocument2 pagesActiwatch Spec Sheet PDFVarunSharmaNo ratings yet
- Sleep Studies in ChildrenDocument12 pagesSleep Studies in ChildrenJHONATAN MATA ARANDANo ratings yet
- Zopiclone Versus Placebo For Short TermDocument9 pagesZopiclone Versus Placebo For Short TermPandi PerumalNo ratings yet
- Accelerometer Data Collection and Processing Criteria To AssessDocument25 pagesAccelerometer Data Collection and Processing Criteria To AssessBJNo ratings yet
- Different Levels of Work Related Stress and The Effects On Sleep, Fatigue and CortisolDocument10 pagesDifferent Levels of Work Related Stress and The Effects On Sleep, Fatigue and CortisolMakhrus ShofiNo ratings yet
- Wearable Sensors and Their Metrics For Measuring Comprehensive Occupational Fatigue: A Scoping ReviewDocument5 pagesWearable Sensors and Their Metrics For Measuring Comprehensive Occupational Fatigue: A Scoping ReviewSusanWiliamNo ratings yet
- Sleep ParameterDocument18 pagesSleep ParameterBogi VargaNo ratings yet
- Post-Stroke InsomniaDocument9 pagesPost-Stroke InsomniaRizqan Fahlevvi AkbarNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscriptKondang WarasNo ratings yet
- Autism SleepDocument9 pagesAutism SleepdrimranmnooraniNo ratings yet
- Sleep-Wake Disturbances and Sleep Disorders in Patients With DementiaDocument45 pagesSleep-Wake Disturbances and Sleep Disorders in Patients With DementiaVolt HakimNo ratings yet
- Circadian Rhythm Sleep Disorders CRSDDocument11 pagesCircadian Rhythm Sleep Disorders CRSDjaime manciaNo ratings yet
- Patient Characteristics Affecting Accurate Detection of Sleep Apnea Using A Bed Sheet-Type Portable MonitorDocument8 pagesPatient Characteristics Affecting Accurate Detection of Sleep Apnea Using A Bed Sheet-Type Portable MonitorNadhifa TrivandariNo ratings yet
- Datasheet Actwatch PhilipsDocument4 pagesDatasheet Actwatch PhilipsNos Sos Bi ChosNo ratings yet
- Back Massage Intervention For Improving Health and Sleep Quality Among Intensive Care Unit PatientsDocument7 pagesBack Massage Intervention For Improving Health and Sleep Quality Among Intensive Care Unit PatientsيوكيNo ratings yet
- The Athlete Sleep Screening Questionnaire A New Tool For Assessing and Managing Sleep in Elite AthletesDocument6 pagesThe Athlete Sleep Screening Questionnaire A New Tool For Assessing and Managing Sleep in Elite AthletesKapibar BukartykNo ratings yet
- Aromatherapy On InsomniaDocument8 pagesAromatherapy On InsomniaJacob KuperstokNo ratings yet
- HHS Public Access: Sleep in Adolescence: Physiology, Cognition and Mental HealthDocument16 pagesHHS Public Access: Sleep in Adolescence: Physiology, Cognition and Mental Healthguidance mtisiNo ratings yet
- Stepanski2003 Use of Sleep Hygiene in The Treatment of InsomniaDocument11 pagesStepanski2003 Use of Sleep Hygiene in The Treatment of InsomniaM SNo ratings yet
- 9966 Cons enDocument225 pages9966 Cons enOmz DonNo ratings yet
- Jurnal 6Document21 pagesJurnal 6dwi putri ratehNo ratings yet