Download as pdf or txt
You might also like
- Abc BSN 4y1-1 Week 9 Course TaskDocument1 pageAbc BSN 4y1-1 Week 9 Course TaskHannah BalunanNo ratings yet
- Healthier Lifestyle, Behaviour ChangeDocument4 pagesHealthier Lifestyle, Behaviour ChangeupelworopezaNo ratings yet
- Perceptions, Attitudes, and Behaviors of Primary Care Providers Toward Obesity Management: A Qualitative StudyDocument18 pagesPerceptions, Attitudes, and Behaviors of Primary Care Providers Toward Obesity Management: A Qualitative StudyFitriani WidyastantiNo ratings yet
- Assessment of Provider Adherence To Obesity Treatment GuidelinesDocument9 pagesAssessment of Provider Adherence To Obesity Treatment Guidelinescheng yangNo ratings yet
- Do Practice Nurses Have The Knowledge To Provide Diabetes Self-Management Education?Document9 pagesDo Practice Nurses Have The Knowledge To Provide Diabetes Self-Management Education?Macarena MartínezNo ratings yet
- Nutrients 12 02208Document23 pagesNutrients 12 02208Peace Benyapa LeewiwatwongNo ratings yet
- Assessing The ProblemDocument10 pagesAssessing The ProblemKeyvoh KeymanNo ratings yet
- Does Orthodontic Treatment Harm Children's DietsDocument6 pagesDoes Orthodontic Treatment Harm Children's DietsNaliana LupascuNo ratings yet
- Preventive Medicine Reports: Kristina Walsh, Carol Grech, Kathy HillDocument10 pagesPreventive Medicine Reports: Kristina Walsh, Carol Grech, Kathy Hillnovi tasariNo ratings yet
- DiscussionDocument7 pagesDiscussionnick oringoNo ratings yet
- Nursing Agency To Improve Compliance, Self-Care Agency (Sca) andDocument23 pagesNursing Agency To Improve Compliance, Self-Care Agency (Sca) andWisnu KhawirianNo ratings yet
- Nutritional AssessmentDocument8 pagesNutritional AssessmentOutour KhNo ratings yet
- Adoption and Appropriateness of Mhealth For Weight Management in The Real World: A Qualitative Investigation of Patient PerspectivesDocument9 pagesAdoption and Appropriateness of Mhealth For Weight Management in The Real World: A Qualitative Investigation of Patient PerspectivesAli AhmedNo ratings yet
- Mona Mohamed Ibrahim Paper 13-12-2020Document19 pagesMona Mohamed Ibrahim Paper 13-12-2020mclinelkumahNo ratings yet
- Obesity Medicine: Original ResearchDocument6 pagesObesity Medicine: Original ResearchKate MossNo ratings yet
- Impact of Continuing Medical Education For PrimaryDocument12 pagesImpact of Continuing Medical Education For Primaryxp7jmnh5rpNo ratings yet
- 1 s2.0 S2213076418300654 MainDocument5 pages1 s2.0 S2213076418300654 MaindaytdeenNo ratings yet
- Standards of Medical Care in Diabetesd2019Document6 pagesStandards of Medical Care in Diabetesd2019EirNo ratings yet
- Paper 2Document10 pagesPaper 2Francisco Javier Luza RamosNo ratings yet
- A Trial Examining An Advanced Practice Nurse Intervention To Promote Medication Adherence and Symptom Management in Adult Cancer Patients Prescribed Oral Anti-Cancer Agents - Study ProtocolDocument12 pagesA Trial Examining An Advanced Practice Nurse Intervention To Promote Medication Adherence and Symptom Management in Adult Cancer Patients Prescribed Oral Anti-Cancer Agents - Study ProtocolyawnerNo ratings yet
- Obesity Diagnosis ManagementDocument26 pagesObesity Diagnosis ManagementAdán 'Olveera100% (1)
- Telaah Jurnal METPENDocument16 pagesTelaah Jurnal METPENaida fahleviNo ratings yet
- Attitude of Nurses Towards Diabetes CareDocument24 pagesAttitude of Nurses Towards Diabetes CareGemgem AcostaNo ratings yet
- Nihms 1792804Document18 pagesNihms 1792804Diego Fidelli LopezNo ratings yet
- Transformational Leadership: Student's Name Institutional Affiliation Nursing Professor's Name DateDocument5 pagesTransformational Leadership: Student's Name Institutional Affiliation Nursing Professor's Name DateTrevis ChrispinNo ratings yet
- Literature Review of Overweight and Obese Children and Adults RevisionDocument11 pagesLiterature Review of Overweight and Obese Children and Adults RevisionIlyas BalochNo ratings yet
- Nihms 999651Document17 pagesNihms 999651MUHAMMAD FARIS SASMANNo ratings yet
- BMC Health Services ResearchDocument12 pagesBMC Health Services ResearchpsmabbuttNo ratings yet
- Physician Response To Pay-For-Performance: Evidence From A Natural ExperimentDocument17 pagesPhysician Response To Pay-For-Performance: Evidence From A Natural ExperimentATYPICAL MEDIOCRITYNo ratings yet
- Are Doctors Nutritionists? What Is The Role of Doctors in Providing Nutrition Advice?Document6 pagesAre Doctors Nutritionists? What Is The Role of Doctors in Providing Nutrition Advice?Hilya SalmaNo ratings yet
- 447 Mod 3 DQ Replies - EditedDocument3 pages447 Mod 3 DQ Replies - EditedprinceNo ratings yet
- Jurnal Self Management DM Literacy 4Document8 pagesJurnal Self Management DM Literacy 4Rifa AinunNo ratings yet
- Obesity and Nutrition Epidemiology: A Study of Cause and EffectDocument9 pagesObesity and Nutrition Epidemiology: A Study of Cause and EffectNoob KidNo ratings yet
- Foundations of Care: Education, Nutrition, Physical Activity, Smoking Cessation, Psychosocial Care, and ImmunizationDocument11 pagesFoundations of Care: Education, Nutrition, Physical Activity, Smoking Cessation, Psychosocial Care, and ImmunizationrakolovaNo ratings yet
- AACE TOS ASMBS Clinical Practice Guidlines 3.2013 PDFDocument33 pagesAACE TOS ASMBS Clinical Practice Guidlines 3.2013 PDFJorge MariaNo ratings yet
- Dia Care 2002 Pastors 608 13Document6 pagesDia Care 2002 Pastors 608 13Isnar Nurul AlfiyahNo ratings yet
- Obesity 2019 AIMDocument17 pagesObesity 2019 AIMAndrea CorderoNo ratings yet
- Article IjpnDocument6 pagesArticle Ijpndr harrieNo ratings yet
- Chronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldDocument7 pagesChronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldHaneenNo ratings yet
- 2Document51 pages2Madhavan YadhavanNo ratings yet
- The Effect of Clinical Pathway Compliance On Reducing Length of StayDocument13 pagesThe Effect of Clinical Pathway Compliance On Reducing Length of StayRaipan RIFANSYAHNo ratings yet
- Challenges Faced by Canadian Primary Health Care Nurse Practitioners in Chronic Disease Management: A Qualitative Study Among Key InformantsDocument9 pagesChallenges Faced by Canadian Primary Health Care Nurse Practitioners in Chronic Disease Management: A Qualitative Study Among Key InformantsFedjine Neyssa LouisNo ratings yet
- Chronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldDocument7 pagesChronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldHaneenNo ratings yet
- Empowerment Program For People With Prediabetes: A Randomized Controlled TrialDocument13 pagesEmpowerment Program For People With Prediabetes: A Randomized Controlled TrialMittaningtyasNo ratings yet
- Evaluation & Synthesis of EvidenceDocument16 pagesEvaluation & Synthesis of EvidencebrillteckeNo ratings yet
- ObesityDocument9 pagesObesityTaoreed AdegokeNo ratings yet
- Management of Overweight and Obesity in Primary CareDocument13 pagesManagement of Overweight and Obesity in Primary CarezenNo ratings yet
- Impact of Weight Bias and Stigma On Quality of Care and Outcomes For Patients With ObesityDocument8 pagesImpact of Weight Bias and Stigma On Quality of Care and Outcomes For Patients With ObesityIsabella GrobérioNo ratings yet
- Obesity Medicine Rotation OMA HP Student Syllabus 4 WK Online RotationDocument9 pagesObesity Medicine Rotation OMA HP Student Syllabus 4 WK Online RotationWill HNo ratings yet
- EB001Document10 pagesEB001Giselle MillsNo ratings yet
- Adiposity Measurements and Non-Surgical Periodontal Therapy Outcomes.Document8 pagesAdiposity Measurements and Non-Surgical Periodontal Therapy Outcomes.yomiboyNo ratings yet
- Overview of Obesity Management in Primary Care: Big StoryDocument3 pagesOverview of Obesity Management in Primary Care: Big StoryLeyla MajundaNo ratings yet
- JOURNAL Where Is The Nurse in Nutritional CareDocument5 pagesJOURNAL Where Is The Nurse in Nutritional Carevia macarioNo ratings yet
- NURS FPX 6614 Assessment 1 Defining A Gap in PracticeDocument7 pagesNURS FPX 6614 Assessment 1 Defining A Gap in PracticeEmma WatsonNo ratings yet
- International Journal of Diabetes and Clinical Research Ijdcr 8 134Document7 pagesInternational Journal of Diabetes and Clinical Research Ijdcr 8 134Rio Raden Partotaruno TamaelaNo ratings yet
- Down 2020 5Document16 pagesDown 2020 5Marie GuajardoNo ratings yet
- Nrs 305Document15 pagesNrs 305Michael AlutaNo ratings yet
- Fitzpatrick 2016Document24 pagesFitzpatrick 2016Irsa SevenfoldismNo ratings yet
- Tsai2019 Obesity in The Clinic ACPDocument17 pagesTsai2019 Obesity in The Clinic ACPLuis RodriguezNo ratings yet
- Diabetes Individual CourseworkDocument25 pagesDiabetes Individual CourseworkKrizhel Mirja CawasNo ratings yet
- Benchmarking: - Process - People - Sample OutputDocument12 pagesBenchmarking: - Process - People - Sample Outputotis lynchNo ratings yet
- Value Based HealthcareDocument25 pagesValue Based HealthcareAkshay100% (2)
- Job Description: OsitionDocument2 pagesJob Description: OsitionSanjeev JayaratnaNo ratings yet
- Monica Utari Mariana LR 16.12Document8 pagesMonica Utari Mariana LR 16.12Bunda QueenaNo ratings yet
- National Clinical Guideline No. 5 Clinical Handover Nov2014Document306 pagesNational Clinical Guideline No. 5 Clinical Handover Nov2014Ahmad JuliadiNo ratings yet
- Disease Prevention and Control: Dr.K.Arulanandem Lecturer/CoordinatorDocument30 pagesDisease Prevention and Control: Dr.K.Arulanandem Lecturer/Coordinatorv_vijayakanth7656No ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaNatalia LeeNo ratings yet
- Leave Form 2019 HRHDocument17 pagesLeave Form 2019 HRHMonica BelloNo ratings yet
- Final Position Paper Group 8Document3 pagesFinal Position Paper Group 8secretNo ratings yet
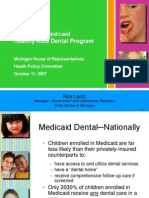
- Michigan's Medicaid Healthy Kids Dental Program: Rick LantzDocument16 pagesMichigan's Medicaid Healthy Kids Dental Program: Rick Lantz_RedX_No ratings yet
- BH Iqvia Event 2022Document108 pagesBH Iqvia Event 2022Irma BrkicNo ratings yet
- VT - Pharm Programs Handbook - 2019 - Final-2 (Somali) PDFDocument21 pagesVT - Pharm Programs Handbook - 2019 - Final-2 (Somali) PDFnimco haamud100% (1)
- Infection Prevention and Control ProgramsDocument2 pagesInfection Prevention and Control ProgramsAnonymous HSZMNq4100% (2)
- NHS England "PREVENT" Letter To CCGsDocument4 pagesNHS England "PREVENT" Letter To CCGsLeakSourceInfoNo ratings yet
- Key Health Challenges in GhanaDocument32 pagesKey Health Challenges in GhanaOwusu TjNo ratings yet
- Quality - Indicator - JAN'19 To JUNE'19Document12 pagesQuality - Indicator - JAN'19 To JUNE'19bodelevNo ratings yet
- Super Top Up - 211130 - 094009Document3 pagesSuper Top Up - 211130 - 094009Venkatesh SharmaNo ratings yet
- FHIR and Public HealthDocument70 pagesFHIR and Public HealthChandra Shekhar SenguptaNo ratings yet
- Chaman0302 ConsulDocument1 pageChaman0302 ConsulamanNo ratings yet
- BHLMP Form 1.b. Barangay Health System Development Six Building Block IndicatorsDocument20 pagesBHLMP Form 1.b. Barangay Health System Development Six Building Block IndicatorsLouieNo ratings yet
- Incidence (Epidemiology)Document3 pagesIncidence (Epidemiology)Muhammad Bilal SiddiquiNo ratings yet
- Basic Medicaid Eligibility Chart 2016 09 19Document3 pagesBasic Medicaid Eligibility Chart 2016 09 19Lydia CowartNo ratings yet
- Mguerrier Resume Final x1Document1 pageMguerrier Resume Final x1api-455033618No ratings yet
- Developing A Web PortalDocument2 pagesDeveloping A Web PortalolaNo ratings yet
- Cost Effectiveness Analysis (CEA) Rjyri 6umDocument15 pagesCost Effectiveness Analysis (CEA) Rjyri 6umYazeed Asrawi100% (1)
- Weebly Entry 4Document1 pageWeebly Entry 4api-479720222No ratings yet
- Healthcare GlossaryDocument18 pagesHealthcare GlossaryKalagara Mohan KrishnaNo ratings yet
- Allocation of Health Care ResourceDocument2 pagesAllocation of Health Care ResourceSha Btsta100% (1)
- FIGO Releases New Guidelines To Combat Pre-Eclampsia - FIGODocument4 pagesFIGO Releases New Guidelines To Combat Pre-Eclampsia - FIGOIgnasius HansNo ratings yet