Download as pdf or txt
You might also like
- Brown Sequard SyndromeDocument20 pagesBrown Sequard SyndromePutu Ariani100% (4)
- CI-03-Brain, Nerve, MuscleDocument4 pagesCI-03-Brain, Nerve, MuscleAna AzNo ratings yet
- CI-08 - Others Critical Illness (Lain-Lain Jenis Penyakit Kritikal)Document2 pagesCI-08 - Others Critical Illness (Lain-Lain Jenis Penyakit Kritikal)nur'afeefa binti hamdanNo ratings yet
- CI-08-Other Critical IllnessDocument2 pagesCI-08-Other Critical IllnessAna AzNo ratings yet
- Why Do We Fall Ill - Class-2 (Notes)Document7 pagesWhy Do We Fall Ill - Class-2 (Notes)Manju SharmaNo ratings yet
- (WG) Update in Trauma EmergenciesDocument31 pages(WG) Update in Trauma EmergencieswahyuekamaulyaniNo ratings yet
- ChronicDocument13 pagesChroniccesjopsNo ratings yet
- VBA-21-0960C-11-ARE Seizure Disorders Epilepsy PDFDocument4 pagesVBA-21-0960C-11-ARE Seizure Disorders Epilepsy PDFCombat CraigNo ratings yet
- Review - August 26Document9 pagesReview - August 26hrry stylesNo ratings yet
- Basic Cardio 3Document6 pagesBasic Cardio 3Malek ZanNo ratings yet
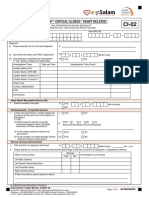
- Doctor'S Statement - Critical Illness - Heart Related CI-02: Heart Attack/ Myocardial Infarcion (MI)Document2 pagesDoctor'S Statement - Critical Illness - Heart Related CI-02: Heart Attack/ Myocardial Infarcion (MI)NUR AZIERANo ratings yet
- HMIS 033b - HEALTH UNIT WEEKLY EPIDEMIOLOGICAL New Edit 28.8.2019Document7 pagesHMIS 033b - HEALTH UNIT WEEKLY EPIDEMIOLOGICAL New Edit 28.8.2019OdetteNo ratings yet
- 1 s2.0 S1201971216310244 MainDocument2 pages1 s2.0 S1201971216310244 Mainnurahmi widyani ratriNo ratings yet
- Cefalea en Racimos Por DISECCION CAROTIDEADocument6 pagesCefalea en Racimos Por DISECCION CAROTIDEAFarid Santiago Abedrabbo LombeydaNo ratings yet
- Legal MedicineDocument7 pagesLegal MedicineEric CamposNo ratings yet
- CI 02 Heart RelatedDocument2 pagesCI 02 Heart RelatedSiti Rohani AhmadNo ratings yet
- Benefits For You and Your Family: 110 CI Care - 80Document3 pagesBenefits For You and Your Family: 110 CI Care - 80Raj RoyNo ratings yet
- Human DiseaseDocument8 pagesHuman Diseaseshubhamkashyap1020No ratings yet
- Transverse Myelitis AtfDocument3 pagesTransverse Myelitis AtfRishi VermaNo ratings yet
- ISU Ogrenci Klinik Uygulama Bakim Plani Degerlendirme DönüştürüldüDocument23 pagesISU Ogrenci Klinik Uygulama Bakim Plani Degerlendirme DönüştürüldüMerve kdkkNo ratings yet
- Lesson 1.2Document30 pagesLesson 1.2alialyasin21No ratings yet
- Orthopedic: OrthopaedicsDocument11 pagesOrthopedic: OrthopaedicsDrAyyoub AbboodNo ratings yet
- B. Immunosuppressive Therapy: Video 11Document9 pagesB. Immunosuppressive Therapy: Video 11Bianx Flores DosdosNo ratings yet
- 1 Health and DiseaseDocument21 pages1 Health and Disease47dp2mrvf4No ratings yet
- Hamza - 8.2Document10 pagesHamza - 8.2Jeff BezozNo ratings yet
- 1.2. Conditions of Diseases.: Category of Diseases Cause of Diseases Example of Diseases 1.) 2.)Document2 pages1.2. Conditions of Diseases.: Category of Diseases Cause of Diseases Example of Diseases 1.) 2.)Gantaal ShaakiyeNo ratings yet
- CRPSDocument8 pagesCRPSchinmayghaisasNo ratings yet
- Muscular Pathology: A. EpidemiologyDocument4 pagesMuscular Pathology: A. EpidemiologyRitz CelsoNo ratings yet
- Forensic Week 3 AssignmentDocument13 pagesForensic Week 3 Assignmentsayenshan0205No ratings yet
- Fibromyalgia Pathogenesis, Mechanisms, Diagnosis and Treatment Options UpdateDocument31 pagesFibromyalgia Pathogenesis, Mechanisms, Diagnosis and Treatment Options UpdateDiana F. MoscosoNo ratings yet
- 1618811695-HCS SCIENCE TECH TEST AnswerDocument9 pages1618811695-HCS SCIENCE TECH TEST AnswershagunNo ratings yet
- Human Health and DiseaseDocument33 pagesHuman Health and DiseaseJayashree JanarthanamNo ratings yet
- MeniningitaDocument3 pagesMeniningitaAlina Elisabeta Tiniuc căs LehaciNo ratings yet
- 141 - Neurology Pathology) Febrile Seizures - Etiology, Pathophysiology, Clinical Features, TreatmentDocument3 pages141 - Neurology Pathology) Febrile Seizures - Etiology, Pathophysiology, Clinical Features, TreatmentUssama MDNo ratings yet
- Prezentare Caz TCC (Engleza)Document20 pagesPrezentare Caz TCC (Engleza)stefania212No ratings yet
- Scs and C 201522Document5 pagesScs and C 201522noorhadi.n10No ratings yet
- Herpes Z Oster Clinical PresentationDocument50 pagesHerpes Z Oster Clinical PresentationS KkNo ratings yet
- Grand RevalidaDocument342 pagesGrand RevalidaJoeNo ratings yet
- Materi Webinar Morfin MartinDocument70 pagesMateri Webinar Morfin Martinfatma watiNo ratings yet
- CPAT3201 2020 Inflammation Lecture 1 NOTESDocument50 pagesCPAT3201 2020 Inflammation Lecture 1 NOTESJoshua KaoNo ratings yet
- Enumerate The Aetiological Agents of Meningeal Involvement in ChildrenDocument21 pagesEnumerate The Aetiological Agents of Meningeal Involvement in ChildrenAbhirup BoseNo ratings yet
- A Child With An Epileptic Status With Growth FalteringDocument25 pagesA Child With An Epileptic Status With Growth FalteringHasan HusienNo ratings yet
- Konsep Nyeri - Dr. SusiloDocument18 pagesKonsep Nyeri - Dr. Susilotendri ayuNo ratings yet
- Burns ActvityDocument8 pagesBurns ActvityMylene MiguelNo ratings yet
- Community Nursing Wound Care PresentationDocument56 pagesCommunity Nursing Wound Care PresentationkugernnesNo ratings yet
- Wa0003.Document8 pagesWa0003.pranesh premkumarNo ratings yet
- Management of Poly Traumatized Patient-1Document20 pagesManagement of Poly Traumatized Patient-1Taha Al-morsiNo ratings yet
- Supportive Care 2Document53 pagesSupportive Care 2Jared A. LangNo ratings yet
- Disease, Sickness & Illness: We May Distinguish 3 Levels That Describe What A Patient ExperiencesDocument1 pageDisease, Sickness & Illness: We May Distinguish 3 Levels That Describe What A Patient ExperiencessNo ratings yet
- Disease, Sickness, Illness PDFDocument1 pageDisease, Sickness, Illness PDFKaterina AntonNo ratings yet
- TraumaDocument8 pagesTraumaA HNo ratings yet
- 0052 - Kadek Diana Susilawati - LP Luka BakarDocument11 pages0052 - Kadek Diana Susilawati - LP Luka BakarDiana IdNo ratings yet
- Emergency Nursing CompleteDocument9 pagesEmergency Nursing CompleteggukNo ratings yet
- ERDNDocument9 pagesERDNggukNo ratings yet
- 4.2 MDS01 - Definition Table of The MDS Items - Ver0.94Document7 pages4.2 MDS01 - Definition Table of The MDS Items - Ver0.94AriniDwiLestariNo ratings yet
- FUO-6th Year MedicineDocument25 pagesFUO-6th Year MedicineananNo ratings yet
- MedCosmos Surgery - History TakingDocument18 pagesMedCosmos Surgery - History TakingEmmanuel DanielsNo ratings yet
- Transverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandTransverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (1)
- Case Study For Pancreas SurgeryDocument5 pagesCase Study For Pancreas SurgeryAARIFA QADRINo ratings yet
- Hematologic DisordersDocument72 pagesHematologic DisordersKEFELEGN ZNo ratings yet
- Case Study - Multiple SclerosisDocument3 pagesCase Study - Multiple SclerosisRachel KoenigsonNo ratings yet
- MalnutrionDocument44 pagesMalnutrionnajeebNo ratings yet
- Basic Concepts and Principles of EpidemiologyDocument137 pagesBasic Concepts and Principles of EpidemiologyShubhamNo ratings yet
- Duchenne Muscular Dystrophy Fact SheetDocument3 pagesDuchenne Muscular Dystrophy Fact SheetRakesh GurrapuNo ratings yet
- NCP (Acute Pain)Document2 pagesNCP (Acute Pain)jennilois100% (1)
- Somatic Symptom Disorder: Placer, Selorio & VuelgaDocument52 pagesSomatic Symptom Disorder: Placer, Selorio & Vuelgacarsheen claireNo ratings yet
- Defining and Diagnosing SepsisDocument9 pagesDefining and Diagnosing SepsisEdwin AlvarezNo ratings yet
- Trigger Finger Faq 1) What Is Trigger Finger?Document1 pageTrigger Finger Faq 1) What Is Trigger Finger?Lasiaf AlaskaNo ratings yet
- Toxoplasmosis Serologic Testing AlgorithmDocument1 pageToxoplasmosis Serologic Testing AlgorithmHanny Prasetiana YuriantiNo ratings yet
- Kenya ARV Guidelines 2022 - 230105 - 142032Document287 pagesKenya ARV Guidelines 2022 - 230105 - 142032islam media100% (1)
- Assignment InstructionsDocument3 pagesAssignment InstructionsRobert AgumbaNo ratings yet
- HTPDocument4 pagesHTPAlyssa Jade SandovalNo ratings yet
- MCE Cambridge Primary Science 2E Stage6 SOW and LP C03Document32 pagesMCE Cambridge Primary Science 2E Stage6 SOW and LP C03Ala' ShehadehNo ratings yet
- The ConjunctivaDocument63 pagesThe ConjunctivaMariam QaisNo ratings yet
- TB Flipchart RSDocument30 pagesTB Flipchart RSMuhammad Hasbul100% (1)
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsArun Kumar U NNo ratings yet
- Edward Tidyman NursingDocument8 pagesEdward Tidyman Nursingyinghua guoNo ratings yet
- Peter Ho - Research PapersDocument9 pagesPeter Ho - Research Papersapi-581223483No ratings yet
- Dehydration: By: M. SofyanDocument2 pagesDehydration: By: M. Sofyansofyan novrizalNo ratings yet
- Edukasi Gizi Pada Ibu Hamil Mencegah Stunting Pada Kelas Ibu HamilDocument8 pagesEdukasi Gizi Pada Ibu Hamil Mencegah Stunting Pada Kelas Ibu HamilDella OktaviantiNo ratings yet
- Insomnia Severity IndexDocument2 pagesInsomnia Severity IndexFurinsuka MoriNo ratings yet
- Dermatologic Therapy Volume Issue 2020 (Doi 10.1111 - dth.13488) Keeling, Elizabeth Daly, Selene McKenna, Dermot B. - Dermatology Patientsâ - Knowledge and Concerns Regarding Their ImmunomodulatoryDocument8 pagesDermatologic Therapy Volume Issue 2020 (Doi 10.1111 - dth.13488) Keeling, Elizabeth Daly, Selene McKenna, Dermot B. - Dermatology Patientsâ - Knowledge and Concerns Regarding Their ImmunomodulatoryJoNo ratings yet
- Pe 9 q1 w1 Answer KeyDocument8 pagesPe 9 q1 w1 Answer KeyRAYMOND ADLAONNo ratings yet
- CASE 2 Substance Induced PsychosisDocument7 pagesCASE 2 Substance Induced PsychosisDezy ShuklaNo ratings yet
- Rekap JR Ppds DV Update Mei 2023Document75 pagesRekap JR Ppds DV Update Mei 2023Katarina ZhongNo ratings yet
- Jurnal CampakDocument9 pagesJurnal CampakbadliinaaNo ratings yet
- Mr. Dasari A. LinconDocument3 pagesMr. Dasari A. LinconMEDICAL REPORTINGNo ratings yet
- LAS - MELC 4 - Writing Effective ParagraphsDocument3 pagesLAS - MELC 4 - Writing Effective ParagraphsKyline Chrizeiah Bautista ChiuNo ratings yet