Download as pdf or txt
You might also like
- Argelander Initial InterviewDocument13 pagesArgelander Initial InterviewTiborNo ratings yet
- Considerations For PO To IV Dose ConversionsDocument4 pagesConsiderations For PO To IV Dose ConversionsKeziah GillNo ratings yet
- Ern Baxter - Thy Kingdom ComeDocument20 pagesErn Baxter - Thy Kingdom ComeAussiedler77100% (1)
- Pt6a Engine Training OverwiewDocument20 pagesPt6a Engine Training OverwiewRafael Alves Dos Santos100% (1)
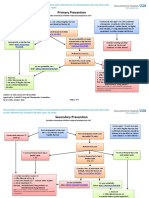
- AACE ACE 2016 Postmenopausal Osteoporosis Treatment Algorithm PDFDocument1 pageAACE ACE 2016 Postmenopausal Osteoporosis Treatment Algorithm PDFTabs NuñezNo ratings yet
- Giop Guideline Summary 2022Document7 pagesGiop Guideline Summary 2022adri20121989No ratings yet
- Glucocorticoid-Induced Osteoporosis: Insights For The ClinicianDocument10 pagesGlucocorticoid-Induced Osteoporosis: Insights For The ClinicianLucía del ValleNo ratings yet
- SDCEP Oral Health Management of Patients at Risk of MRONJ Guidance in BriefDocument6 pagesSDCEP Oral Health Management of Patients at Risk of MRONJ Guidance in BriefLupu AndreeaNo ratings yet
- Glucocorticoid-Induced Osteoporosis: Insights For The ClinicianDocument10 pagesGlucocorticoid-Induced Osteoporosis: Insights For The Clinicianarif fatkhurNo ratings yet
- Fracture Prevention Treatments Postmenopausal Women OsteoporosisDocument4 pagesFracture Prevention Treatments Postmenopausal Women Osteoporosisroby6No ratings yet
- OP Induced by GCsDocument5 pagesOP Induced by GCsjhonnyNo ratings yet
- Long-Term Outcome of Weekly Bisphosphonates: René Rizzoli, MDDocument5 pagesLong-Term Outcome of Weekly Bisphosphonates: René Rizzoli, MDMatthew PhillipsNo ratings yet
- Cochrane Review Osteoporosis 2011Document9 pagesCochrane Review Osteoporosis 2011Sex & Gender Women's Health CollaborativeNo ratings yet
- Bisphosphonate Treatment Break Guidance June 2017Document2 pagesBisphosphonate Treatment Break Guidance June 2017Usman Zafar QaziNo ratings yet
- Top 5 Corticosteroids For Use in Emergency SettingsDocument4 pagesTop 5 Corticosteroids For Use in Emergency SettingsIulian Cătălin GrămadăNo ratings yet
- Drugs For Bone Disorders CompleteDocument18 pagesDrugs For Bone Disorders CompleteOmar AbdullahiNo ratings yet
- Advancesinthetreatment Ofmultiplesclerosis: Carolyn Goldschmidt,, Marisa P. McginleyDocument13 pagesAdvancesinthetreatment Ofmultiplesclerosis: Carolyn Goldschmidt,, Marisa P. McginleyAsma Al-MahmoudNo ratings yet
- Respiratory MedicationDocument4 pagesRespiratory MedicationShang MacarayonNo ratings yet
- Breaking or Crushing TabletsDocument2 pagesBreaking or Crushing TabletsRahmaNo ratings yet
- Medical TherapyDocument6 pagesMedical Therapyvinay reddyNo ratings yet
- WRA0002Document32 pagesWRA0002kezia15rebeccaNo ratings yet
- Algorithm Based On Severity: Confirmed COVID Positive Admitted As InpatientDocument2 pagesAlgorithm Based On Severity: Confirmed COVID Positive Admitted As Inpatientsefigi6746No ratings yet
- Care Plan:, Wrong, Wrong, Wrong, WrongDocument8 pagesCare Plan:, Wrong, Wrong, Wrong, Wronglovelylife theNo ratings yet
- Management of Benzodiazepine Misuse and Dependence: Jonathan Brett Bridin MurnionDocument4 pagesManagement of Benzodiazepine Misuse and Dependence: Jonathan Brett Bridin MurnionLucius MarpleNo ratings yet
- Low Molecular Weigh Heparins Summary Prescribing Guide Version 14Document15 pagesLow Molecular Weigh Heparins Summary Prescribing Guide Version 14alexandr zinchenkoNo ratings yet
- Low Molecular Weight Heparins Summary Prescribing Guide Version 1.3Document14 pagesLow Molecular Weight Heparins Summary Prescribing Guide Version 1.3sharief145No ratings yet
- Dental Health GP PCDocument7 pagesDental Health GP PCMichael WallNo ratings yet
- MILV8N8Document4 pagesMILV8N8garywall.ukNo ratings yet
- Adult Policy For Intermittent Oral Opioid DosingDocument6 pagesAdult Policy For Intermittent Oral Opioid DosingQuestsNo ratings yet
- Ash Itp Pocket Guide For Web 1204Document5 pagesAsh Itp Pocket Guide For Web 1204Restu Annisa PutriNo ratings yet
- FerroussulfatedsDocument2 pagesFerroussulfatedsDayanaj OngNo ratings yet
- Ijce Id22 PDFDocument3 pagesIjce Id22 PDFSciRes LiteratureNo ratings yet
- Farmakoterapi Osteoporosis: Suharti K Suherman Dept. Farmakologi & Terapeutik FkuiDocument23 pagesFarmakoterapi Osteoporosis: Suharti K Suherman Dept. Farmakologi & Terapeutik FkuimeldrewbNo ratings yet
- BoneKEy Intro Osteoporosis TreatmentDocument13 pagesBoneKEy Intro Osteoporosis TreatmentKrishna Teja GummadiNo ratings yet
- B Is Phospho NatesDocument34 pagesB Is Phospho NatesGayathri RaveendranNo ratings yet
- DS 3 Ectopic PregnancyDocument2 pagesDS 3 Ectopic PregnancyJohn Kenley FerryNo ratings yet
- Advantages and Disadvantages of Oral Anticoagulants - UpToDateDocument2 pagesAdvantages and Disadvantages of Oral Anticoagulants - UpToDateMunkhjargal BatmunkhNo ratings yet
- Rivaroxaban PresentationDocument13 pagesRivaroxaban PresentationReem El-HusseinyNo ratings yet
- Opioid-BenzosTapering FlowchartDocument1 pageOpioid-BenzosTapering FlowchartjuanchibarberoismNo ratings yet
- UK Guideline 2020 220709Document8 pagesUK Guideline 2020 220709rnwkrnrnNo ratings yet
- Treatment of Thalassemia: Nadirah Rasyid Ridha Dasril DaudDocument30 pagesTreatment of Thalassemia: Nadirah Rasyid Ridha Dasril DaudIfah Inayah D'zatrichaNo ratings yet
- Ambrisentan: James E. FramptonDocument12 pagesAmbrisentan: James E. FramptonElden Kyle BillonesNo ratings yet
- WarfarinDocument1 pageWarfarinaismyp12No ratings yet
- Drug Study - Osteomyelitis - Dalangin Delos Santos Pajarillo RigatDocument6 pagesDrug Study - Osteomyelitis - Dalangin Delos Santos Pajarillo RigatQueenie SilvaNo ratings yet
- Osteoporosis Screening, Diagnosis, and Treatment Guideline: Last Guideline Approval: April 2019Document12 pagesOsteoporosis Screening, Diagnosis, and Treatment Guideline: Last Guideline Approval: April 2019Mia DangaNo ratings yet
- Bone Turnover Markers To Monitor Oral Bisphosphonate TherapyDocument6 pagesBone Turnover Markers To Monitor Oral Bisphosphonate Therapyhossein kasiriNo ratings yet
- Rituximab Tullus Kjeil 2021Document9 pagesRituximab Tullus Kjeil 2021Carmen MunteanNo ratings yet
- Drug Tab YheDocument6 pagesDrug Tab YhegeejeiNo ratings yet
- Osteoporosis GuidelineDocument3 pagesOsteoporosis Guidelinechendm123No ratings yet
- Strumazol Strong Iodine SolutionDocument5 pagesStrumazol Strong Iodine SolutionAisha MarieNo ratings yet
- Doacs For VteDocument10 pagesDoacs For VteAhmed MohammedNo ratings yet
- Polypharmacy: Guidance For Prescribing in Frail AdultsDocument6 pagesPolypharmacy: Guidance For Prescribing in Frail AdultsAgil BredlyNo ratings yet
- Medical Management of Osteoporosis in Menopausal WomenDocument11 pagesMedical Management of Osteoporosis in Menopausal WomenSiri DevarapalliNo ratings yet
- Prednisone Drug StudyDocument9 pagesPrednisone Drug StudyericcrizzawalingNo ratings yet
- HPAxis 3rd (Autosaved)Document29 pagesHPAxis 3rd (Autosaved)Jess PeltraNo ratings yet
- Asma 101Document43 pagesAsma 101Asfiksia NeonatorumNo ratings yet
- Guia Australiana de Perdida Masa Osea e Inhibidores AromatasaDocument6 pagesGuia Australiana de Perdida Masa Osea e Inhibidores AromatasaFrancisco Agustin CaballeroNo ratings yet
- DabigatranDocument25 pagesDabigatranNagesh JadavNo ratings yet
- Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Clinical Practice GuidelineDocument28 pagesPharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Clinical Practice GuidelineChon ChiNo ratings yet
- Ghid Tratament in Osteoporoza 2020Document28 pagesGhid Tratament in Osteoporoza 2020Simona ChiricăNo ratings yet
- MILsgsdgds VDocument4 pagesMILsgsdgds Vgarywall.ukNo ratings yet
- Trifluridine and TipiracilDocument3 pagesTrifluridine and TipiracilKristine AcasioNo ratings yet
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Roboshot Brochure enDocument19 pagesRoboshot Brochure envantuan17792No ratings yet
- Electrical Workshop EE-113: Prepared By: Engr. Shafaq EjazDocument53 pagesElectrical Workshop EE-113: Prepared By: Engr. Shafaq Ejazshafaq ejazNo ratings yet
- Paramahansa Yogananda - A TributeDocument7 pagesParamahansa Yogananda - A TributeDr Srinivasan Nenmeli -KNo ratings yet
- Accepted Manuscript: Journal of King Saud University - ScienceDocument8 pagesAccepted Manuscript: Journal of King Saud University - ScienceFajar HutagalungNo ratings yet
- Scientific Revolution: Galileo Galilei - Italian Mathematician in University of PaduaDocument6 pagesScientific Revolution: Galileo Galilei - Italian Mathematician in University of PaduaDaniel VasquezNo ratings yet
- Supplier Response Time: - Measured in Days/Hours - Better The Lowest SRTDocument6 pagesSupplier Response Time: - Measured in Days/Hours - Better The Lowest SRTJebin GeorgeNo ratings yet
- AssignmentDocument4 pagesAssignmentoolyrocksNo ratings yet
- Study Master Life Sciences Teachers Guide Grade 10 9781107380509ARDocument225 pagesStudy Master Life Sciences Teachers Guide Grade 10 9781107380509ARmiltonellkayNo ratings yet
- Past The Last Mountain 01 Paul AllorDocument23 pagesPast The Last Mountain 01 Paul AllorRalf Singh (Graphics)No ratings yet
- Electrolux EWW12753 7.5kg Washer 4.5kg Dryer Combo User ManualDocument40 pagesElectrolux EWW12753 7.5kg Washer 4.5kg Dryer Combo User ManualJohn Ray AbadNo ratings yet
- General Solution For The Dynamic Modeling of Parallel RobotsDocument17 pagesGeneral Solution For The Dynamic Modeling of Parallel RobotsHuynh TLoiNo ratings yet
- UntitledDocument136 pagesUntitledjhon rodriguezNo ratings yet
- Ethyl BenzeneDocument10 pagesEthyl Benzenenmmpnmmpnmmp80% (5)
- Soal UAS 2023 KELAS 9Document5 pagesSoal UAS 2023 KELAS 9MASDALYLA TINENDUNGNo ratings yet
- Simulation Methods Used To Analyze The Performance Ge Pg6541b Gas Turbine Utilizing Low Heating Value FuelsDocument10 pagesSimulation Methods Used To Analyze The Performance Ge Pg6541b Gas Turbine Utilizing Low Heating Value FuelsMike Erbes100% (1)
- Project On Production Process OFDocument15 pagesProject On Production Process OFtarun-neha100% (2)
- 196 5-95 PDFDocument12 pages196 5-95 PDFMurali Krish100% (6)
- Syllabus Vtu17scheme ECEDocument146 pagesSyllabus Vtu17scheme ECEsureshNo ratings yet
- Toxic Substances and Hazardous and Nuclear Wastes Control Act of 1990Document20 pagesToxic Substances and Hazardous and Nuclear Wastes Control Act of 1990Jeong100% (1)
- Pending Help Desk Sticker PastingDocument144 pagesPending Help Desk Sticker PastingnavavadhuvuNo ratings yet
- Counter Fort Retaining WallDocument3 pagesCounter Fort Retaining WalljosefNo ratings yet
- Astm G32 - 10Document19 pagesAstm G32 - 10ABINASH BEHERANo ratings yet
- Nursong ResponsibilitiesDocument4 pagesNursong ResponsibilitiesMichaela JapsayNo ratings yet
- Power System Lab QuizDocument2 pagesPower System Lab QuizVipin KumarNo ratings yet
- Shri Vishnu Panjar StotramDocument7 pagesShri Vishnu Panjar Stotramvicky168No ratings yet
- Replacing The Feeder Wheel Motor MaxFire and UBBDocument2 pagesReplacing The Feeder Wheel Motor MaxFire and UBBAl Malley50% (2)
- Network Security and Cryptography IIDocument114 pagesNetwork Security and Cryptography IIMohd AkbarNo ratings yet