Professional Documents
Culture Documents
1 Year Risk Corona-Comorbidities
1 Year Risk Corona-Comorbidities
Uploaded by
Elena BivolOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
1 Year Risk Corona-Comorbidities
1 Year Risk Corona-Comorbidities
Uploaded by
Elena BivolCopyright:
Available Formats
Articles
Estimating excess 1-year mortality associated with the
COVID-19 pandemic according to underlying conditions and
age: a population-based cohort study
Amitava Banerjee, Laura Pasea, Steve Harris, Arturo Gonzalez-Izquierdo, Ana Torralbo, Laura Shallcross, Mahdad Noursadeghi, Deenan Pillay,
Neil Sebire, Chris Holmes, Christina Pagel, Wai Keong Wong, Claudia Langenberg, Bryan Williams, Spiros Denaxas, Harry Hemingway
Summary
Background The medical, societal, and economic impact of the coronavirus disease 2019 (COVID-19) pandemic has Lancet 2020; 395: 1715–25
unknown effects on overall population mortality. Previous models of population mortality are based on death over Published Online
days among infected people, nearly all of whom thus far have underlying conditions. Models have not incorporated May 12, 2020
https://doi.org/10.1016/
information on high-risk conditions or their longer-term baseline (pre-COVID-19) mortality. We estimated the excess
S0140-6736(20)30854-0
number of deaths over 1 year under different COVID-19 incidence scenarios based on varying levels of transmission
Institute of Health Informatics
suppression and differing mortality impacts based on different relative risks for the disease. (A Banerjee DPhil, L Pasea PhD,
A Gonzalez-Izquierdo PhD,
Methods In this population-based cohort study, we used linked primary and secondary care electronic health records A Torralbo PhD, L Shallcross PhD,
Prof S Denaxas PhD,
from England (Health Data Research UK–CALIBER). We report prevalence of underlying conditions defined by Public
Prof H Hemingway FMedSci),
Health England guidelines (from March 16, 2020) in individuals aged 30 years or older registered with a practice Division of Infection and
between 1997 and 2017, using validated, openly available phenotypes for each condition. We estimated 1-year mortality Immunity
in each condition, developing simple models (and a tool for calculation) of excess COVID-19-related deaths, assuming (Prof M Noursadeghi PhD,
Prof D Pillay PhD), Clinical
relative impact (as relative risks [RRs]) of the COVID-19 pandemic (compared with background mortality) of 1·5, 2·0,
Operational Research Unit
and 3·0 at differing infection rate scenarios, including full suppression (0·001%), partial suppression (1%), mitigation (Prof C Pagel PhD), and Institute
(10%), and do nothing (80%). We also developed an online, public, prototype risk calculator for excess death estimation. of Cardiovascular Science
(Prof B Williams PhD),
University College London,
Findings We included 3 862 012 individuals (1 957 935 [50·7%] women and 1 904 077 [49·3%] men). We estimated that
London, UK; University College
more than 20% of the study population are in the high-risk category, of whom 13·7% were older than 70 years and London Hospitals NHS Trust,
6·3% were aged 70 years or younger with at least one underlying condition. 1-year mortality in the high-risk population London, UK (A Banerjee,
was estimated to be 4·46% (95% CI 4·41–4·51). Age and underlying conditions combined to influence background S Harris PhD, W K Wong PhD,
Prof B Williams); Barts Health
risk, varying markedly across conditions. In a full suppression scenario in the UK population, we estimated that there
NHS Trust, The Royal London
would be two excess deaths (vs baseline deaths) with an RR of 1·5, four with an RR of 2·0, and seven with an RR of Hospital, London, UK
3·0. In a mitigation scenario, we estimated 18 374 excess deaths with an RR of 1·5, 36 749 with an RR of 2·0, and (A Banerjee); Great Ormond
73 498 with an RR of 3·0. In a do nothing scenario, we estimated 146 996 excess deaths with an RR of 1·5, 293 991 with Street Hospital, London, UK
(Prof N Sebire PhD); University
an RR of 2·0, and 587 982 with an RR of 3·0. of Oxford, Oxford, UK
(Prof C Holmes PhD);
Interpretation We provide policy makers, researchers, and the public a simple model and an online tool for Alan Turing Institute, London,
understanding excess mortality over 1 year from the COVID-19 pandemic, based on age, sex, and underlying UK (Prof C Holmes,
Prof S Denaxas); MRC
condition-specific estimates. These results signal the need for sustained stringent suppression measures as well as Epidemiology Unit, University
sustained efforts to target those at highest risk because of underlying conditions with a range of preventive of Cambridge, Cambridge, UK
interventions. Countries should assess the overall (direct and indirect) effects of the pandemic on excess mortality. (C Langenberg PhD); University
College London Hospitals
National Institute for Health
Funding National Institute for Health Research University College London Hospitals Biomedical Research Centre, Research Biomedical Research
Health Data Research UK. Centre, London, UK
(Prof B Williams); and Health
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 Data Research UK, London, UK
(Prof S Denaxas,
license. Prof H Hemingway)
Correspondence to:
Introduction societal changes. One way of estimating and monitoring Dr Amitava Banerjee, Institute of
Excess deaths from the coronavirus disease 2019 excess mortality is to compare observed numbers of Health Informatics,
(COVID-19) pandemic might arise both in those infected deaths with those expected based on the background University College London,
London NW1 2DA, UK
(direct effects), as well as those affected (indirectly, not (pre-COVID-19) mortality risks in the population.1 ami.banerjee@ucl.ac.uk
infected) by altered access to health services; the physical, One model of the population mortality impact of
psychological, and social effects of distancing; and COVID-19 is based on age-stratified death rates over days
economic changes. Understanding the effect of COVID-19 in infected patients, but excludes prevalence of underlying
on mortality during this emergency requires modelling of conditions, their differing pre-COVID-19 background long-
an infectious disease, as well as wider medical and term mortality risks, or the additional risk associated with
www.thelancet.com Vol 395 May 30, 2020 1715
Articles
Research in context
Evidence before this study of impact of COVID-19 on health systems, and prevalence of
We searched PubMed, medRxiv, bioRxiv, arXiv, and Wellcome underlying conditions. We showed that in a full suppression
Open Research for peer-reviewed articles, preprints, and scenario, even if COVID-19 has high relative impact on health
research reports on mortality and comorbidities at baseline in systems, excess mortality over 1 year can be minimised.
coronavirus disease 2019 (COVID-19), using the search terms Conversely, with mitigation (ie, less rigorous and voluntary
“coronavirus”, “COVID-19”, and similar terms, and “mortality”, measures), we predict between 18 000 and 37 000 deaths.
up to March 21, 2020. We found no previous studies of excess We have provided a prototype risk calculator for the researchers
deaths due to the COVID-19 pandemic. Previous tools and and policy makers to make estimates and change the
models to estimate COVID-19-related deaths have not assumptions in the model. We also highlight the value of
considered the prevalence of underlying conditions, routine electronic health records and use of large, linked
background pre-COVID-19 mortality, long-term estimates, datasets at the country level in responding to the pandemic.
or the relative impact (relative risk) of COVID-19 on mortality.
Implications of all the available evidence
Without these data, it is challenging to predict and prepare
Our models allow the estimation of overall (direct and indirect)
health systems to respond to the COVID-19 health-care burden.
effects on excess mortality of the COVID-19 pandemic. For the
Added value of this study first time, we provide a model, a tool, and open-access data to
We produced a model to estimate the excess COVID-19-related individualise risk prediction across underlying conditions,
mortality by incorporating population infection rate in different which has clinical, public health, and research benefits for both
scenarios relating to degree of social isolation, differing degrees the COVID-19 pandemic and post-pandemic contexts.
COVID-19.2 Few reports of excess deaths beyond specific to be exposed) until March 23, 2020. Up to that date, people
high-risk populations have been published3,4 (most deaths were still in close proximity in work and public places.
have occurred in people with underlying health conditions Here, we provide estimates of 1-year mortality by
or those of older ages5–7). This situation is changing, with underlying conditions to understand the broader health
severe infections being treated in younger patients with impact of COVID-19. Our objectives were to provide the
COVID-19 who do not have underlying conditions.8 Case research and policy community and public with par
fatality rates for COVID-19 vary from 0·27% to 10%,9 ameters (prevalence and background pre-COVID-19
possibly explained by differing demography, testing strat 1-year mortality risk by age and underlying conditions) to
egies, and prevalence of underlying conditions. The UK assist modelling; and to provide initial estimates of the
has relatively high case fatality rates (8·2%), but mortality excess COVID-19-related deaths over a 1-year period
rates are unknown at this stage of the pandemic because based on differing rates and relative levels of impact of
testing is more common among sicker patients who are infection. We define COVID-19-related mortality as both
admitted to hospital (the context where most testing has direct and indirect effects of the pandemic.
been done) rather than milder cases. On April 14, the Office
for National Statistics reported 6000 excess deaths Methods
registered in the week March 28 to April 3, 2020, of which Study design and data sources
about 2500 deaths did not have COVID-19 recorded on the This was a population-based cohort study, done with
death certificates, providing the first indication of indirect clinical research using linked bespoke studies and
effects of the pandemic on mortality.10 electronic health records (CALIBER), an open research
Physical distancing and other strategies focus on high- platform with validated, reusable definitions of several
risk groups, with US Centers for Disease Control and hundred underlying conditions.14,15 It links electronic
Prevention specifying “older adults, and people who have health records from different data sources (via UK
serious chronic medical conditions such as heart disease, unique individual identification data and National Health
diabetes and lung disease”.11 On March 16, 2020, the UK Service [NHS] numbers), including primary care (Clinical
Government announced that particular subgroups are at Practice Research Datalink-GOLD), hospital care (Hospital
high risk from COVID-19,12 and recommended stringent Episodes Statistics), and death registry (Office of National
distancing measures, telling people how to stay away from Statistics). Nearly all (>99%) of the English population has
others. On March 22, 2020, the Government announced general practice registration. CALIBER has been shown to
that 1·5 million ”extremely vulnerable” people in England be representative of the general population in terms of
with underlying conditions (including severe chronic sociodemographic characteristics and overall mortality.
obstructive pulmonary disease [COPD]) should ”shield” Approval for the study was granted by the Independent
for 12 weeks, but did not explain how these conditions Scientific Advisory Committee (20_074R) of the Medicines
were selected.13 The UK Government did not implement and Healthcare products Regulatory Agency in the UK in
full suppression (during which only key workers are likely accordance with the Declaration of Helsinki.
1716 www.thelancet.com Vol 395 May 30, 2020
Articles
Study population number of underlying conditions. We then modelled the
Eligible individuals were aged 30 years or older and excess COVID-19-associated mortality for relative impact
registered with a general practice at any point between of mortality associated with COVID-19 (relative risk [RR]
Jan 1, 1997, and Jan 1, 2017, with at least 1 year of follow-up compared with background mortality) of 1·5, 2·0, and 3·021
data. Demographic characteristics (age, gender, index of at the infection rate consequences of different strategies:
multiple deprivation quintiles, and geographical region) full suppression (0·001%), partial suppression (1%),
and baseline characteristics (prevalence of underlying mitigation (10%), or do nothing (80%).22 Relative risk is a
conditions, risk factors, and medications) were recorded.14 comparison of risks or probabilities. For example, an RR
The overall population at high risk of COVID-19 and of 2·0 for COVID-19 describes a doubling of the risk of
recommended for physical distancing was defined as per mortality in individuals infected with or affected by
Public Health England guidance.12 COVID-19 versus their background risk of death. A
definition of COVID-19-related mortality relevant to the
Open national portal for definitions of underlying emergency includes both deaths among those infected
conditions (direct), and deaths among those affected by health service,
We used the Health Data Research (HDR) UK–CALIBER societal, and economic changes (indirect). Considering
open online portal to define underlying conditions from excess deaths in this way, it is reasonable to consider that a For the HDR UK–CALIBER online
records. The underlying conditions were defined using high proportion (eg, 80% of the population) might be portal see www.caliberresearch.
org/portal
Read codes in primary care and the International affected by the COVID-19 emergency. To extrapolate
Classification of Diseases 10th edition for hospital our estimates of excess deaths to the whole population of
admissions as per validated CALIBER pheno types.14 England older than 30 years, we used 2018 estimates of
Hypertension was defined on the basis of recorded overall population size and mortality.23 For illustration, we
values in primary care according to the most recent applied our study estimates to UN Population Fund24
guidelines (≥140 mm Hg systolic blood pressure [or estimates of population size in other countries. All analyses
≥150 mm Hg for people aged ≥60 years without were done using R, version 3.4.3. Data were analysed in
diabetes and chronic kidney disease] or ≥90 mm Hg the University College London ISO27001 safe haven.
diastolic blood pressure).16 Diabetes was defined at
baseline (including type 1, type 2, or uncertain type) on Role of the funding source
the basis of coded diagnoses recorded in Clinical Practice The funders of the study had no role in study design,
Research Datalink or Hospital Episode Statistics at or data collection, data analysis, data interpretation, or
before study entry.15 Severe obesity was defined as body- writing of the report. LP and SD had full access to all the
mass index of 40 kg/m² or more.16 Cardiovascular disease data in the study and AB and HH had final responsibility
was defined as the 12 most common symptomatic for the decision to submit for publication.
manifestations: chronic stable angina, unstable angina,
myocardial infarction, unheralded death from coronary Results
heart disease, heart failure, cardiac arrest or sudden We included 3 862 012 individuals aged 30 years or older.
coronary death, transient ischaemic attack, ischaemic 1 957 935 (50·7%) were women and 1 904 077 (49·3%)
stroke, intracerebral haemorrhage, subarachnoid haem
or
rhage, peripheral arterial disease, and abdominal
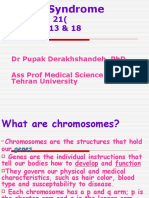
16 >70 years
aortic aneurysm, as per previous studies.15–17 COPD and
13·7% ≤70 years
chronic kidney disease were defined using previous 14
definitions.14–17 Multi
morbidity was defined as the co- 12
occurrence of two or more conditions in an individual.18
10
Prevalence (%)
Given recent interest in the potential roles of angiotensin-
converting enzyme (ACE) inhibitors19 and non-steroidal 8
inflammatory drugs (NSAIDs),20 we also estimated 6
prevalence of their use.
4
2·3% 2·2% 1·9%
Statistical analysis 2 0·9% 0·6% 0·5% 0·2% 0·01% 0·02% 0·005% 0·001%
To assess prevalent underlying conditions, we only 0
included records from the year before baseline (date of
0
py
g²
ns
DS
s
e
er
er
as
as
as
as
>7
k
et
tio
ra
AI
rd
rd
g/
se
se
ise
ise
ab
he
iso
iso
di
general practice registration or being aged >30 years
0m
di
di
or
yd
rd
Di
dt
on
ar
ed
V
ive
ne
ar
>4
HI
oi
ul
ic
lc
on
un
len
id
er
cl
during the 1997–2017 study period). Follow-up ceased at
sc
ca
ex
ck
St
m
va
ni
gi
Sp
nd
ro
ul
Im
io
lo
ni
si
ep
Ch
ro
rd
the date of death or on Jan 1, 2017. We estimated prevalence
ro
as
Ca
eu
Ch
tiv
-m
cn
uc
of each underlying condition and used Kaplan-Meier
dy
ni
tr
Bo
bs
ro
Ch
co
estimates of 1-year all-cause mortality at each age group
ni
ro
Ch
cell to estimate the number of excess deaths by age bands
and at each number of conditions cell to estimate by Figure 1: Prevalence of underlying conditions associated with high mortality in COVID-19 infection (n=3 862 012)
www.thelancet.com Vol 395 May 30, 2020 1717
Articles
were men; 3 331 280 (86·3%) were aged 70 years or (48·0 years [16·4]) and COPD (48·2 years [16·6]) 6·7%
younger (mean age 43·5 years [SD 11·7] in both sexes) without cardiovascular disease, 7·9% without diabetes,
and 530 732 (13·7%) were older than 70 years (mean age 9·1% without chronic kidney disease, and 9·7% without
78·1 years [6·1] in men and 80·2 years [7·0] in women; COPD still had a condition meeting criteria for physical
See Online for appendix appendix p 1). distancing. Hypertension was common: 7·4% in the
More than 20·0% of the study population had at least individuals aged 70 years or younger and 31·7% in those
one high-risk condition defined by Public Health England older than 70 years. In individuals aged 70 years or
guidelines. 13·7% were older than 70 years and 6·3% younger, prescription of ACE inhibitors was lower (3·7%)
were aged 70 years or younger with at least one underlying than in those older than 70 years (14·9%). 14·0% of those
condition (figure 1). Age-specific (5-year age bands) and aged 70 years or younger and 21·1% of those older than
sex-specific estimates of prevalence for each underlying 70 years were prescribed NSAIDs.
For the open-access repository condition are available online. Mortality at 1 year was estimated at 4·46% (95% CI
see https://doi.org/10.6084/ Multimorbidity was common (10·1%), especially 4·41–4·51) among individuals at high risk. 1-year
m9.figshare.12238118
with cardiovascular disease, diabetes, chronic kidney mortality was 8·62% (8·32–8·92) for those with COPD,
disease, and COPD (appendix p 2). In individuals without 7·84% (7·62–8·06) for those with chronic kidney
cardiovascular disease (mean age 47·5 years [SD 16·2]), disease, 6·37% (6·25–6·49) for those with cardiovas
diabetes (48·0 years [16·5]), chronic kidney disease cular disease, and 4·1% (4·0–4·2) for those with
n (%) Deaths 1 year all-cause
mortality % (95% CI)
Risk factors
Any risk factor 774 639 (20·1%) 33 549 4·46% (4·41–4·51)
Chronic obstructive pulmonary disease 35 006 (0·9%) 2900 8·62% (8·32–8·92)
Chronic kidney disease 59 397 (1·5%) 4501 7·84% (7·62–8·06)
Cardiovascular disease 159 069 (4·1%) 9820 6·37% (6·25–6·49)
Age >70 530 732 (13·7%) 30 529 5·88% (5·82–5·95)
Corticosteroid 105 978 (2·7%) 4599 4·49% (4·37–4·62)
Diabetes 111 668 (2·9%) 4399 4·12% (4·00–4·24)
Body-mass index >40 mg/kg2 31 173 (2·7%) 194 0·66% (0·57–0·75)
Number of risk factors
≥3 15 030 (0·4%) 1890 13·10% (12·55–13·65)
2 63 578 (1·6%) 4612 7·53% (7·32–7·74)
1 327 544 (8·5%) 11 073 3·51% (3·44–3·57)
0 3 455 860 (89·5%) 21 272 0·64% (0·64–0·65)
Overall population 3 862 012 (100%) 38 847 1·05% (1·04–1·06)
0 5 10 15
Figure 2: Baseline 1-year mortality in England according to underlying conditions (n=3 862 012)
1 year all-cause mortality risk %
0 5 10 15 20 25 30
Men Women
4·63% 2·77% 7·04% 8·94% 12·22% 15·00% 19·41% 28·72% 3·95% 6·53% 5·24% 8·08% 8·36% 10·73% 16·38% 26·01%
≥3
n=576 n=443 n=717 n=1004 n=1217 n=1281 n=1099 n=956 n=704 n=462 n=663 n=882 n=1109 n=1301 n=1191 n=1425
Number of underlying conditions
1·54% 3·50% 3·50% 4·85% 5·86% 9·02% 14·65% 24·04% 1·25% 1·06% 2·18% 3·12% 4·75% 6·71% 11·17% 20·41%
2
n=4683 n=2614 n=3511 n=4241 n=4558 n=4589 n=3235 n=2835 n=5687 n=2171 n=2858 n=3514 n=4136 n=4819 n=4261 n=5866
0·61% 1·21% 1·77% 2·45% 3·43% 5·52% 0·41% 0·91% 1·05% 1·74% 2·41% 3·80% 7·03% 17·14%
10·10% 19·08%
1 n= n= n= n= n= n= n= n= n= n= n= n= n= n=
n=9459 n=7887
53 898 15 705 17 413 17 189 16 725 14 592 62 059 13 309 14 512 15 092 16 577 18 027 15 163 19 937
0·12% 0·37% 0·64% 1·07% 1·71% 2·99% 5·96% 12·43% 0·07% 0·25% 0·44% 0·66% 1·12% 2·14% 4·47% 11·97%
0 n= n= n= n= n= n= n= n= n= n= n= n= n= n= n= n=
1 293 080 121 928 91 312 68 414 54 706 42 431 23 511 18 268 1 218 784 121 895 95 619 76 341 68 089 63 302 44 787 53 393
30–55 56–60 61–65 66–70 71–75 76–80 81–85 >85 30–55 56–60 61–65 66–70 71–75 76–80 81–85 >85
Age group (years) Age group (years)
Figure 3: Baseline 1-year mortality in England according to number of underlying conditions, age category, and sex (n=3 862 012)
1718 www.thelancet.com Vol 395 May 30, 2020
Articles
A Full suppression (0·001%) Absolute excess UK deaths
0 1000 5000 10 000 50 000 100 000 250 000
underlying conditions
0
Number of
RR 1·2
RR 1·5
Total excess deaths 1 Total excess deaths 2
2
≥3
underlying conditions
0
Number of
RR 2
RR 3
Total excess deaths 4 Total excess deaths 7
2
≥3
Partial supression (1%)
underlying conditions
0
Number of
1
RR 1·2
RR 1·5
Total excess deaths 735 Total excess deaths 1837
2
≥3
underlying conditions
0
Number of
1
RR 2
RR 3
Total excess deaths 3675 Total excess deaths 7 350
2
≥3
Mitigation (10%)
underlying conditions
0
Number of
1
RR 1·2
RR 1·5
Total excess deaths 7350 Total excess deaths 18 374
2
≥3
underlying conditions
0
Number of
1
RR 2
RR 3
Total excess deaths 36 749 Total excess deaths 73 498
2
≥3
Do nothing (80%)
underlying conditions
0
Number of
1
RR 1·2
RR 1·5
Total excess deaths 58 798 Total excess deaths 146 996
2
≥3
underlying conditions
0
Number of
1
Total excess deaths 293 991 Total excess deaths 587 982
RR 2
RR 3
≥3
5
5
0
0
–5
–6
–7
–8
>8
–5
–6
–7
–8
>8
–7
–8
–7
–8
–6
–6
71
71
30
30
66
66
61
81
61
81
76
76
56
56
Age group (years) Age group (years)
(Figure 4 continues on next page)
www.thelancet.com Vol 395 May 30, 2020 1719
Articles
B Full suppression (0·001%) Absolute excess UK deaths
0 1000 5000 10 000 50 000 100 000 250 000
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
underlying conditions
0
(0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0)
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Number of
RR 1·2
RR 1·5
(0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0)
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
2
(0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0)
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
≥3 (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0)
0 0 0 0 0 0 0 1 1 0 0 0 0 0 1 2
underlying conditions
0 (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0)
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1
Number of
1 (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0)
RR 2
RR 3
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
2 (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0)
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
≥3 (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0)
Partial supression (1%)
46 14 18 23 31 48 62 159 115 35 46 56 78 120 156 397
underlying conditions
0
(0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0·1)
11 6 8 13 18 27 37 90 27 14 21 31 45 68 93 226
Number of
1
RR 1·2
RR 1·5
(0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0·1)
3 2 3 6 9 14 17 34 7 5 8 14 21 34 44 86
2
(0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0) (0·1) (0·1)
1 1 2 3 4 6 7 12 2 2 4 7 11 15 19 30
≥3 (0) (0) (0) (0) (0) (0) (0) (0·1) (0) (0) (0) (0) (0·1) (0·1) (0·1) (0·1)
231 70 92 113 155 240 312 794 462 139 183 226 311 481 1171 1588
underlying conditions
0 (0) (0) (0) (0) (0) (0) (0) (0·1) (0) (0) (0) (0) (0) (0) (0·1) (0·2)
53 28 42 63 89 137 185 451 106 57 84 125 178 273 695 902
Number of
1 (0) (0) (0) (0) (0) (0) (0·1) (0·2) (0) (0) (0) (0) (0·1) (0·1) (0·2) (0·4)
RR 2
RR 3
13 10 17 29 43 68 87 172 26 21 34 58 85 135 327 344
2 (0) (0) (0) (0) (0·1) (0·1) (0·1) (0·2) (0) (0) (0·1) (0·1) (0·1) (0·2) (0·3) (0·4)
5 4 8 15 22 30 37 59 10 8 16 30 44 61 140 118
≥3 (0) (0) (0·1) (0·1) (0·1) (0·1) (0·2) (0·3) (0·1) (0·1) (0·1) (0·2) (0·2) (0·3) (0·4) (0·5)
Mitigation (10%)
462 139 183 226 311 481 624 1588 1155 348 458 565 777 1202 1560 3971
underlying conditions
0
(0) (0) (0) (0) (0) (0) (0·1) (0·2) (0) (0) (0) (0) (0·1) (0·1) (0·2) (0·6)
106 57 84 125 178 273 371 902 265 142 211 313 446 683 927 2256
Number of
1
RR 1·2
RR 1·5
(0) (0) (0) (0) (0·1) (0·1) (0·2) (0·4) (0) (0·1) (0·1) (0·1) (0·1) (0·2) (0·4) (0·9)
26 21 34 58 85 135 174 344 66 52 85 144 213 338 435 861
2
(0) (0) (0·1) (0·1) (0·1) (0·2) (0·3) (0·4) (0·1) (0·1) (0·1) (0·2) (0·3) (0·4) (0·6) (1·1)
10 8 16 30 44 61 75 118 25 19 39 74 111 152 187 296
≥3 (0·1) (0·1) (0·1) (0·2) (0·2) (0·3) (0·4) (0·5) (0·2) (0·2) (0·3) (0·4) (0·5) (0·6) (0·9) (1·4)
·
2310 696 916 1130 1553 2403 3120 7941 4619 1392 1831 2259 3107 4807 6240 15 883
underlying conditions
0
(0) (0) (0·1) (0·1) (0·1) (0·2) (0·5) (1·2) (0) (0·1) (0·1) (0·2) (0·3) (0·5) (1) (2·4)
530 284 422 626 892 1365 1853 4511 1061 568 · 844 1253 1784 2731 3706 9023
Number of
1 (0) (0·1) (0·1) (0·2) (0·3) (0·5) (0·8) (1·8) (0·1) (0·2) (0·3) (0·4) (0·6) (0·9) (1·6) (3·5)
RR 2
131 105 170 289 425 676 871 1722 262 209 340 578 850 1352 1742 3444 RR 3
2
(0·1) (0·2) (0·3) (0·4) (0·5) (0·8) (1·3) (2·2) (0·3) (0·5) (0·6) (0·8) (1·1) (1·6) (2·5) (4·3)
50 39 78 148 221 304 374 592 100 78 156 295 442 608 749 1183
≥3 (0·4) (0·5) (0·6) (0·9) (1) (1·3) (1·8) (2·7) (0·9) (0·9) (1·2) (1·7) (2·1) (2·6) (3·6) (5·4)
Do nothing (80%)
3695 1114 1465 1807 2485 3846 4992 12 706 9239 2785 3663 4518 6213 9614 12 480 31 765
underlying conditions
0
(0) (0) (0·1) (0·1) (0·2) (0·4) (0·8) (1·9) (0) (0·1) (0·2) (0·3) (0·6) (1) (2) (4·8)
849 454 676 1002 1427 2185 2965 7218 2122 1136 1689 2505 3568 5462 7413 18 046
Number of
1
RR 1·2
RR 1·5
(0·1) (0·2) (0·2) (0·3) (0·5) (0·7) (1·3) (2·8) (0·2) (0·4) (0·6) (0·8) (1·2) (1·8) (3·3) (7·1)
210 168 272 462 680 1081 1394 2755 524 419 679 1156 1700 2703 3484 6888
2
(0·2) (0·4) (0·5) (0·7) (0·9) (1·3) (2) (3·5) (0·6) (1) (1·2) (1·6) (2·1) (3·1) (5·1) (8·6)
80 62 125 236 354 487 599 947 200 155 313 590 885 1216 1497 2367
≥3 (0·7) (0·7) (1) (1·4) (1·7) (2·1) (2·9) (4·3) (1·7) (1·9) (2·5) (3·4) (4·1) (5·1) (7·1) (10·8)
18 477 5569 7325 9036 12 427 19 228 24 960 63 531 36 954 11 138 14 651 18 073 24 854 38 456 49 921 127 062
underlying conditions
0
(0·1) (0·2) (0·4) (0·7) (1·1) (2) (4) (9·7) (0·2) (0·5) (0·9) (1·4) (2·2) (4) (8) (19·3)
Figure 4: Estimated number 4243 2272 3378 5011 7137 10 923 14 825 36 091 8487 4545 6755 10 022 14 273 21 847 29 650 72 183
Number of
of excess deaths at 1 year in 1 (0·4) (0·9) (1·2) (1·7) (2·3) (3·7) (6·6) (14·1) (0·8) (1·7) (2·3) (3·4) (4·7) (7·3) (13·1) (28·3)
RR 2
RR 3
the UK at different infection 2 1048 838 1359 2312 3401 5407 6968 13 777 2096 1676 2717 4623 6802 10 813 13 935 27 554
(1·1) (1·9) (2·3) (3·3) (4·3) (6·3) (10·1) (17·3) (2·2) (3·8) (4·7) (6·5) (8·5) (12·5) (20·3) (34·5)
rates and relative risks for 400 311 626 1181 1769 2433 2994 4734 800 621 1252 2362 3538 4866 5989 9468
the impact of COVID-19 ≥3 (3·4) (3·7) (4·9) (6·8) (8·3) (10·3) (14·3) (21·7) (6·8) (7·5) (9·9) (13·7) (16·6) (20·6) (28·5) (43·4)
(A) Total deaths. (B) Detailed
5
5
0
0
–5
–6
–7
–8
>8
–5
–6
–7
–8
>8
–7
–8
–7
–8
breakdown of deaths across
–6
–6
71
71
30
30
66
66
61
81
81
61
76
76
56
56
different categories. Age group (years) Age group (years)
RR=relative risk.
1720 www.thelancet.com Vol 395 May 30, 2020
Articles
diabetes (figure 2). Among those older than 70 years,
General population High-risk group (millions) Baseline number
1-year mortality rates were 13·6% (12·9–14·3) for (millions) of deaths in
COPD, 11·5% (11·0–12·1) for chronic kidney disease, 1 year in
10·4% (10·1–10·7) for cardiovascular disease, and 8·9% high-risk group
(8·5–9·4) for diabetes in men and 12·3% (11·6–13·0) for Total Older than Older than 70 years or Total at high
COPD, 9·6% (9·3–10·0) for chronic kidney disease, 30 years 70 years younger with risk
underlying
10·6% (10·3–10·9) for cardiovascular disease, and 9·8% condition
(9·4–10·2) for diabetes in women.
Canada 37·06 23·44 3·22 1·48 4·70 209 732
We estimated baseline 1-year mortality risk by age
England 55·98 35·41 4·87 2·24 7·10 316 805
group, sex, and number of conditions, in the absence of
France 65·50 41·43 5·69 2·62 8·31 370 681
COVID-19 (figure 3). For example, a man aged 66–70 years
with no underlying high-risk conditions has a higher Germany 82·40 52·12 7·16 3·29 10·46 466 322
estimated 1-year mortality risk (1·07%) than a woman Italy 59·20 37·45 5·15 2·37 7·51 335 028
aged 56–60 years with one underlying condition (0·91%). Sweden 10·10 6·39 0·88 0·40 1·28 57 158
According to our online risk calculator, a 66-year-old UK 66·44 42·03 5·77 2·66 8·43 376 001
man with COPD has a 6·39% (95% CI 5·48–7·30) USA 329·10 208·17 28·60 13·16 41·76 1 862 459
baseline 1-year mortality risk; thus with 25 641 people in All assumptions are based on England (CALIBER) estimates of 63·25% of the total population older than 30 years,
England in this subgroup, we projected 1639 baseline 13·74% older than 70 years, 6·32% 70 years or younger with an underlying condition, and 20·06% total high-risk
group; and a 1-year mortality (Kaplan-Meier) for the total high-risk group of 4·46%.
deaths over 1 year. The model (if set to 10% infection rate
and RR 2·0) estimates 164 excess COVID-related deaths Table: Projected deaths in 1 year in high-risk group pre-COVID-19 infection across countries
over a year in that demographic category.
At COVID-19 prevalence of 10% (mitigation) and
80% (do nothing), we estimate the number of excess for policy makers, clinicians, and the public. Our results For our online risk calculator
deaths to be 18 374 (mitigation) and 146 996 (do nothing) support rigorous, sustained implementation of suppres prototype see http://covid19-
phenomics.org/
with an RR of 1·5; 36 749 (mitigation) and 293 991 (do sion measures.25
PrototypeOurRiskCoV.html
nothing) with an RR of 2·0; and 73 498 (mitigation) and With our definition of overall excess deaths, combining
587 982 (do nothing) with an RR of 3·0. Corresponding direct and indirect effects among those with and without
numbers of deaths at full suppression (0·001%) and infection, it is reasonable to consider that a high (eg, 80%)
partial suppression (1%) were two (full) and 1837 (partial) proportion of the population might be affected by the
with an RR of 1·5; four (full) and 3675 (partial) with an COVID-19 pandemic. We do not know what the relative
RR of 2·0; and seven (full) and 7350 (partial) with an RR impact of excess deaths from the COVID-19 pandemic
of 3·0 (figure 4). will be over a 1-year period in any country. However,
Extrapolating from our English sample to the whole UK clinical and societal concern internationally is that it is
population, we estimate 8·43 million people are in the not a regular seasonal flu. We show that if the pandemic
high-risk group, of whom 5·77 million are older than is associated with an RR of 1·5, then there will
70 years of age, and 2·66 million have one or more be 18 374 excess deaths in a mitigation scenario and
underlying condition and are 70 years or younger). Based 146 996 excess deaths in a do nothing scenario; compared
on the background (pre-COVID-19) 1-year mortality that with two deaths under a full suppression scenario. A
we observed in the CALIBER data of 4·46% for this group, doubling of the risk is worth considering because of
376 001 deaths would occur in the UK. Using these uncertainty regarding the actual risk associated with
estimates, numbers of people at high-risk other countries COVID-19 and mounting health-care burden around
were 4·70 million in Canada, 8·31 million in France, the world. This RR of 2·0 would result in 36 749 excess
10·46 million in Germany, 7·51 million in Italy, deaths in a mitigation scenario and 293 991 excess deaths
1·28 million in Sweden, and 41·76 million in the USA in a do nothing scenario.
(table). A major concern is that relative risks will rise in a
non-linear fashion with infection rates if health systems
Discussion become overwhelmed by critically ill patients. Thus, at
Using NHS records, we provide an initial population-based high infection rates, relative risks for excess mortality
study estimating plausible ranges of excess COVID-19- would almost certainly be much higher—and these
related mortality in England. We provide esti mates of non-linear interactions are a subject for further
the prevalence and background (pre-COVID-19) 1-year modelling. The impact of COVID-19 is likely to be much
mortality risks according to underlying conditions at dif greater if there is poor compliance with social isolation
ferent ages in women and men, sharing these estimates policies and low treatment and health-system capacity.
in online materials, and the disease definitions in the The RR of COVID-19 infection and the case fatality rate
HDR UK–CALIBER portal. These are major parameters in have been estimated,21 but the RR for mortality will
understanding the emergency, and the best source of better capture the impact of infection on individuals
estimates comes from electronic records, with implications and health systems. Even in the RR of 2·0 model, full
www.thelancet.com Vol 395 May 30, 2020 1721
Articles
suppression would lead to virtually no excess mortality, risk calculator might be relevant for clinicians to prioritise
because some patients with underlying conditions such patients.
would have died over a 1-year period regardless of the In England, 1·5 million individuals have been iden
COVID-19 outbreak. The prototype online risk calculator tified based on national health records as being extremely
allows exploration and visualisation of the age-specific, vulnerable to COVID-19 infection, on the basis of one of
sex-specific, and underlying condition-specific excess a wide range of factors (including pregnancy with
mortality under different assumptions. Near real-time serious heart disease, chemotherapy, solid organ
cause-specific mortality, as reported by the Office for transplants, and cystic fibrosis).12 These patients have
National Statistics, ideally on a weekly basis, will greatly been identified and are being individually supported
aid understanding of the direct and indirect impacts of (eg, with food parcels and medicine delivery) for the
the COVID-19 pandemic.10 Such information can inform life-changing intervention of 12 weeks of shielding. Such
timing of exit strategies from lockdown. In future policies, which require actionable knowledge across
analyses, the impact of the COVID-19 pandemic on multiple diseases have few, if any, historical precedents;
disease-specific health-care provision and use should be only countries with nationwide health-system data can
assessed. implement such policies. The list was probably designed
We have assumed the same impact (RR) of COVID-19 to identify patients who are most susceptible to infection
on excess mortality for each underlying condition—ie, it or have a degree of immunosuppression, which cannot
is the same for a patient with COPD or with morbid be quantified in a standardised way. The prognosis
obesity. Although a reasonable starting point, this research strategy initiative has previously made recom
assumption requires testing as empirical data become mendations for consistent approaches to understanding
available. An interaction between different comorbid prognosis across multiple diseases and clinical spe
ities almost certainly exists, meaning that some cialties, the importance of which is highlighted by the
combinations are worse than others, and this factor COVID-19 pandemic.27
needs to be investigated. We found that patients with conditions not on the
We used a 1-year time period because of concerns vulnerable patient list may be at as high or greater
regarding second waves of infection and the time mortality than those who are. For example, cardiovascular
needed for health services and the wider socioeconomic disease is not on the vulnerable patient list and has a
disruption to return to a new steady state. Complementary 1-year mortality of 6%; we found that the 1-year mortality
future analyses might usefully address the temporal risk of people with two or more conditions was 11%—
resolution (daily and weekly) of excess mortality estimates, but multiple morbidities co-occurring in the same
which are likely to change at different phases of the individual do not yet qualify as extremely vulnerable. A
epidemic; specifically to focus on the first 3 months, more systematic, transparent understanding is needed
extending to 2 years and beyond. of which underlying conditions are important for policy
We show that by Public Health England criteria, at least and patients. Further research is required to identify the
20% of the population falls within the high-risk mortality extent to which patients with other physical conditions,
category for COVID-19: 13·7% based on age older than frailty, and mental health conditions as well as those
70 years (an arbitrary cutoff) and a further 6·3% based on experiencing social exclusion (eg, homeless people and
having one or more underlying conditions. We show how intravenous drug users) might benefit from targeted
policy might consider age in combination with underlying interventions.
conditions. For example, a man aged 66–70 years with no We have deposited definitions of underlying conditions
underlying conditions, who is not currently considered relevant to COVID-19 in the HDR UK–CALIBER open
high risk, has a higher background 1-year mortality (1·07%) online portal. It is important for reproducible research
than that of a woman aged 56–60 years with one underlying in COVID-19 that different research groups within
condition (0·91%), who is considered high risk. and between countries use clinical information from
The underlying conditions that we report (cardiovascular electronic health records in consistent, transparent,
diseases, COPD, and diabetes) are known to already be and validated ways to define underlying conditions and
suboptimally managed before COVID-19, with missed the COVID-19 syndrome (electronic health record
opportunities for effective (secondary) preventive inter phenotypes). It has previously been shown that in
ventions common in many countries.26 With COVID-19 defining one disease—asthma—research groups com
pressures, these practical actions for clinicians might not bine clinical data in more than 60 different ways to reach
be addressed, and chronic disease management care a definition.28 However, few efforts have been made to
might deteriorate. Primary and secondary health-care harmonise definitions of diseases across national
workers have an important role in optimising guideline- electronic health records. To address the COVID-19
recommended management of underlying conditions pandemic, international efforts are needed to harmonise
to lower background risk, particularly if shielding or definitions of underlying conditions and the clinical
suppression measures are to be sustained over long syndrome and progression of COVID-19 infection using
periods—eg, 3 or more months. The prototype online routine clinical health records.
1722 www.thelancet.com Vol 395 May 30, 2020
Articles
We share age-specific (5-year age bands) and sex- linking data about causes and consequences of the
specific estimates of prevalence and 1-year mortality for emergency across sectors, including education, economy,
each underlying condition. These population-based esti and transport.
mates might be relevant for other countries, particularly We have presented our findings in a way that begins to
those in which population-based records are neither be understandable by the general public, because of calls
available nor accessible. As an illustration, we show for information that might be relevant to an individual’s
estimates of excess deaths in different countries if the risk—here defined by age, sex, and presence of an
background (pre-COVID-19) mortality from England underlying condition.1 No authoritative public-facing tools
were applied. It is known, based on disease-specific are yet available, but they might provide context, motivation,
registries, that mortality among people with underlying and support to comply with the multiple changes in daily
conditions differs between countries, but few studies living that shielding entails. Particularly over prolonged
using electronic health records compare outcomes across isolation, this could be important given concern about the
countries. In one study, the long-term mortality among practical ability of patients to maintain shielding.
patients who had survived a heart attack was broadly By contrast with the daily news feed in every country,
consistent across France, Sweden, the UK, and the USA,29 which reports the numbers of deaths (the numerator), we
suggesting that our findings might have international report a risk: numbers of deaths over 1 year divided by the
relevance. population who was at risk of dying. Among the public it
Like other researchers, we were able to access only a might not be widely appreciated that 1400 people die on
sample of relevant NHS data, covering 5% of the UK average every day in the UK at baseline (ie, before
population, excluding any detailed information from COVID-19).33 Of all those people dying within 1 year, it is
hospitals. Research is a key part of the COVID-19 likely that COVID-19 brings forward the death earlier in
response, and the UK Government is already acting to the year. In other words, there are competing causes for
increase publicly accountable access to NHS health the mortality.
and social care data to a large number of researchers, Our study has important limitations. The study was
clinicians, and policy makers nationwide. Currently developed over a 72-h period before posting the results on
researchers can access only small samples, in which March 22, 2020, the day before the UK Prime Minister
linkage to even simple data on hospital admissions announced lockdown. First, our models require further
requires multiple approvals and can take years. It is data for their development. Commonly, research using
impossible to access NHS data on the COVID-19 NHS data can take months, and even years, partly because
epidemic as a nationwide whole (it is fragmented by of the multiple steps in accessing such data for research.
primary and secondary care and across countries). Specifically, it is important to study a wider range of
Despite small networks for critical care,30 and coronary underlying conditions, a wider range of hospital and
disease,31 there are currently no national efforts to stream critical care admissions, linkage of primary care data to
real-time, actionable data on COVID-19 care and (non- nationally available information on COVID-19 testing,
fatal) outcomes. With public and Government support, linkage to richer, real-time hospital data, and use of
the NHS has an opportunity to mobilise its data to create nationwide NHS data. Second, we believe it is both a
a learning health system needed urgently for COVID-19, limitation and a strength that our model is simple and
in which high-quality clinical information is collected. supports public understanding. The assumptions we
A system like this would need to include measures of make can be tested as empirical data become available,
disease severity, which are often absent. Beyond the such as the Office for National Statistics data.10 There
COVID-19 pandemic, this system could have far- are many avenues for further modelling to better
reaching, long-term benefits for patient care by understand how to target different preventive interven
accelerating knowledge generation and application. tions. An (incomplete) list includes statistical (dynamic
We might have underestimated true 1-year mortality models, weekly rates of mortality, and competing risks),
risks because physical distancing policies might them public health (disease-specific data for high-risk and
selves influence the background mortality risks—people extremely vulnerable conditions, regional variation, social
might be less likely to access health and social care, and deprivation, and ethnicity), clinical (including hospital
physical isolation has in many previous studies been and critical care admissions), and health service factors
shown to be associated with the onset and progression of (including data on health-care workers and operational
cardiovascular and other diseases. Underlying diseases, features).
treatment, and health-care use need to be explored in Health-care professionals, like those involved in this
detail in the context of COVID-19. It is not known paper, are being redirected to provide priority clinical
whether sudden and systematic physical distancing,32 services during the emergency internationally. We
particularly if prolonged over months, has different believe an important aspect of emergency response is to
or additional health consequences from those reported support clinical academics to continue to contribute to
from earlier studies of isolation. Understanding how research into new preventive and treatment options, as
to mitigate the emergency will require accessing and they take on new service responsibilities.
www.thelancet.com Vol 395 May 30, 2020 1723
Articles
If the relative risk of COVID-19 on mortality over 1 year 5 WHO Emergency Committee. Statement on the second meeting of
were 1·2 (ie, the same magnitude as the winter vs summer the International Health Regulations (2005) Emergency Committee
regarding the outbreak of novel coronavirus (2019-nCoV). Geneva:
mortality excess) then the number of excess deaths would World Health Organization, Jan 30, 2020. https://www.who.int/
be zero when one in 100 000 individuals are infected (full news-room/detail/30-01-2020-statement-on-the-second-meeting-of-
the-international-health-regulations-(2005)-emergency-committee-
suppression scenario), 7350 when one in ten are infected regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed
(mitigate scenario), and 58 798 when eight in ten are April 16, 2020).
infected (do nothing scenario). However, if the relative risk 6 Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics
of patients dying in relation to COVID-19 in Italy. JAMA 2020;
is doubled to 2·0, then there would be 36 749 deaths in the published online March 23. DOI:10.1001/jama.2020.4683.
mitigation scenario and 293 991 deaths in the do nothing 7 Huang C, Wang Y, Li X, et al. Clinical features of patients infected
scenario. These results should inform targeting of those at with 2019 novel coronavirus in Wuhan, China. Lancet 2020;
395: 497–506.
highest risk for a range of preventive interventions.
8 Bialek S, Boundy E, Bowen V, et al. Severe outcomes among patients
Contributors with coronavirus disease 2019 (COVID-19)—United States,
AB conceived the research question. SD and HH obtained funding. February 12–March 16, 2020. MMWR Morb Mortal Wkly Rep 2020;
AB, LP, CL, SD, and HH designed the study and analysis plan. 69: 343–46.
SD, AG-I, AT, WKW, and NS prepared the data, including electronic 9 Oke J, Heneghan C. Global COVID-19 case fatality rates.
health record phenotyping in the CALIBER open portal. LP and AB did CEBM Research, April 6, 2020. https://www.cebm.net/global-covid-
the statistical analysis. AB and HH drafted the initial and final versions 19-case-fatality-rates/ (accessed April 16, 2020).
of the manuscript. All authors critically reviewed early and final versions 10 Office for National Statistics. Deaths registered weekly in England
of the manuscript. and Wales, provisional: week ending 3 April 2020. April 14, 2020.
https://www.ons.gov.uk/peoplepopulationandcommunity/
Declaration of interests birthsdeathsandmarriages/deaths/bulletins/
AB is supported by research funding from the National Institute for deathsregisteredweeklyinenglandandwalesprovisional/
Health Research (NIHR), British Medical Association, AstraZeneca, weekending3april2020#main-points (accessed April 17, 2020).
and UK Research and Innovation. All other authors declare no 11 US Centers for Disease Control and Prevention. Coronavirus disease
competing interests. 2019 (COVID-19). People who are at higher risk. April 15, 2020.
https://www.cdc.gov/coronavirus/2019-ncov/specific-groups/high-
Data sharing risk-complications.html (accessed April 16, 2020).
We will make available the estimates of age-specific, sex-specific,
12 Public Health England. Guidance on social distancing for everyone
and condition-specific prevalence and 1 year mortality estimates online, in the UK. March 30, 2020. https://www.gov.uk/government/
the electronic health record phenotypes via the HDR UK–CALIBER publications/covid-19-guidance-on-social-distancing-and-for-
online portal, and the online risk calculator. vulnerable-people/guidance-on-social-distancing-for-everyone-in-
the-uk-and-protecting-older-people-and-vulnerable-adults (accessed
Acknowledgments
April 16, 2020).
BW and HH are funded by the National Institute for Health Research
13 UK Government. Major new measures to protect people at highest
(NIHR) University College London Hospitals Biomedical Research Centre.
risk from coronavirus. March 21, 2020. https://www.gov.uk/
HH is supported by Health Data Research UK (HDR-UK; grant no government/news/major-new-measures-to-protect-people-at-
LOND1), which is funded by the UK Medical Research Council, highest-risk-from-coronavirus (accessed April 16, 2020).
Engineering and Physical Sciences Research Council, Economic and 14 Denaxas S, Gonzalez-Izquierdo A, Direk K, et al. UK phenomics
Social Research Council, Department of Health and Social Care (England), platform for developing and validating electronic health
Chief Scientist Office of the Scottish Government Health and Social Care record phenotypes: CALIBER. J Am Med Inform Assoc 2019;
Directorates, Health and Social Care Research and Development Division 26: 1545–59.
(Welsh Government), Public Health Agency (Northern Ireland), British 15 Kuan V, Denaxas S, Gonzalez-Izquierdo A, et al. A chronological
Heart Foundation, and Wellcome Trust. HH is also supported by the map of 308 physical and mental health conditions from 4 million
BigData@Heart Consortium, funded by the Innovative Medicines individuals in the English National Health Service.
Initiative-2 joint undertaking under grant agreement no 116074. This joint Lancet Digital Health 2019; 1: e63–77.
undertaking receives support from the EU’s Horizon 2020 research and 16 Rapsomaniki E, Timmis A, George J, et al. Blood pressure and
innovation programme and European Federation of Pharmaceutical incidence of twelve cardiovascular diseases: lifetime risks, healthy
Industries and Associations. This work was supported by an NIHR life-years lost, and age-specific associations in 1·25 million people.
Clinician Scientist award (CS-2016-007) to LS. NS is supported by NIHR Lancet 2014; 383: 1899–911.
Great Ormond Street Hospital Biomedical Research Centre and HDR-UK. 17 Pikoula M, Quint JK, Nissen F, Hemingway H, Smeeth L,
Denaxas S. Identifying clinically important COPD sub-types using
References data-driven approaches in primary care population based electronic
1 Spiegelhalter D. How much ‘normal’ risk does Covid represent? health records. BMC Med Inform Decis Mak 2019; 19: 86.
Medium, March 21, 2020. https://medium.com/wintoncentre/ 18 Hurst JR, Dickhaus J, Maulik PK, et al. Global Alliance for Chronic
how-much-normal-risk-does-covid-represent-4539118e1196 Disease researchers’ statement on multimorbidity. Lancet Glob Health
(accessed April 16, 2020). 2018; 6: e1270–71.
2 Ferguson NM, Laydon D, Nedjati-Gilani G, et al. Impact of 19 Bozkurt B, Kovacs R, Harrington R. HFSA/ACC/AHA statement
non-pharmaceutical interventions (NPIs) to reduce COVID-19 addresses concerns re: using RAAS antagonists in COVID-19.
mortality and healthcare demand. London: Imperial College, March 17, 2020. https://professional.heart.org/professional/
March 16, 2020. https://www.imperial.ac.uk/media/imperial- ScienceNews/UCM_505836_HFSAACCAHAstatement-addresses-
college/medicine/sph/ide/gida-fellowships/Imperial-College- concerns-re-using-RAAS-antagonists-in-COVID.jsp (accessed
COVID19-NPI-modelling-16-03-2020.pdf (accessed April 16, 2020). April 16, 2020).
3 WHO. Report of the WHO-China joint mission on coronavirus 20 US Food and Drug Administration. FDA advises patients on use
disease 2019 (COVID-19). Geneva: World Health Organization, of non-steroidal anti-inflammatory drugs (NSAIDs) for
Feb 16–24, 2020. https://www.who.int/docs/default-source/ COVID-19. March 19, 2020. https://www.fda.gov/drugs/drug-
coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf safety-and-availability/fda-advises-patients-use-non-steroidal-anti-
(accessed April 16, 2020). inflammatory-drugs-nsaids-covid-19(accessed April 16, 2020).
4 Yang J, Zheng Y, Gou X, et al. Prevalence of comorbidities in the 21 Baud D, Qi X, Nielsen-Saines K, Musso D, Pomar L, Favre G.
novel Wuhan coronavirus (COVID-19) infection: a systematic Real estimates of mortality following COVID-19 infection.
review and meta-analysis. Int J Infect Dis 2020; published online Lancet Infect Dis 2020; published online March 12. https://doi.org/
March 12. DOI:10.1016/j.ijid.2020.03.017. 10.1016/S1473-3099(20)30195-X.
1724 www.thelancet.com Vol 395 May 30, 2020
Articles
22 Lintern S. Coronavirus could kill half a million Britons and infect 28 Al Sallakh MA, Vasileiou E, Rodgers SE, Lyons RA, Sheikh A,
80% of UK population, government documents indicate. Davies GA. Defining asthma and assessing asthma outcomes using
The Independent, Feb 26, 2020. https://www.independent.co.uk/ electronic health record data: a systematic scoping review.
news/health/coronavirus-news-latest-deaths-uk-infection- Eur Respir J 2017; 49: 1700204.
flu-a9360271.html (accessed April 16, 2020). 29 Rapsomaniki E, Thuresson M, Yang E, et al. Using big data from
23 Office for National Statistics. Deaths by single year of age tables, health records from four countries to evaluate chronic disease
UK. Jan 17, 2020. https://www.ons.gov.uk/peoplepopulation outcomes: a study in 114 364 survivors of myocardial infarction.
andcommunity/birthsdeathsandmarriages/deaths/datasets/ Eur Heart J Qual Care Clin Outcomes 2016; 2: 172–83.
deathregistrationssummarytablesenglandandwalesdeathsbysingle 30 Harris S, Shi S, Brealey D, et al. Critical Care Health Informatics
yearofagetables (accessed April 16, 2020). Collaborative (CCHIC): data, tools and methods for reproducible
24 United Nations Population Fund. World population dashboard. research: a multi-centre UK intensive care database.
https://www.unfpa.org/data/world-population-dashboard (accessed Int J Med Inform 2018; 112: 82–89.
April 16, 2020). 31 Kaura A, Panoulas V, Glampson B, et al. Association of troponin
25 Cyranoski D. What China’s coronavirus response can teach the rest level and age with mortality in 250 000 patients: cohort study across
of the world. Nature 2020; 579: 479–80. five UK acute care centres. BMJ 2019; 367: l6055.
26 Yusuf S, Islam S, Chow CK, et al. Use of secondary prevention 32 Fenichel EP. Economic considerations for social distancing and
drugs for cardiovascular disease in the community in high-income, behavioral based policies during an epidemic. J Health Econ 2013;
middle-income, and low-income countries (the PURE study): 32: 440–51.
a prospective epidemiological survey. Lancet 2011; 378: 1231–43. 33 BBC News. Coronavirus: UK deaths double in 24 hours.
27 Hemingway H, Croft P, Perel P, et al. Prognosis research strategy March 14, 2020. https://www.bbc.co.uk/news/uk-51889957
(PROGRESS) 1: a framework for researching clinical outcomes. (accessed April 16, 2020).
BMJ 2013; 346: e5595.
www.thelancet.com Vol 395 May 30, 2020 1725
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Theraputic Guidelines Version 3 - 2019 PDFDocument163 pagesTheraputic Guidelines Version 3 - 2019 PDFPulkit Kinra83% (6)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Cardiologie MANUALDocument15 pagesCardiologie MANUALElena Bivol50% (12)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Overcoming Crystal Meth AddictionDocument356 pagesOvercoming Crystal Meth AddictionSarah Menz100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- "God's Hotel: A Doctor A Hospital, and A Pilgrimage Into The Heart of Medicine" by Victoria SweetDocument43 pages"God's Hotel: A Doctor A Hospital, and A Pilgrimage Into The Heart of Medicine" by Victoria Sweetwamu885No ratings yet
- Childhood Obesity OutlineDocument3 pagesChildhood Obesity Outlinemarisolwashere100% (2)
- CDC Girl 2-20Document1 pageCDC Girl 2-20Angelique NatalieNo ratings yet
- Anorectal Disease Presentatione 2Document91 pagesAnorectal Disease Presentatione 2kavindukarunarathnaNo ratings yet
- Oral Disease: Dental CariesDocument8 pagesOral Disease: Dental CariesAnna PruteanuNo ratings yet
- Developing A Hospital Disaster Risk Management Evaluation ModelDocument11 pagesDeveloping A Hospital Disaster Risk Management Evaluation ModelElena BivolNo ratings yet
- Conducting Feasibility Studies For Knowledge Based SystemsDocument14 pagesConducting Feasibility Studies For Knowledge Based SystemsElena BivolNo ratings yet
- 87 - Interim Report For Hospital Construction Feasibility Study - Overview and Analysis of The Health Care System Within KoreaDocument136 pages87 - Interim Report For Hospital Construction Feasibility Study - Overview and Analysis of The Health Care System Within KoreaElena BivolNo ratings yet
- 4.3a - Feasibility Study Revised Format v7. TB 26.3.15Document68 pages4.3a - Feasibility Study Revised Format v7. TB 26.3.15Elena BivolNo ratings yet
- 11+MS+1892 EtiopiaDocument7 pages11+MS+1892 EtiopiaElena BivolNo ratings yet
- Health Insurance Feasibility Study in Afghanistan: Phase One Summary FindingsDocument18 pagesHealth Insurance Feasibility Study in Afghanistan: Phase One Summary FindingsElena BivolNo ratings yet
- 3 Leadership Trends For 2021 You Can't Afford To Ignore - DDIDocument5 pages3 Leadership Trends For 2021 You Can't Afford To Ignore - DDIElena BivolNo ratings yet
- 2021 CHP FR EnglishDocument24 pages2021 CHP FR EnglishElena BivolNo ratings yet
- 2021 - CHP - at - English AustriaDocument24 pages2021 - CHP - at - English AustriaElena BivolNo ratings yet
- Thesis Ida Löfman PDFDocument66 pagesThesis Ida Löfman PDFElena BivolNo ratings yet
- Top 10 Public Health Challenges - Rivier AcademicsDocument2 pagesTop 10 Public Health Challenges - Rivier AcademicsElena BivolNo ratings yet
- Comprehensive Obesity ManagementDocument11 pagesComprehensive Obesity ManagementElena BivolNo ratings yet
- Literature-Review Infographic V01Document1 pageLiterature-Review Infographic V01Elena BivolNo ratings yet
- Glucose Abnormalities in Patients With Hepatitis C Virus InfectionDocument10 pagesGlucose Abnormalities in Patients With Hepatitis C Virus InfectionElena BivolNo ratings yet
- Science: Quarter 3 - Module 5Document29 pagesScience: Quarter 3 - Module 5Amara ValleNo ratings yet
- White Blood CellsDocument4 pagesWhite Blood Cells9786541238No ratings yet
- Lifebuoy CSRDocument11 pagesLifebuoy CSRJaspreet KaurNo ratings yet
- Mayasthenia Gravis NclexDocument47 pagesMayasthenia Gravis NclexKrishna SapkotaNo ratings yet
- Trisomy 13, 18 & 21Document72 pagesTrisomy 13, 18 & 21Dr.MohanNo ratings yet
- Grade5exam Sy20192020Document7 pagesGrade5exam Sy20192020Esra AngadNo ratings yet
- Essay On Health IssuesDocument9 pagesEssay On Health IssuesAreeba ZaidiNo ratings yet
- Radiactive Uses Group Assignment-1Document7 pagesRadiactive Uses Group Assignment-1Alexia AguilarNo ratings yet
- Eisenmenger Syndrome: Clinical DefinitionDocument3 pagesEisenmenger Syndrome: Clinical Definition22194No ratings yet
- AMR Action Plan - Role of AcademiaDocument55 pagesAMR Action Plan - Role of AcademiaShonit SharmaNo ratings yet
- Nursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationDocument5 pagesNursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationAubrey SungaNo ratings yet
- Covid-19 Memoir by OGDocument55 pagesCovid-19 Memoir by OGDr Olayinka OkeolaNo ratings yet
- 2014 Acute Hemorrhage and Blood Transfusions in Horses PDFDocument10 pages2014 Acute Hemorrhage and Blood Transfusions in Horses PDFCamila CalleNo ratings yet
- PneumoniaSystem DisorderDocument1 pagePneumoniaSystem DisorderAA DDNo ratings yet
- SN Week10 PDFDocument3 pagesSN Week10 PDFRajesh KumarNo ratings yet
- Cluster HeadacheDocument10 pagesCluster HeadacheEhsan ElahiNo ratings yet
- Scented Hand and Body Sanitizing Soap Using Oxalis Triangularis Fused With Salvia RosmarinusDocument22 pagesScented Hand and Body Sanitizing Soap Using Oxalis Triangularis Fused With Salvia RosmarinusApple Joy BuenNo ratings yet
- Epidemiology of Sarcopenia Prevalence, Risk FactoDocument9 pagesEpidemiology of Sarcopenia Prevalence, Risk FactoW Antonio Rivera MartínezNo ratings yet
- Digital COVID Certificate Certificat Digital CovidDocument2 pagesDigital COVID Certificate Certificat Digital CovidOrtim Smart MastersNo ratings yet
- Chapter 22Document23 pagesChapter 22Hamza ElmoubarikNo ratings yet
- 2 Myocardial Infarction Nursing Care Management and Study GuideDocument13 pages2 Myocardial Infarction Nursing Care Management and Study GuideQuijano Gpokskie100% (2)
- Urinary IncontinenceDocument66 pagesUrinary Incontinencedr_asaleh100% (1)
- Budget Fy22Document74 pagesBudget Fy22Gohar AhmadNo ratings yet