
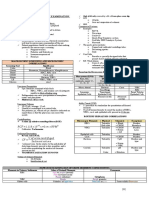
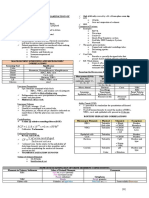
Bone Marrow Film Examination For Platelet Maturation Series: Activity No. 1
Bone Marrow Film Examination For Platelet Maturation Series: Activity No. 1
You might also like
- Blood Banking Lab Manual 3rdDocument7 pagesBlood Banking Lab Manual 3rdDanna Angelick ReyesNo ratings yet
- Med Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsDocument36 pagesMed Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsAshley100% (1)
- EMR Scenarios v2Document9 pagesEMR Scenarios v2Chris EnrightNo ratings yet
- Cc1-Task 4Document8 pagesCc1-Task 4Joshua TrinidadNo ratings yet
- Chapter 42Document3 pagesChapter 42Soc Gerren TuasonNo ratings yet
- AUBF Notes 1Document9 pagesAUBF Notes 1ChiNo ratings yet
- Clinical Chemistry: ToxicologyDocument9 pagesClinical Chemistry: ToxicologyChristine BadilloNo ratings yet
- Laboratory Activity 10: Osmotic Fragility Test (Oft)Document27 pagesLaboratory Activity 10: Osmotic Fragility Test (Oft)Marie LlanesNo ratings yet
- BSC Licensure Sample QuestionsDocument144 pagesBSC Licensure Sample QuestionsSAMMY0% (1)
- CC 2 Lab - Amylase and LipaseDocument7 pagesCC 2 Lab - Amylase and LipaseAngelaAmmcoNo ratings yet
- IMHM321 Lecture Trans 3Document9 pagesIMHM321 Lecture Trans 3Brix BrixNo ratings yet
- CC2 2Document13 pagesCC2 2Aedren TrillanaNo ratings yet
- Capillary Fragility/ Resistance Test: Tourniquet or Rumpel-Leede or Hess TestDocument4 pagesCapillary Fragility/ Resistance Test: Tourniquet or Rumpel-Leede or Hess TestGerly MaglangitNo ratings yet
- M6 Histopath ImpregantionAndEmbeddingDocument4 pagesM6 Histopath ImpregantionAndEmbeddingninaNo ratings yet
- Micropara Final LabNotesDocument75 pagesMicropara Final LabNotescream oNo ratings yet
- MEDT 19 (Lec)Document17 pagesMEDT 19 (Lec)Erick PanganibanNo ratings yet
- Chapter 3Document2 pagesChapter 3Rachel Marie M. Gania100% (1)
- Histopathologic Techniques by Gregorios Pages 257 269Document13 pagesHistopathologic Techniques by Gregorios Pages 257 269Desirie Rose LopenaNo ratings yet
- Compre-Quiz For MedtechDocument18 pagesCompre-Quiz For MedtechynaellyNo ratings yet
- 6 Ra 1517Document56 pages6 Ra 1517Jay Andrea Vea Dayuday-IsraelNo ratings yet
- Micro 1Document6 pagesMicro 1JOSSHUWA CASISNo ratings yet
- MT Laws and Lab ManDocument8 pagesMT Laws and Lab ManGene Narune GaronitaNo ratings yet
- Exercise 14: Macroscopic and Chemical Examination of UrineDocument11 pagesExercise 14: Macroscopic and Chemical Examination of UrineAfif PusamaniaNo ratings yet
- Carbohydrates StainsDocument43 pagesCarbohydrates StainssupahvyNo ratings yet
- 1 CCHM Trans LecDocument5 pages1 CCHM Trans LecCRUZ, ANNA MARIELLENo ratings yet
- Fresh Tissue Examination: Mark Lester B. Cauan, RMTDocument22 pagesFresh Tissue Examination: Mark Lester B. Cauan, RMTMarissa CordovaNo ratings yet
- Ra 5527Document14 pagesRa 5527Kai CulanagNo ratings yet
- Week 2 Chemical Examination of UrineDocument44 pagesWeek 2 Chemical Examination of UrineDayledaniel SorvetoNo ratings yet
- Red Cell suspensionRRL2020EDocument2 pagesRed Cell suspensionRRL2020EpixiedustNo ratings yet
- A Manual of Laboratory Techniques in Clinical Hematology 1Document15 pagesA Manual of Laboratory Techniques in Clinical Hematology 1Jaycel Mae Ba-ay (Gaikokujinn)No ratings yet
- Lab 2 - Microscopy and The CellDocument44 pagesLab 2 - Microscopy and The CellNatalie Pemberton100% (1)
- Post Lab 01-09Document7 pagesPost Lab 01-09Patrick ParconNo ratings yet
- Swu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisDocument7 pagesSwu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisTrex MarciiiNo ratings yet
- Exercise 5 Hematocrit DeterminationDocument7 pagesExercise 5 Hematocrit DeterminationJam RamosNo ratings yet
- RCS PreparationDocument3 pagesRCS PreparationMaria Charlene OrpillaNo ratings yet
- Mtle Bacte Revised 1Document35 pagesMtle Bacte Revised 1melvinsalonga2999No ratings yet
- Quality Assurance IN Histopathology: QC Should Consider The Whole ProcessDocument38 pagesQuality Assurance IN Histopathology: QC Should Consider The Whole Processalrasheed2020No ratings yet
- Micro TechniqueDocument2 pagesMicro Techniquehumanupgrade100% (1)
- BELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Document69 pagesBELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Sharon Agor0% (1)
- Lesson 5: Nature of The Clinical LaboratoryDocument8 pagesLesson 5: Nature of The Clinical LaboratoryJohn Daniel AriasNo ratings yet
- I. Aldehydes: Fixatives Advantages Disadvantages Formula Fixation Time Classifica TionDocument20 pagesI. Aldehydes: Fixatives Advantages Disadvantages Formula Fixation Time Classifica TionKaty RosNo ratings yet
- Stool Concentration MethodDocument2 pagesStool Concentration Methodqwshagdvndsavsb100% (1)
- Bleeding Time (Final)Document6 pagesBleeding Time (Final)Darwin Cañeso Balasta100% (1)
- 5 Hematologic-ExaminationsDocument12 pages5 Hematologic-ExaminationsMark Jireck AndresNo ratings yet
- Abo and MN Blood Group SystemDocument54 pagesAbo and MN Blood Group SystemAkram chaudaryNo ratings yet
- Doh DC 2018-0142Document2 pagesDoh DC 2018-0142vanceNo ratings yet
- HISTOTECHNIQUESDocument20 pagesHISTOTECHNIQUESZIPPORAH JESSICA NONOGNo ratings yet
- Fecalysis Form New 2021Document1 pageFecalysis Form New 2021GCMDHNo ratings yet
- Mtle - Hema 1Document50 pagesMtle - Hema 1Leogene Earl FranciaNo ratings yet
- MTLBE Internship Assessment QuizDocument2 pagesMTLBE Internship Assessment QuizAngela LaglivaNo ratings yet
- General Approach in Investigation of Haemostasis: Lecture 2: Bleeding TimeDocument28 pagesGeneral Approach in Investigation of Haemostasis: Lecture 2: Bleeding TimeClorence John Yumul FerrerNo ratings yet
- Antigen and Its PropertiesDocument20 pagesAntigen and Its Propertiestusharpremin92% (12)
- HTMLE SEMINAR NOTES DOC. ORTEGA - CompressedDocument35 pagesHTMLE SEMINAR NOTES DOC. ORTEGA - CompressedNISSI JUNE T. UNGABNo ratings yet
- Logic TechniquesDocument111 pagesLogic Techniquesdirenjan100% (1)
- CHALLENGE QUESTIONS (Write Your Answer/s Here For Practice)Document2 pagesCHALLENGE QUESTIONS (Write Your Answer/s Here For Practice)Roma Ann ManahanNo ratings yet
- CC1 Lab Fin V2Document22 pagesCC1 Lab Fin V2Melody PardilloNo ratings yet
- PopcornDocument41 pagesPopcorntrixia therese00No ratings yet
- Glucose MethodologiesDocument3 pagesGlucose MethodologiesprincessNo ratings yet
- Coombs TestDocument6 pagesCoombs TestjnsenguptaNo ratings yet
- The politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840From EverandThe politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840No ratings yet
- Holy Child Jesus Montessori: School of Dasmariñas, Incorporated S.Y.2020-2021Document2 pagesHoly Child Jesus Montessori: School of Dasmariñas, Incorporated S.Y.2020-2021pixiedustNo ratings yet
- Rarwardqaarmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwardqaarmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedust100% (1)
- Rarwrdrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrdrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- Rarwrdqaarmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrdqaarmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- Rarwrdqrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrdqrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- Rarwrrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- Rarwrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- GAS LAWS - QUIZ 1lolDocument1 pageGAS LAWS - QUIZ 1lolpixiedustNo ratings yet
- Nasugbu: Commission Slip Commission SlipDocument1 pageNasugbu: Commission Slip Commission SlippixiedustNo ratings yet
- Blood Components (E-Learning Activity) : Francisco, Frances Lorraine RDocument3 pagesBlood Components (E-Learning Activity) : Francisco, Frances Lorraine RpixiedustNo ratings yet
- TAC Street Medic 'ZineDocument9 pagesTAC Street Medic 'ZineTrish Mills100% (1)
- Ship Captain's Medical Guide - 22nd EdDocument224 pagesShip Captain's Medical Guide - 22nd EdcelmailenesNo ratings yet
- Initial Management of Moderate To Severe Hemorrhage in The Adult Trauma Patient - UpToDateDocument38 pagesInitial Management of Moderate To Severe Hemorrhage in The Adult Trauma Patient - UpToDateiustin loghinNo ratings yet
- Blood and Blood ProductsDocument52 pagesBlood and Blood Productswellawalalasith100% (1)
- First Aid and Basic Life Support and Water Safety - PPT 1Document21 pagesFirst Aid and Basic Life Support and Water Safety - PPT 1JM MillanesNo ratings yet
- Hemophilia and Von Willebrand Disease EmergenciesDocument13 pagesHemophilia and Von Willebrand Disease EmergenciesDobrila SimonovicNo ratings yet
- Samplex Aug2021-Dec2021Document162 pagesSamplex Aug2021-Dec2021Christian TayagNo ratings yet
- Hemostasis Dan Disseminated Intravascular Coagulation (DIC)Document14 pagesHemostasis Dan Disseminated Intravascular Coagulation (DIC)ErlinNo ratings yet
- ThrombocytopeniaDocument49 pagesThrombocytopeniaMaria EnjelinaNo ratings yet
- Transfusi BlokDocument96 pagesTransfusi BlokTutde SedanaNo ratings yet
- Angina Bullosa Hemorrhagica, An Uncommon Oral Disorder. Report of 4 CasesDocument5 pagesAngina Bullosa Hemorrhagica, An Uncommon Oral Disorder. Report of 4 CaseslitaakkNo ratings yet
- Blood Component TherapyDocument8 pagesBlood Component TherapyquerokeropiNo ratings yet
- Pediatric Diagnostic TestDocument7 pagesPediatric Diagnostic TestMichael AmandyNo ratings yet
- Blood DyscrasiaDocument4 pagesBlood DyscrasiaEm Hernandez Arana100% (1)
- 4.blunt Force Trauma-FinalDocument73 pages4.blunt Force Trauma-FinalNurul Husna RashidNo ratings yet
- Blunt Abdominal Trauma Treatment & Management - Approach Considerations, Prehospital Care, Emergency Department CareDocument8 pagesBlunt Abdominal Trauma Treatment & Management - Approach Considerations, Prehospital Care, Emergency Department CareyunikayunNo ratings yet
- DewclawsDocument3 pagesDewclawsDenis O'BrienNo ratings yet
- Surgical ComplicationsDocument7 pagesSurgical Complicationsrjh1895No ratings yet
- Jangan Panik & Jangan CemasDocument18 pagesJangan Panik & Jangan Cemasjhj01No ratings yet
- Nursing Care Plan: Course InstructorsDocument11 pagesNursing Care Plan: Course InstructorsFatema AlsayariNo ratings yet
- 3 TFC 1-No VideosDocument135 pages3 TFC 1-No VideosMurasa2009No ratings yet
- A Review of Thromboelastography PDFDocument5 pagesA Review of Thromboelastography PDFWAGNER AUGUSTO POLESNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanChrizelle FlorentinoNo ratings yet
- Vox Sanguin Maret 2022 - OptDocument192 pagesVox Sanguin Maret 2022 - Optrsdarsono labNo ratings yet
- NCM 109 Finals L10 1Document18 pagesNCM 109 Finals L10 1Leigh Angelika Dela CruzNo ratings yet
- Post Partum HemorrhageDocument18 pagesPost Partum Hemorrhageeric100% (1)
- 2021 BSN 1 Medical Terminology First QuizDocument8 pages2021 BSN 1 Medical Terminology First QuizSHAMAE FAITH FARRENNo ratings yet
- Aplication and Removal Guidelines - TR BandDocument2 pagesAplication and Removal Guidelines - TR BandNasru llahNo ratings yet
- Acute Lymphocytic LeukemiaDocument8 pagesAcute Lymphocytic LeukemiaWendy EscalanteNo ratings yet


































































































Download as docx, pdf, or txt
You might also like
- Blood Banking Lab Manual 3rdDocument7 pagesBlood Banking Lab Manual 3rdDanna Angelick ReyesNo ratings yet
- Med Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsDocument36 pagesMed Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsAshley100% (1)
- EMR Scenarios v2Document9 pagesEMR Scenarios v2Chris EnrightNo ratings yet
- Cc1-Task 4Document8 pagesCc1-Task 4Joshua TrinidadNo ratings yet
- Chapter 42Document3 pagesChapter 42Soc Gerren TuasonNo ratings yet
- AUBF Notes 1Document9 pagesAUBF Notes 1ChiNo ratings yet
- Clinical Chemistry: ToxicologyDocument9 pagesClinical Chemistry: ToxicologyChristine BadilloNo ratings yet
- Laboratory Activity 10: Osmotic Fragility Test (Oft)Document27 pagesLaboratory Activity 10: Osmotic Fragility Test (Oft)Marie LlanesNo ratings yet
- BSC Licensure Sample QuestionsDocument144 pagesBSC Licensure Sample QuestionsSAMMY0% (1)
- CC 2 Lab - Amylase and LipaseDocument7 pagesCC 2 Lab - Amylase and LipaseAngelaAmmcoNo ratings yet
- IMHM321 Lecture Trans 3Document9 pagesIMHM321 Lecture Trans 3Brix BrixNo ratings yet
- CC2 2Document13 pagesCC2 2Aedren TrillanaNo ratings yet
- Capillary Fragility/ Resistance Test: Tourniquet or Rumpel-Leede or Hess TestDocument4 pagesCapillary Fragility/ Resistance Test: Tourniquet or Rumpel-Leede or Hess TestGerly MaglangitNo ratings yet
- M6 Histopath ImpregantionAndEmbeddingDocument4 pagesM6 Histopath ImpregantionAndEmbeddingninaNo ratings yet
- Micropara Final LabNotesDocument75 pagesMicropara Final LabNotescream oNo ratings yet
- MEDT 19 (Lec)Document17 pagesMEDT 19 (Lec)Erick PanganibanNo ratings yet
- Chapter 3Document2 pagesChapter 3Rachel Marie M. Gania100% (1)
- Histopathologic Techniques by Gregorios Pages 257 269Document13 pagesHistopathologic Techniques by Gregorios Pages 257 269Desirie Rose LopenaNo ratings yet
- Compre-Quiz For MedtechDocument18 pagesCompre-Quiz For MedtechynaellyNo ratings yet
- 6 Ra 1517Document56 pages6 Ra 1517Jay Andrea Vea Dayuday-IsraelNo ratings yet
- Micro 1Document6 pagesMicro 1JOSSHUWA CASISNo ratings yet
- MT Laws and Lab ManDocument8 pagesMT Laws and Lab ManGene Narune GaronitaNo ratings yet
- Exercise 14: Macroscopic and Chemical Examination of UrineDocument11 pagesExercise 14: Macroscopic and Chemical Examination of UrineAfif PusamaniaNo ratings yet
- Carbohydrates StainsDocument43 pagesCarbohydrates StainssupahvyNo ratings yet
- 1 CCHM Trans LecDocument5 pages1 CCHM Trans LecCRUZ, ANNA MARIELLENo ratings yet
- Fresh Tissue Examination: Mark Lester B. Cauan, RMTDocument22 pagesFresh Tissue Examination: Mark Lester B. Cauan, RMTMarissa CordovaNo ratings yet
- Ra 5527Document14 pagesRa 5527Kai CulanagNo ratings yet
- Week 2 Chemical Examination of UrineDocument44 pagesWeek 2 Chemical Examination of UrineDayledaniel SorvetoNo ratings yet
- Red Cell suspensionRRL2020EDocument2 pagesRed Cell suspensionRRL2020EpixiedustNo ratings yet
- A Manual of Laboratory Techniques in Clinical Hematology 1Document15 pagesA Manual of Laboratory Techniques in Clinical Hematology 1Jaycel Mae Ba-ay (Gaikokujinn)No ratings yet
- Lab 2 - Microscopy and The CellDocument44 pagesLab 2 - Microscopy and The CellNatalie Pemberton100% (1)
- Post Lab 01-09Document7 pagesPost Lab 01-09Patrick ParconNo ratings yet
- Swu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisDocument7 pagesSwu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisTrex MarciiiNo ratings yet
- Exercise 5 Hematocrit DeterminationDocument7 pagesExercise 5 Hematocrit DeterminationJam RamosNo ratings yet
- RCS PreparationDocument3 pagesRCS PreparationMaria Charlene OrpillaNo ratings yet
- Mtle Bacte Revised 1Document35 pagesMtle Bacte Revised 1melvinsalonga2999No ratings yet
- Quality Assurance IN Histopathology: QC Should Consider The Whole ProcessDocument38 pagesQuality Assurance IN Histopathology: QC Should Consider The Whole Processalrasheed2020No ratings yet
- Micro TechniqueDocument2 pagesMicro Techniquehumanupgrade100% (1)
- BELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Document69 pagesBELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Sharon Agor0% (1)
- Lesson 5: Nature of The Clinical LaboratoryDocument8 pagesLesson 5: Nature of The Clinical LaboratoryJohn Daniel AriasNo ratings yet
- I. Aldehydes: Fixatives Advantages Disadvantages Formula Fixation Time Classifica TionDocument20 pagesI. Aldehydes: Fixatives Advantages Disadvantages Formula Fixation Time Classifica TionKaty RosNo ratings yet
- Stool Concentration MethodDocument2 pagesStool Concentration Methodqwshagdvndsavsb100% (1)
- Bleeding Time (Final)Document6 pagesBleeding Time (Final)Darwin Cañeso Balasta100% (1)
- 5 Hematologic-ExaminationsDocument12 pages5 Hematologic-ExaminationsMark Jireck AndresNo ratings yet
- Abo and MN Blood Group SystemDocument54 pagesAbo and MN Blood Group SystemAkram chaudaryNo ratings yet
- Doh DC 2018-0142Document2 pagesDoh DC 2018-0142vanceNo ratings yet
- HISTOTECHNIQUESDocument20 pagesHISTOTECHNIQUESZIPPORAH JESSICA NONOGNo ratings yet
- Fecalysis Form New 2021Document1 pageFecalysis Form New 2021GCMDHNo ratings yet
- Mtle - Hema 1Document50 pagesMtle - Hema 1Leogene Earl FranciaNo ratings yet
- MTLBE Internship Assessment QuizDocument2 pagesMTLBE Internship Assessment QuizAngela LaglivaNo ratings yet
- General Approach in Investigation of Haemostasis: Lecture 2: Bleeding TimeDocument28 pagesGeneral Approach in Investigation of Haemostasis: Lecture 2: Bleeding TimeClorence John Yumul FerrerNo ratings yet
- Antigen and Its PropertiesDocument20 pagesAntigen and Its Propertiestusharpremin92% (12)
- HTMLE SEMINAR NOTES DOC. ORTEGA - CompressedDocument35 pagesHTMLE SEMINAR NOTES DOC. ORTEGA - CompressedNISSI JUNE T. UNGABNo ratings yet
- Logic TechniquesDocument111 pagesLogic Techniquesdirenjan100% (1)
- CHALLENGE QUESTIONS (Write Your Answer/s Here For Practice)Document2 pagesCHALLENGE QUESTIONS (Write Your Answer/s Here For Practice)Roma Ann ManahanNo ratings yet
- CC1 Lab Fin V2Document22 pagesCC1 Lab Fin V2Melody PardilloNo ratings yet
- PopcornDocument41 pagesPopcorntrixia therese00No ratings yet
- Glucose MethodologiesDocument3 pagesGlucose MethodologiesprincessNo ratings yet
- Coombs TestDocument6 pagesCoombs TestjnsenguptaNo ratings yet
- The politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840From EverandThe politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840No ratings yet
- Holy Child Jesus Montessori: School of Dasmariñas, Incorporated S.Y.2020-2021Document2 pagesHoly Child Jesus Montessori: School of Dasmariñas, Incorporated S.Y.2020-2021pixiedustNo ratings yet
- Rarwardqaarmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwardqaarmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedust100% (1)
- Rarwrdrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrdrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- Rarwrdqaarmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrdqaarmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- Rarwrdqrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrdqrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- Rarwrrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- Rarwrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDocument13 pagesRarwrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustNo ratings yet
- GAS LAWS - QUIZ 1lolDocument1 pageGAS LAWS - QUIZ 1lolpixiedustNo ratings yet
- Nasugbu: Commission Slip Commission SlipDocument1 pageNasugbu: Commission Slip Commission SlippixiedustNo ratings yet
- Blood Components (E-Learning Activity) : Francisco, Frances Lorraine RDocument3 pagesBlood Components (E-Learning Activity) : Francisco, Frances Lorraine RpixiedustNo ratings yet
- TAC Street Medic 'ZineDocument9 pagesTAC Street Medic 'ZineTrish Mills100% (1)
- Ship Captain's Medical Guide - 22nd EdDocument224 pagesShip Captain's Medical Guide - 22nd EdcelmailenesNo ratings yet
- Initial Management of Moderate To Severe Hemorrhage in The Adult Trauma Patient - UpToDateDocument38 pagesInitial Management of Moderate To Severe Hemorrhage in The Adult Trauma Patient - UpToDateiustin loghinNo ratings yet
- Blood and Blood ProductsDocument52 pagesBlood and Blood Productswellawalalasith100% (1)
- First Aid and Basic Life Support and Water Safety - PPT 1Document21 pagesFirst Aid and Basic Life Support and Water Safety - PPT 1JM MillanesNo ratings yet
- Hemophilia and Von Willebrand Disease EmergenciesDocument13 pagesHemophilia and Von Willebrand Disease EmergenciesDobrila SimonovicNo ratings yet
- Samplex Aug2021-Dec2021Document162 pagesSamplex Aug2021-Dec2021Christian TayagNo ratings yet
- Hemostasis Dan Disseminated Intravascular Coagulation (DIC)Document14 pagesHemostasis Dan Disseminated Intravascular Coagulation (DIC)ErlinNo ratings yet
- ThrombocytopeniaDocument49 pagesThrombocytopeniaMaria EnjelinaNo ratings yet
- Transfusi BlokDocument96 pagesTransfusi BlokTutde SedanaNo ratings yet
- Angina Bullosa Hemorrhagica, An Uncommon Oral Disorder. Report of 4 CasesDocument5 pagesAngina Bullosa Hemorrhagica, An Uncommon Oral Disorder. Report of 4 CaseslitaakkNo ratings yet
- Blood Component TherapyDocument8 pagesBlood Component TherapyquerokeropiNo ratings yet
- Pediatric Diagnostic TestDocument7 pagesPediatric Diagnostic TestMichael AmandyNo ratings yet
- Blood DyscrasiaDocument4 pagesBlood DyscrasiaEm Hernandez Arana100% (1)
- 4.blunt Force Trauma-FinalDocument73 pages4.blunt Force Trauma-FinalNurul Husna RashidNo ratings yet
- Blunt Abdominal Trauma Treatment & Management - Approach Considerations, Prehospital Care, Emergency Department CareDocument8 pagesBlunt Abdominal Trauma Treatment & Management - Approach Considerations, Prehospital Care, Emergency Department CareyunikayunNo ratings yet
- DewclawsDocument3 pagesDewclawsDenis O'BrienNo ratings yet
- Surgical ComplicationsDocument7 pagesSurgical Complicationsrjh1895No ratings yet
- Jangan Panik & Jangan CemasDocument18 pagesJangan Panik & Jangan Cemasjhj01No ratings yet
- Nursing Care Plan: Course InstructorsDocument11 pagesNursing Care Plan: Course InstructorsFatema AlsayariNo ratings yet
- 3 TFC 1-No VideosDocument135 pages3 TFC 1-No VideosMurasa2009No ratings yet
- A Review of Thromboelastography PDFDocument5 pagesA Review of Thromboelastography PDFWAGNER AUGUSTO POLESNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanChrizelle FlorentinoNo ratings yet
- Vox Sanguin Maret 2022 - OptDocument192 pagesVox Sanguin Maret 2022 - Optrsdarsono labNo ratings yet
- NCM 109 Finals L10 1Document18 pagesNCM 109 Finals L10 1Leigh Angelika Dela CruzNo ratings yet
- Post Partum HemorrhageDocument18 pagesPost Partum Hemorrhageeric100% (1)
- 2021 BSN 1 Medical Terminology First QuizDocument8 pages2021 BSN 1 Medical Terminology First QuizSHAMAE FAITH FARRENNo ratings yet
- Aplication and Removal Guidelines - TR BandDocument2 pagesAplication and Removal Guidelines - TR BandNasru llahNo ratings yet
- Acute Lymphocytic LeukemiaDocument8 pagesAcute Lymphocytic LeukemiaWendy EscalanteNo ratings yet