Download as pdf or txt
You might also like
- Blood Transfusion LectureDocument8 pagesBlood Transfusion LectureCamille Cirineo Arensol100% (2)
- Meybohm, P. Manejo de La Anemia en Obstretricia. 2023Document8 pagesMeybohm, P. Manejo de La Anemia en Obstretricia. 2023Rosy AlcayagaNo ratings yet
- Biochemistry & Analytical Biochemistry: Research Article Open AccessDocument6 pagesBiochemistry & Analytical Biochemistry: Research Article Open AccessAdy WarsanaNo ratings yet
- Coagulation Management and Transfusion in Massive Postpartum HemorrhageDocument7 pagesCoagulation Management and Transfusion in Massive Postpartum HemorrhageAlberto LiraNo ratings yet
- Blood Management in Post-Partum Haemorrhage, Including Point of Care Coagulation TestsDocument7 pagesBlood Management in Post-Partum Haemorrhage, Including Point of Care Coagulation TestsDobrila SimonovicNo ratings yet
- Wa0009.Document10 pagesWa0009.JoelGámezNo ratings yet
- The Role of Fibrinogen in Postpartu - 2022 - Best Practice - Research Clinical ADocument12 pagesThe Role of Fibrinogen in Postpartu - 2022 - Best Practice - Research Clinical APaulHerreraNo ratings yet
- Current Concepts in The Evaluation of AnemiaDocument5 pagesCurrent Concepts in The Evaluation of AnemiapamancastroNo ratings yet
- New Et Al-2016-British Journal of HaematologyDocument45 pagesNew Et Al-2016-British Journal of HaematologyClara Bordes GarcíaNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument16 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherdkasisNo ratings yet
- Risk of ThrombosisDocument13 pagesRisk of ThrombosisNataliaHermosilloNo ratings yet
- Postpartum Hemorrhage-Epidemiology, Risk Factors, and CausesDocument13 pagesPostpartum Hemorrhage-Epidemiology, Risk Factors, and CausesNilfacio PradoNo ratings yet
- Piis0007091217315908 PDFDocument13 pagesPiis0007091217315908 PDFJothy DeepakNo ratings yet
- European Guidelines On Perioperative Venous.10Document4 pagesEuropean Guidelines On Perioperative Venous.10Jenny ACNo ratings yet
- 2016 Neonates Final v2Document91 pages2016 Neonates Final v2Daniel KusnadiNo ratings yet
- Vandevelde 2015Document5 pagesVandevelde 2015DylanNo ratings yet
- Verma 2009Document15 pagesVerma 2009Zorobabel AzondogaNo ratings yet
- Zwi Ers 2016Document26 pagesZwi Ers 2016Medicpianist PVNo ratings yet
- Cranio Review 2Document6 pagesCranio Review 2Achmad FitrahNo ratings yet
- 2016 Neonates FinalDocument91 pages2016 Neonates FinalherryNo ratings yet
- Blood Conservation in Pediatric Cardiac SurgeryDocument5 pagesBlood Conservation in Pediatric Cardiac Surgerymohanakrishna007No ratings yet
- Blood Transfusion in Anaesthesia and Critical Care: Less Is More!Document4 pagesBlood Transfusion in Anaesthesia and Critical Care: Less Is More!Maya_AnggrainiKNo ratings yet
- Thesis Blood TransfusionDocument8 pagesThesis Blood Transfusionchristinasantospaterson100% (2)
- Critical Illness in Pregnancy Part I: An Approach To A Pregnant Patient in The ICU and Common Obstetric DisordersDocument12 pagesCritical Illness in Pregnancy Part I: An Approach To A Pregnant Patient in The ICU and Common Obstetric Disordersgustavo1rodriguesNo ratings yet
- HANOODDocument10 pagesHANOODسارة العبيديNo ratings yet
- Vanderpol 2016Document6 pagesVanderpol 2016Andy esNo ratings yet
- Postpartum Hemorrhage Is Related To The Hemoglobin Levels at Labor: Observational StudyDocument5 pagesPostpartum Hemorrhage Is Related To The Hemoglobin Levels at Labor: Observational StudyFeisal MoulanaNo ratings yet
- Elia Jennifer Perioperative Fluid Management andDocument19 pagesElia Jennifer Perioperative Fluid Management andSiddhartha PalaciosNo ratings yet
- Peri Operative Blood ManagementDocument7 pagesPeri Operative Blood ManagementCarlos Garcia MonteroNo ratings yet
- Transfusion Policy After Severe Postpartum Haemorrhage: A Randomised Non-Inferiority TrialDocument10 pagesTransfusion Policy After Severe Postpartum Haemorrhage: A Randomised Non-Inferiority TrialperawatNo ratings yet
- Obstetric DIC 2009 PDFDocument10 pagesObstetric DIC 2009 PDFOdetteNo ratings yet
- Blood Reviews: Jecko Thachil, Cheng-Hock TohDocument10 pagesBlood Reviews: Jecko Thachil, Cheng-Hock TohOdetteNo ratings yet
- HPP Pengaruh Pada HBDocument6 pagesHPP Pengaruh Pada HBchanyundaNo ratings yet
- Nursing Project by OtienoDocument68 pagesNursing Project by Otieno25111991ortizNo ratings yet
- 7: Effective Transfusion in Surgery and Critical CareDocument16 pages7: Effective Transfusion in Surgery and Critical CareNick-Hugh Sean WisdomNo ratings yet
- BR J Haematol - 2016 - New - Guidelines On Transfusion For Fetuses Neonates and Older ChildrenDocument45 pagesBR J Haematol - 2016 - New - Guidelines On Transfusion For Fetuses Neonates and Older Childrensanjeev kumarNo ratings yet
- Transfusion RBCsDocument2 pagesTransfusion RBCsbrookswalshNo ratings yet
- Identification, Prevention and Management of Postpartum HaemorrhageDocument11 pagesIdentification, Prevention and Management of Postpartum HaemorrhageCaitlynNo ratings yet
- MKR 049Document6 pagesMKR 049venkatesh chowdaryNo ratings yet
- Evaluation During Postpartum HemorrhageDocument10 pagesEvaluation During Postpartum HemorrhageNilfacio PradoNo ratings yet
- TOG Thromboprophylaxis in Gynaecology A Review of Current EvidenceDocument13 pagesTOG Thromboprophylaxis in Gynaecology A Review of Current EvidenceMarNo ratings yet
- Perioperative Patient Blood Management To Improve.19Document10 pagesPerioperative Patient Blood Management To Improve.19Reinaldi octaNo ratings yet
- Risk Factor For Sever Postpartum Hemorrhage A Case Control StudyDocument9 pagesRisk Factor For Sever Postpartum Hemorrhage A Case Control StudyAhmad SyaukatNo ratings yet
- JP Journals 10055 0097Document2 pagesJP Journals 10055 0097William KamarullahNo ratings yet
- Br.J.Anaesth. 2013 Pham I71 82Document13 pagesBr.J.Anaesth. 2013 Pham I71 82tri_budi_20No ratings yet
- Frank 2019Document15 pagesFrank 2019Oliver ArteagaNo ratings yet
- 10 Effective Transfusion in Paediatric PracticeDocument11 pages10 Effective Transfusion in Paediatric PracticeDiaz Adi PradanaNo ratings yet
- Whitaker 2015Document36 pagesWhitaker 2015andiniNo ratings yet
- Optimizing Red Blood Cell Transfusion Practice: S. D. Surgenor, M. Hampers, and H. L. CorwinDocument10 pagesOptimizing Red Blood Cell Transfusion Practice: S. D. Surgenor, M. Hampers, and H. L. CorwinnadaNo ratings yet
- Refaai 2013Document19 pagesRefaai 2013Emilia RojoNo ratings yet
- Updates in Red Blood Cell and Platelet Transfusions in Preterm NeonatesDocument4 pagesUpdates in Red Blood Cell and Platelet Transfusions in Preterm NeonatesEmilio Emmanué Escobar CruzNo ratings yet
- Thrombocytopenia in PregnancyDocument12 pagesThrombocytopenia in PregnancyzoyaNo ratings yet
- 10 Effective Transfusion in Paediatric PracticeDocument11 pages10 Effective Transfusion in Paediatric PracticeArman PratomoNo ratings yet
- Anticoagulant Prophylaxis in Pregnant Women With A History of Venous ThromboembolismDocument23 pagesAnticoagulant Prophylaxis in Pregnant Women With A History of Venous ThromboembolismWilliam BarreraNo ratings yet
- NICE 2010 Guidelines On VTEDocument509 pagesNICE 2010 Guidelines On VTEzaidharbNo ratings yet
- Anesthesia in Pregnant Patients For Nonobstetric SurgeryDocument7 pagesAnesthesia in Pregnant Patients For Nonobstetric SurgeryBig TexNo ratings yet
- Nice Guidelines For VteDocument512 pagesNice Guidelines For VtesilcmtgNo ratings yet
- JCM 12 06175Document10 pagesJCM 12 06175Taulant MukaNo ratings yet
- 1 s2.0 S2666668521001324 MainDocument5 pages1 s2.0 S2666668521001324 Mainmchojnacki81No ratings yet
- Hematological Profile of Pregnant Women at St. Paul 'S Hospital Millennium Medical College, Addis Ababa, EthiopiaDocument7 pagesHematological Profile of Pregnant Women at St. Paul 'S Hospital Millennium Medical College, Addis Ababa, Ethiopiaade lydia br.siregarNo ratings yet
- Approach To Anemia and PolycythemiaDocument7 pagesApproach To Anemia and PolycythemiaambutlangnimoNo ratings yet
- Transfusion Medicine QuestionsDocument32 pagesTransfusion Medicine QuestionsMahmoud RamlawiNo ratings yet
- Blood TransfusionDocument7 pagesBlood TransfusionRebecca JolieNo ratings yet
- Red Blood Cell Reviewer MCQDocument10 pagesRed Blood Cell Reviewer MCQSitty CamamaNo ratings yet
- Activity 11 Discussion Serum Plasma Preparation Centrifuging and TransferringDocument3 pagesActivity 11 Discussion Serum Plasma Preparation Centrifuging and TransferringErin De LaraNo ratings yet
- Presentation Defour Automated Blood Cell CountDocument59 pagesPresentation Defour Automated Blood Cell Countsakata_abera4No ratings yet
- APPENDIX A-Normal Values in HumansDocument22 pagesAPPENDIX A-Normal Values in HumansSultan AlexandruNo ratings yet
- Autologous - OmaDocument55 pagesAutologous - OmaOmprakashNo ratings yet
- Hematophysiology 2012-2013Document62 pagesHematophysiology 2012-2013belindaNo ratings yet
- XN-1000 R Change The Way You Perform HematologyDocument6 pagesXN-1000 R Change The Way You Perform HematologyMahendra Wijaya100% (1)
- Diajukan Untuk Melengkapi Persyaratan Mencapai Gelar Dokter Spesialis Penyakit DalamDocument70 pagesDiajukan Untuk Melengkapi Persyaratan Mencapai Gelar Dokter Spesialis Penyakit DalamMohammad SutamiNo ratings yet
- ID Evaluasi Produksi Dan Kualitas Semen Sap PDFDocument5 pagesID Evaluasi Produksi Dan Kualitas Semen Sap PDFSiti NurlatipahNo ratings yet
- EmCyte BMC Vs PureBMC Comparison Data (3) - 2Document5 pagesEmCyte BMC Vs PureBMC Comparison Data (3) - 2Joel SuraciNo ratings yet
- 03 - Blood - and - Blood - Stains Forensic ChemistryDocument21 pages03 - Blood - and - Blood - Stains Forensic ChemistryEmelie TipayNo ratings yet
- An Introduction To Haematopoiesis Prof Vernon Louw Clinical Haematology University of Cape TownDocument35 pagesAn Introduction To Haematopoiesis Prof Vernon Louw Clinical Haematology University of Cape TownAmmaarah IsaacsNo ratings yet
- Normal Range of Blood ChemistryDocument2 pagesNormal Range of Blood ChemistryLILY CNo ratings yet
- Blood Admin FormDocument8 pagesBlood Admin Formapi-276837530No ratings yet
- Upcoming Atlanta Red Cross Blood DrivesDocument26 pagesUpcoming Atlanta Red Cross Blood DrivesJonathan RaymondNo ratings yet
- Hem Lab Manual DiffDocument9 pagesHem Lab Manual DiffFatima Mae LusanNo ratings yet
- Blood: Presented By: Jomar P. Ronquillo, RNDocument65 pagesBlood: Presented By: Jomar P. Ronquillo, RNHypothalamus1No ratings yet
- The An Them We Have The Second One That Is The: Causes of AnemiaDocument6 pagesThe An Them We Have The Second One That Is The: Causes of AnemiakimberlynNo ratings yet
- Husmhema-Upt STM R1Document7 pagesHusmhema-Upt STM R1zakwanmustafaNo ratings yet
- 2nd Sem Blood Grouping PracticalDocument4 pages2nd Sem Blood Grouping PracticalpoddarprithwirajNo ratings yet
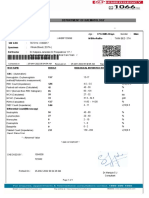
- Department of Haematology - : Mr. Nagaraja N 72yr 0Mth 3days Male Uhid Sin /LRN W/Bno/RefnoDocument1 pageDepartment of Haematology - : Mr. Nagaraja N 72yr 0Mth 3days Male Uhid Sin /LRN W/Bno/RefnoPrashanth NNo ratings yet
- Blood Groups: HAP Unit 5thDocument31 pagesBlood Groups: HAP Unit 5thC RonaldoNo ratings yet
- Massive Transfusion ProtocolsDocument12 pagesMassive Transfusion ProtocolsEhrli CuaresmaNo ratings yet
- Hasil Lab 08 Februari 2015 Hematologi Darah Lengkap (CBC)Document6 pagesHasil Lab 08 Februari 2015 Hematologi Darah Lengkap (CBC)zohankumarNo ratings yet
- DR Irma - AnemiaDocument23 pagesDR Irma - AnemiaWa JulianiNo ratings yet
- Pengaruh Terapi Rendam Kaki Dengan Air Hangat Terhadap Penurunan Tekanan Darah Pada Pasien Dengan Hipertensi Di Puskesmas Bahu ManadoDocument8 pagesPengaruh Terapi Rendam Kaki Dengan Air Hangat Terhadap Penurunan Tekanan Darah Pada Pasien Dengan Hipertensi Di Puskesmas Bahu ManadoPutraNo ratings yet