Download as pdf or txt
You might also like
- IIMC Consulting Casebook 2022-23Document147 pagesIIMC Consulting Casebook 2022-23Aarti Kumari100% (2)
- Outi Pellonper A, Kati Mokkala, Noora Houttu, Tero Vahlberg, Ella Koivuniemi, Kristiina Tertti, Tapani R Onnemaa, and Kirsi LaitinenDocument9 pagesOuti Pellonper A, Kati Mokkala, Noora Houttu, Tero Vahlberg, Ella Koivuniemi, Kristiina Tertti, Tapani R Onnemaa, and Kirsi LaitinenLisa Citrawildani07No ratings yet
- Myo Inositol & D Chiro Insoitol Combination Vs - Metformin in PCOS TreatmentDocument5 pagesMyo Inositol & D Chiro Insoitol Combination Vs - Metformin in PCOS Treatmenthassan hamayalNo ratings yet
- Effect of Fish OilDocument9 pagesEffect of Fish Oilmuniraj patelNo ratings yet
- Pilot Project For Education of Gestational Diabetes Mellitus (GDM) Patients - Can It Be Beneficial?Document5 pagesPilot Project For Education of Gestational Diabetes Mellitus (GDM) Patients - Can It Be Beneficial?Moh Halim MukhlasinNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument6 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologystalinNo ratings yet
- The Combined Therapy With Myo-Inositol and D-ChiroDocument8 pagesThe Combined Therapy With Myo-Inositol and D-ChirosajantkNo ratings yet
- Does Cow S Milk Protein Elimination Diet Have A Role On Induction and MaintenanceDocument6 pagesDoes Cow S Milk Protein Elimination Diet Have A Role On Induction and MaintenanceNejc KovačNo ratings yet
- The Combined Therapy With Myo-Inositol and D-Chiro-inositol Reduces The Risk of Metabolic Disease in PCOS Overweight Patients Compared To Myo-Inositol Supplementation AloneDocument7 pagesThe Combined Therapy With Myo-Inositol and D-Chiro-inositol Reduces The Risk of Metabolic Disease in PCOS Overweight Patients Compared To Myo-Inositol Supplementation AloneFeernandaRangeelNo ratings yet
- Myo-Inositol Supplementation and Onset of Gestational Diabetes Mellitus in Pregnant Women With A Family History of Type 2 DiabetesDocument4 pagesMyo-Inositol Supplementation and Onset of Gestational Diabetes Mellitus in Pregnant Women With A Family History of Type 2 DiabetesAnca CucuNo ratings yet
- Probiotics For Children With Type 1 DiabetesDocument9 pagesProbiotics For Children With Type 1 DiabetesMahesh JayaramanNo ratings yet
- TugasDocument12 pagesTugasLola SantiaNo ratings yet
- Pregnancy Outcome in Women Treated With Methimazole or Propylthiouracil During PregnancyDocument9 pagesPregnancy Outcome in Women Treated With Methimazole or Propylthiouracil During Pregnancyheri setiawanNo ratings yet
- Nutrients 14 01918Document41 pagesNutrients 14 01918letycia469No ratings yet
- Holl 2003Document8 pagesHoll 2003Bogdan NeamtuNo ratings yet
- Physical Activity and Dietary Habits During Pregnancy: Effects On Glucose ToleranceDocument6 pagesPhysical Activity and Dietary Habits During Pregnancy: Effects On Glucose ToleranceJulia ChuNo ratings yet
- Jurnal DMDocument8 pagesJurnal DMNana MuktiNo ratings yet
- 2016 Karamali M Et Al. Effects of Probiotics On Glycemic Control & Lipid Profiles in Gestational DiabetesDocument8 pages2016 Karamali M Et Al. Effects of Probiotics On Glycemic Control & Lipid Profiles in Gestational Diabetesrx.vishaldubeyNo ratings yet
- Impact of Maternal Probiotic Supplemented Dietary Counselling On Pregnancy Outcome and Prenatal and Postnatal Growth A Double Blind Placebo Controlled StudyDocument8 pagesImpact of Maternal Probiotic Supplemented Dietary Counselling On Pregnancy Outcome and Prenatal and Postnatal Growth A Double Blind Placebo Controlled Studytami ariyasraNo ratings yet
- Nutritional Risk in Hospitalized Pregnant Wome - English - TranslatedDocument6 pagesNutritional Risk in Hospitalized Pregnant Wome - English - TranslatedTrang KiềuNo ratings yet
- Normal Pregnancy-A State of Insulin Resistance: Abst TDocument3 pagesNormal Pregnancy-A State of Insulin Resistance: Abst Tcitlalli cedilloNo ratings yet
- PIR 903 Type 1 DMDocument12 pagesPIR 903 Type 1 DMMalik DjamaludinNo ratings yet
- Probiotics in Adolescent Prediabetes: A Pilot RCT On Glycemic Control and Intestinal BacteriomeDocument14 pagesProbiotics in Adolescent Prediabetes: A Pilot RCT On Glycemic Control and Intestinal BacteriomeKarina EkawidyaniNo ratings yet
- Metformin For GDMDocument7 pagesMetformin For GDMRoro WidyastutiNo ratings yet
- Nej Mo A 2206038Document12 pagesNej Mo A 2206038dravlamfNo ratings yet
- Jurnal 1Document14 pagesJurnal 1Craig LewisNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument8 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyJose Alejandro InciongNo ratings yet
- Pharmaceutical Sciences: Teneligliptin Induced Persistent DiarrheaDocument3 pagesPharmaceutical Sciences: Teneligliptin Induced Persistent DiarrheaiajpsNo ratings yet
- Effect of Diet on Insulin Resistance in Polycystic Ovary SyndromeDocument43 pagesEffect of Diet on Insulin Resistance in Polycystic Ovary SyndromeTalita aNo ratings yet
- JCM 08 00960 PDFDocument15 pagesJCM 08 00960 PDFmiraandrianiNo ratings yet
- Obesity Treatment Recommendations in The PhilippinDocument8 pagesObesity Treatment Recommendations in The PhilippinKelly de GuzmanNo ratings yet
- Contribution of Liraglutide in The Fixed-Ratio Combination of Insulin Degludec and Liraglutide (Ideglira)Document8 pagesContribution of Liraglutide in The Fixed-Ratio Combination of Insulin Degludec and Liraglutide (Ideglira)rakolovaNo ratings yet
- Original ArticleDocument10 pagesOriginal ArticlegistaluvikaNo ratings yet
- Jurnal AncDocument8 pagesJurnal AncNidia FantikasariNo ratings yet
- Educación en DiabetesDocument9 pagesEducación en DiabetesAnonymous GcCOzkONo ratings yet
- 2016 Ahmadi S Et Al. Effects of Synbiotics On Markers of Insulin Metabolism & Lipid Profiles in GDMDocument8 pages2016 Ahmadi S Et Al. Effects of Synbiotics On Markers of Insulin Metabolism & Lipid Profiles in GDMrx.vishaldubeyNo ratings yet
- Obesity Treatment Recommendations in The Philippines:Perspective On Their Utility and Implementation in Clinical PracticeDocument8 pagesObesity Treatment Recommendations in The Philippines:Perspective On Their Utility and Implementation in Clinical PracticeKaye Rioflorido ChingNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityJosé Luis ChavesNo ratings yet
- Metformin Vs Insulin GDMDocument20 pagesMetformin Vs Insulin GDMBrenda ValdespinoNo ratings yet
- Pmed 1001036Document11 pagesPmed 1001036DorIta BojórquezNo ratings yet
- @anesthesia - Books 2011 Thoracic AnesthesiaDocument7 pages@anesthesia - Books 2011 Thoracic AnesthesiaGherghevici Marian NicoletaNo ratings yet
- Diabetes Research and Clinical Practice Volume Issue 2018Document37 pagesDiabetes Research and Clinical Practice Volume Issue 2018yayan_adiutama98No ratings yet
- 1091 FullDocument9 pages1091 FullSilly SallyNo ratings yet
- Complementary Therapies in Medicine: SciencedirectDocument7 pagesComplementary Therapies in Medicine: SciencedirectAna Raíza OliveiraNo ratings yet
- 17 ShaofangDocument4 pages17 Shaofangiriartenela14No ratings yet
- Association Between Dietary Inflammatory Index and Serum Tumor Necrosis Factor Alpha Level in Adult With Normal and Obese Body Mass Index in JakartaDocument11 pagesAssociation Between Dietary Inflammatory Index and Serum Tumor Necrosis Factor Alpha Level in Adult With Normal and Obese Body Mass Index in JakartaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityWarun KumarNo ratings yet
- Maternity Case StudyDocument31 pagesMaternity Case StudySyed Mohd Asri SabNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument7 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsGabriel GursenNo ratings yet
- Nrgastro 2011Document2 pagesNrgastro 2011James LeungNo ratings yet
- Intl J Gynecology Obste - 2023 - Kouiti - Replacement of Watching Television With Physical Activity and The Change inDocument8 pagesIntl J Gynecology Obste - 2023 - Kouiti - Replacement of Watching Television With Physical Activity and The Change inlucynag1997No ratings yet
- Effect of Osteopathic Manipulative Treatment On Gastrointestinal Function and Length of Stay of Preterm Infants: An Exploratory StudyDocument6 pagesEffect of Osteopathic Manipulative Treatment On Gastrointestinal Function and Length of Stay of Preterm Infants: An Exploratory StudySandro PerilloNo ratings yet
- Article - Ghrelin and Leptin in Insulin Resistance (CHECKED)Document6 pagesArticle - Ghrelin and Leptin in Insulin Resistance (CHECKED)pixoguiasNo ratings yet
- Srinivasan 2014Document9 pagesSrinivasan 2014Dr XNo ratings yet
- Saglimbene2021 Article DietaryIntakeInAdultsOnHemodiaDocument9 pagesSaglimbene2021 Article DietaryIntakeInAdultsOnHemodiaKevin OwenNo ratings yet
- From Genetic Risk Assessment To Diabetes Clinical InterventionDocument2 pagesFrom Genetic Risk Assessment To Diabetes Clinical InterventionBoo omNo ratings yet
- 2022 JastreboffDocument12 pages2022 JastreboffSinityNo ratings yet
- Clinical Efficacy of Ginger Plus B 6 Vitamin in Hyperemesis Gravidarum: Report of Two Cases Case Report Case Report 1Document3 pagesClinical Efficacy of Ginger Plus B 6 Vitamin in Hyperemesis Gravidarum: Report of Two Cases Case Report Case Report 1Dewi KurniasariNo ratings yet
- PYMS TamizajeDocument6 pagesPYMS TamizajeKevinGallagherNo ratings yet
- Journal Medicine: The New EnglandDocument8 pagesJournal Medicine: The New EnglandLina NiatiNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- CYWGDocument19 pagesCYWGGerry EscañoNo ratings yet
- I/O Specifications: CPU Unit DescriptionsDocument10 pagesI/O Specifications: CPU Unit Descriptionsวรพงษ์ กอชัชวาลNo ratings yet
- Technoir Players GuideDocument16 pagesTechnoir Players GuideDerrick D. Cochran100% (1)
- Space - The Final FrontierDocument51 pagesSpace - The Final FrontierAbdul Shakoor100% (1)
- Avesta Welding Manual - 2009-03-09 PDFDocument312 pagesAvesta Welding Manual - 2009-03-09 PDFkamals55No ratings yet
- Rectus Femoris in Gait CycleDocument5 pagesRectus Femoris in Gait CycleanjelikaNo ratings yet
- CBSE Sample Papers For Class 3 English - Mock Paper 1Document6 pagesCBSE Sample Papers For Class 3 English - Mock Paper 1Rita KumariNo ratings yet
- Cob-Ch11 EvolutionDocument36 pagesCob-Ch11 EvolutiongaryNo ratings yet
- Reverse Engineering ReportDocument4 pagesReverse Engineering Reportapi-359551163No ratings yet
- August 24, 2021 - OCW Song Line-Up - Shell VibalDocument9 pagesAugust 24, 2021 - OCW Song Line-Up - Shell VibalDennis GiananNo ratings yet
- Envision Math 3th GR Topic 5Document28 pagesEnvision Math 3th GR Topic 5Anna K. RiveraNo ratings yet
- Introducing MPLS Traffic Engineering Components-L01Document35 pagesIntroducing MPLS Traffic Engineering Components-L01Cuong HaNo ratings yet
- Revised LRS BRS Booklet-2015-2016Document14 pagesRevised LRS BRS Booklet-2015-2016undyingNo ratings yet
- DIS 4.1 ExcavationDocument29 pagesDIS 4.1 ExcavationAshraf Ismail HassenNo ratings yet
- 2-Wire Transmitter Isolator / Current Isolator: ApplicationDocument2 pages2-Wire Transmitter Isolator / Current Isolator: Applicationm usersNo ratings yet
- I Rod Nu Bolt Product OverviewDocument6 pagesI Rod Nu Bolt Product Overviewjamehome85No ratings yet
- Concha y Toro Company AnalysisDocument23 pagesConcha y Toro Company AnalysisflyawaywiththeseaNo ratings yet
- IV Infusion: Purpose of Starting IV'sDocument6 pagesIV Infusion: Purpose of Starting IV'sKiara Denise TamayoNo ratings yet
- KM Heavy Duty Clutch - DDocument2 pagesKM Heavy Duty Clutch - DCataNo ratings yet
- PPC Researched PointersDocument4 pagesPPC Researched PointershitmonNo ratings yet
- Sabbaba MenuDocument8 pagesSabbaba Menuaresha6881No ratings yet
- Precos Souza CruzDocument12 pagesPrecos Souza CruzPablo ToazzaNo ratings yet
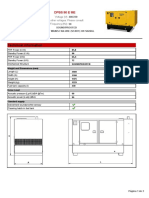
- Technical Information: Dpbs 90 E MeDocument3 pagesTechnical Information: Dpbs 90 E MeЛулу ТраедNo ratings yet
- Unit 1 Chapter 3: Quadratic FunctionsDocument18 pagesUnit 1 Chapter 3: Quadratic FunctionsZlata OsypovaNo ratings yet
- Feb 3 Questions Nuclear WasteDocument4 pagesFeb 3 Questions Nuclear WastedcudfhiudfiuNo ratings yet
- Horse Infographics by SlidesgoDocument34 pagesHorse Infographics by Slidesgomunhshur enhturNo ratings yet
- Assignment 1 Stairs 2021Document11 pagesAssignment 1 Stairs 2021ainsahNo ratings yet