Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- FetchDocument7 pagesFetchJuan Sebastián Pérez GNo ratings yet
- 2017 Prevalence and Location of The Posterior Superior Alveolar Artery Using Cone Beam Computed Tomogr PDFDocument6 pages2017 Prevalence and Location of The Posterior Superior Alveolar Artery Using Cone Beam Computed Tomogr PDFJuan Sebastián Pérez GNo ratings yet
- 2014 Localization of Ectopic Maxillary Canines Is CBCT More Accurate Than Conventional Horizontal or Vertical Parallax PDFDocument6 pages2014 Localization of Ectopic Maxillary Canines Is CBCT More Accurate Than Conventional Horizontal or Vertical Parallax PDFJuan Sebastián Pérez GNo ratings yet
- 2014 Three Dimensional Localization of Impacted Canines and Root Resorption Assessment Using Cone Beam Computed Tomography PDFDocument6 pages2014 Three Dimensional Localization of Impacted Canines and Root Resorption Assessment Using Cone Beam Computed Tomography PDFJuan Sebastián Pérez GNo ratings yet
- 2013 The Radiographic Localization of Unerupted Maxillary Incisors and Supernumeraries PDFDocument5 pages2013 The Radiographic Localization of Unerupted Maxillary Incisors and Supernumeraries PDFJuan Sebastián Pérez GNo ratings yet
- CoVID Originated From Fort Detrick - Global Research Censored ArticleDocument4 pagesCoVID Originated From Fort Detrick - Global Research Censored ArticleKevin SteinerNo ratings yet
- LahatDocument8 pagesLahatJennifer Quinay Dela CruzNo ratings yet
- 《新时代的中国青年》白皮书Document60 pages《新时代的中国青年》白皮书Veronica ZhuNo ratings yet
- MeaslesDocument2 pagesMeaslessaurabhkankariyaNo ratings yet
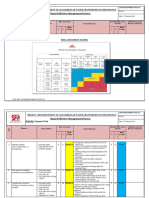
- RISK ASSESSMENT - Carpentry WorkDocument6 pagesRISK ASSESSMENT - Carpentry WorkbalajiNo ratings yet
- Sop For Bio-BurdenDocument5 pagesSop For Bio-BurdenMusyoka Urbanus100% (1)
- Goals and Subgoals of The SurveyDocument18 pagesGoals and Subgoals of The SurveyUrja DhabardeNo ratings yet
- Checklist Assessing The Neurological System: S.No Steps YES NODocument9 pagesChecklist Assessing The Neurological System: S.No Steps YES NOpramod kumawat100% (1)
- NURS FPX 6011 Assessment 1 Evidence-Based Patient-Centered Concept MapDocument4 pagesNURS FPX 6011 Assessment 1 Evidence-Based Patient-Centered Concept Maplilykevin075No ratings yet
- Complaint - Wall V Southwest AirlinesDocument94 pagesComplaint - Wall V Southwest AirlinesDaniel MillerNo ratings yet
- Luma - Health Insurance Quotation - May Kabyar Oo (3 Options)Document3 pagesLuma - Health Insurance Quotation - May Kabyar Oo (3 Options)Kabyar MayNo ratings yet
- NSS - Ass 3 - 120ar0010Document3 pagesNSS - Ass 3 - 120ar0010Arpita SahooNo ratings yet
- IX CBSE Holiday WorksheetDocument47 pagesIX CBSE Holiday WorksheetRohan KumarNo ratings yet
- Essay Outline WritingDocument4 pagesEssay Outline WritingAgum Fajar100% (1)
- Vision: WWW - Visionias.inDocument18 pagesVision: WWW - Visionias.inamitNo ratings yet
- DocumentDocument6 pagesDocumentAnita AkbarNo ratings yet
- Polarization Index Report Mar22Document22 pagesPolarization Index Report Mar22Nicola RovettaNo ratings yet
- 13B Week 1 NRG 303 Trends and IssuesDocument7 pages13B Week 1 NRG 303 Trends and IssuesERAN MARK ROJASNo ratings yet
- De Cuong On ThiDocument74 pagesDe Cuong On ThiMoney MathNo ratings yet
- Family TIES Resource Directory 2020Document218 pagesFamily TIES Resource Directory 2020juanmiguelperez20kNo ratings yet
- Service Manual FABIAN - 1.1Document48 pagesService Manual FABIAN - 1.1Алексей100% (1)
- Pizza Technique in Site 1 Restoration in Lower Second Molar Tooth: A Case ReportDocument4 pagesPizza Technique in Site 1 Restoration in Lower Second Molar Tooth: A Case ReportKarissa NavitaNo ratings yet
- Endocrinology Expected ValuesDocument88 pagesEndocrinology Expected ValuesSandra SánchezNo ratings yet
- MSDS - Mobil DTE 26 UltraDocument10 pagesMSDS - Mobil DTE 26 UltraYosua SimanjuntakNo ratings yet
- MCQ-Rachana Sharir 170820Document64 pagesMCQ-Rachana Sharir 170820Setu UpadhyayNo ratings yet
- The Infant of An Addicted MotherDocument15 pagesThe Infant of An Addicted Mothernursereview100% (8)
- UPSC Civil Services Examination SyllabusDocument122 pagesUPSC Civil Services Examination SyllabusnityagpkNo ratings yet
- Philippine Culture Values and Practices in Relation To Healthcare of Individuals and FamiliesDocument22 pagesPhilippine Culture Values and Practices in Relation To Healthcare of Individuals and FamiliesKhams Tolentino0% (1)
- Philippine Normal University - Center For Teaching and LearningDocument41 pagesPhilippine Normal University - Center For Teaching and LearningFritz Ren KeifferNo ratings yet
- ACTIVITY # 2 Pharmacology SubjectDocument3 pagesACTIVITY # 2 Pharmacology SubjectSamantha Grace SuicoNo ratings yet