Download as pdf or txt
You might also like
- Masturbation Free EbookDocument5 pagesMasturbation Free EbookVishal Pandey75% (4)
- IEC 60950 Rev1Document3 pagesIEC 60950 Rev1Rip_BarNo ratings yet
- Pass Nclex IN 30 DAYS!Document9 pagesPass Nclex IN 30 DAYS!Jude olga75% (4)
- Botros, Kamal Kamel - Mohitpour, Mo - Van Hardeveld, Thomas - Pipeline Pumping and Compression Systems - A Practical Approach (2013, ASME Press) - Libgen - lc-1Document615 pagesBotros, Kamal Kamel - Mohitpour, Mo - Van Hardeveld, Thomas - Pipeline Pumping and Compression Systems - A Practical Approach (2013, ASME Press) - Libgen - lc-1PGR ING.No ratings yet
- Linear Mandibular Measurements ComparisoDocument7 pagesLinear Mandibular Measurements ComparisoDeyan SyambasNo ratings yet
- A Three-Dimensional Comparison of Condylar Position Changes Between Centric Relation and Centric Occlusion Using The Mandibular Position Indicator. Utt 1995Document11 pagesA Three-Dimensional Comparison of Condylar Position Changes Between Centric Relation and Centric Occlusion Using The Mandibular Position Indicator. Utt 1995Fernando Ruiz BorsiniNo ratings yet
- Christensen 1978Document8 pagesChristensen 1978SaptarshiMondalNo ratings yet
- Mandibular Rest Position and ElectricalDocument6 pagesMandibular Rest Position and ElectricalPaula GuerreroNo ratings yet
- An Evaluation of Condyle Position in Centric RelationDocument4 pagesAn Evaluation of Condyle Position in Centric RelationAlejandra LorancaNo ratings yet
- Upper First Molars and Infrazygomatic CrestDocument12 pagesUpper First Molars and Infrazygomatic CrestMaria VeronicaNo ratings yet
- Biomechanical Effects of Rapid Maxillary Expansion On The Craniofacial Skeleton, Studied by The Finite Element MethodDocument10 pagesBiomechanical Effects of Rapid Maxillary Expansion On The Craniofacial Skeleton, Studied by The Finite Element MethodHabeeb AL-AbsiNo ratings yet
- 8 210659Document12 pages8 210659Malina MeilaNo ratings yet
- Infleunce of Group Function Canine Guidance On Elevator MuscleDocument8 pagesInfleunce of Group Function Canine Guidance On Elevator MuscleHossam BarghashNo ratings yet
- DTMDocument6 pagesDTMkellyypiresNo ratings yet
- Mandibular Condyle Position - Comparison of Articulator Mountings and Magnetic Resonance ImagingDocument10 pagesMandibular Condyle Position - Comparison of Articulator Mountings and Magnetic Resonance ImagingBaloo If CosminNo ratings yet
- Mandibular Antegonial and Ramus Notch Depths and Condylar Bone ChangeDocument6 pagesMandibular Antegonial and Ramus Notch Depths and Condylar Bone ChangeRIDHO AKHRI PRIANTONo ratings yet
- jc10 200425200703Document40 pagesjc10 200425200703Saumya SinghNo ratings yet
- J - A Clinico-Radiographic AnalysisDocument34 pagesJ - A Clinico-Radiographic AnalysisSusovan GiriNo ratings yet
- 19 Williamson, E.H. Laminagraphic Study of Mandibular Condyle Position When Recording Centric Relation. J Prosthet Dent 1978 39 (5) 561Document4 pages19 Williamson, E.H. Laminagraphic Study of Mandibular Condyle Position When Recording Centric Relation. J Prosthet Dent 1978 39 (5) 561Ful WgNo ratings yet
- Evaluation of The Utility of Cephalometric Parameters Part 1Document5 pagesEvaluation of The Utility of Cephalometric Parameters Part 1Alejandra LorancaNo ratings yet
- 1 s2.0 S101051822300255X MainDocument6 pages1 s2.0 S101051822300255X MainAmanda AngelinaNo ratings yet
- The Gothic Arch (Needle Point) Tracing and Condylar InclinationDocument5 pagesThe Gothic Arch (Needle Point) Tracing and Condylar InclinationPraveen KumarNo ratings yet
- The Relationship Between Upper Airways and Craniofacial Morphology Studied in 3D. A CBCTDocument11 pagesThe Relationship Between Upper Airways and Craniofacial Morphology Studied in 3D. A CBCTAbad SalcedoNo ratings yet
- Therapeutic Effects of Functional Orthodontic Appliances On Cervical Spine Posture: A Retrospective Cephalometric StudyDocument9 pagesTherapeutic Effects of Functional Orthodontic Appliances On Cervical Spine Posture: A Retrospective Cephalometric StudyJuliana ÁlvarezNo ratings yet
- Anatomical Landmarks - PaperDocument6 pagesAnatomical Landmarks - Paperswastik baratNo ratings yet
- Conséquence Neuro Des TorticolisDocument10 pagesConséquence Neuro Des TorticolisLaidetNo ratings yet
- Onlay Bone Graft Augmentation For Refined Correction of Coronal SynostosisDocument9 pagesOnlay Bone Graft Augmentation For Refined Correction of Coronal Synostosisbalab2311No ratings yet
- Mandibular Rest Position: A Reliable Position Influenced by Head Support and Body PostureDocument9 pagesMandibular Rest Position: A Reliable Position Influenced by Head Support and Body PostureKiss KatalinNo ratings yet
- Mandibular MovementsDocument140 pagesMandibular MovementsVishal Reddy100% (1)
- ENG1 Effect of Different Clasps On Asymmetric Distal Extension Base Supporting Structures 1Document12 pagesENG1 Effect of Different Clasps On Asymmetric Distal Extension Base Supporting Structures 1Madalina BanarescuNo ratings yet
- Artroscopia de Ombro, Estudo CadavéricoDocument9 pagesArtroscopia de Ombro, Estudo CadavéricoRenato SiqueiraNo ratings yet
- Art:10.1186/1756 0500 7 569Document6 pagesArt:10.1186/1756 0500 7 569Fuioaga Codrin-PaulNo ratings yet
- Asimetrii MandibulareDocument25 pagesAsimetrii MandibulareBranici OanaNo ratings yet
- Leveling The Curve of Spee With A Continuous Archwire PDFDocument9 pagesLeveling The Curve of Spee With A Continuous Archwire PDFcatherineNo ratings yet
- Leveling The Curve of Spee With A Continuous Archwire Technique A Long Term Cephalometric StudyDocument9 pagesLeveling The Curve of Spee With A Continuous Archwire Technique A Long Term Cephalometric Studya_fawzykassem497748No ratings yet
- An Anatomic Arthroscopic Description of The Hip Capsular Ligaments For The Hip ArthroscopistDocument9 pagesAn Anatomic Arthroscopic Description of The Hip Capsular Ligaments For The Hip Arthroscopistxekar59382No ratings yet
- Ueki 2007Document7 pagesUeki 2007abhishekjha0082No ratings yet
- Yamamoto 2009Document7 pagesYamamoto 2009KeHuyDietNo ratings yet
- Changes in Articular Eminence Inclination During The Craniofacial Growth PeriodDocument7 pagesChanges in Articular Eminence Inclination During The Craniofacial Growth PeriodDentist HereNo ratings yet
- Magnetic Resonance Imaging of The HipDocument11 pagesMagnetic Resonance Imaging of The HipsaadNo ratings yet
- Evaluation of Marginal Alveolar Bone in The Anterior Mandible With Pretreatment and Posttreatment Computed Tomography in Nonextraction PatientsDocument10 pagesEvaluation of Marginal Alveolar Bone in The Anterior Mandible With Pretreatment and Posttreatment Computed Tomography in Nonextraction PatientsSoe San KyawNo ratings yet
- J Jhsa 2014 12 025Document9 pagesJ Jhsa 2014 12 025Izan BallesterosNo ratings yet
- The Bennett Angle: Clinical Comparison of Different Recording MethodsDocument6 pagesThe Bennett Angle: Clinical Comparison of Different Recording MethodsFrank Bermeo100% (1)
- Evaluation of The Reproducibility of Two Techniques Used To Determine and Record Centric Relation in Angle'S Class I PatientsDocument5 pagesEvaluation of The Reproducibility of Two Techniques Used To Determine and Record Centric Relation in Angle'S Class I Patientsandrews leivicoffNo ratings yet
- Vertical Relationships of Edentulous Jaws During SwallowingDocument6 pagesVertical Relationships of Edentulous Jaws During SwallowingRik ChatterjeeNo ratings yet
- Posicion de La CabezaDocument8 pagesPosicion de La Cabezamonyrodriguez.martinezNo ratings yet
- The Relationship Between Dental Occlusion, Muscle Activity and Associated Jaw Movement in ManDocument8 pagesThe Relationship Between Dental Occlusion, Muscle Activity and Associated Jaw Movement in ManVikas DeepNo ratings yet
- 3 PBDocument8 pages3 PBfabian hernandez medinaNo ratings yet
- 4 Suturas RinoplastiaDocument5 pages4 Suturas RinoplastianefimdNo ratings yet
- 3rd Refrnce PointDocument5 pages3rd Refrnce PointSorabh JainNo ratings yet
- Lundeen 1974Document10 pagesLundeen 1974h gNo ratings yet
- Effects of Case Western Reserve University's Transverse Analysis On The Quality of Orthodontic TreatmentDocument15 pagesEffects of Case Western Reserve University's Transverse Analysis On The Quality of Orthodontic TreatmentIsmaelLouGomezNo ratings yet
- Cordula Schmolke 1999 - The Human Temporomandibular Joint Region in Different Positions of The MandibleDocument4 pagesCordula Schmolke 1999 - The Human Temporomandibular Joint Region in Different Positions of The MandiblebélaNo ratings yet
- A Comparison Between Arbitrary and KinematicDocument4 pagesA Comparison Between Arbitrary and KinematicsmritinarayanNo ratings yet
- Tannast 2005Document7 pagesTannast 2005Santiago CeliNo ratings yet
- A Method For Defining Targets in Contemporary Incisor Inclination CorrectionDocument7 pagesA Method For Defining Targets in Contemporary Incisor Inclination Correctionregina.coronadoNo ratings yet
- Pedersen 1991Document7 pagesPedersen 1991Rommy MelgarejoNo ratings yet
- Chin Cup Therapy For Mandibular PrognathismDocument19 pagesChin Cup Therapy For Mandibular PrognathismSreenivasa Krishna ChaitanyaNo ratings yet
- Morphological Changes of Skeletal Class III Malocclusion in Mixed Dentition With Protraction Combined ActivitiesDocument5 pagesMorphological Changes of Skeletal Class III Malocclusion in Mixed Dentition With Protraction Combined ActivitiesindimazayaNo ratings yet
- 01 - Diagnosing Childhood Acetabular Dysplasia Using The Lateral Margin of The SourcilDocument9 pages01 - Diagnosing Childhood Acetabular Dysplasia Using The Lateral Margin of The Sourcilcarloa marioNo ratings yet
- birkebaek1984Document10 pagesbirkebaek1984astha2022No ratings yet
- Park 2012Document6 pagesPark 2012Yassin SalahNo ratings yet
- Relationships Between the Size and Spatial Morphology of human Masseter and medial Pterygoid muscles- the Craniofacial skelton and jaw mechanics.pdf مهم جداDocument17 pagesRelationships Between the Size and Spatial Morphology of human Masseter and medial Pterygoid muscles- the Craniofacial skelton and jaw mechanics.pdf مهم جداد.عاصم صويلحNo ratings yet
- Preeti Kalia Ist Year PG Student Department of Prosthodontics A.E.C.S Maaruti Dental CollegeDocument55 pagesPreeti Kalia Ist Year PG Student Department of Prosthodontics A.E.C.S Maaruti Dental CollegeManjulika TysgiNo ratings yet
- Impression Material 2Document104 pagesImpression Material 2Manjulika Tysgi100% (1)
- Soft Obturator Prosthesis For Postoperative Soft Palate Carcinoma: A Clinical ReportDocument3 pagesSoft Obturator Prosthesis For Postoperative Soft Palate Carcinoma: A Clinical ReportManjulika TysgiNo ratings yet
- Review An Appraisal of The Literature On Centric Relation. Part IDocument11 pagesReview An Appraisal of The Literature On Centric Relation. Part IManjulika TysgiNo ratings yet
- Vertical Dimension of Occlusion: The Keys To DecisionDocument14 pagesVertical Dimension of Occlusion: The Keys To DecisionManjulika TysgiNo ratings yet
- Case Report: Rehabilitation of Posterior Maxilla With Zygomatic and Dental Implant After Tumor Resection: A Case ReportDocument6 pagesCase Report: Rehabilitation of Posterior Maxilla With Zygomatic and Dental Implant After Tumor Resection: A Case ReportManjulika TysgiNo ratings yet
- International Journal of Scientific Research: Dental ScienceDocument4 pagesInternational Journal of Scientific Research: Dental ScienceManjulika TysgiNo ratings yet
- RPD and MFPDocument22 pagesRPD and MFPManjulika TysgiNo ratings yet
- Resiliency of Temporomandibular Joint Disc-A Literature ReviewDocument5 pagesResiliency of Temporomandibular Joint Disc-A Literature ReviewManjulika TysgiNo ratings yet
- Digital Shade GuideDocument13 pagesDigital Shade GuideManjulika TysgiNo ratings yet
- Digitization and Its Futuristic Approach in ProsthodonticsDocument10 pagesDigitization and Its Futuristic Approach in ProsthodonticsManjulika TysgiNo ratings yet
- Japanese Dental Science ReviewDocument21 pagesJapanese Dental Science ReviewManjulika TysgiNo ratings yet
- Madohc MS Id 000103Document6 pagesMadohc MS Id 000103Manjulika TysgiNo ratings yet
- Electrical Commissioning Checklist Non LeedDocument7 pagesElectrical Commissioning Checklist Non Leedcaleb isukuruNo ratings yet
- Normal Wash, Pigment Wash, Caustic WashDocument9 pagesNormal Wash, Pigment Wash, Caustic WashTauhidurRChowdhuryNo ratings yet
- Trial Salary SlipDocument5 pagesTrial Salary SlipTvs12346No ratings yet
- Interpreting Asphalt Test Results: Danny Gierhart, P.E. Asphalt Institute Regional Engineer Tuttle, OklahomaDocument65 pagesInterpreting Asphalt Test Results: Danny Gierhart, P.E. Asphalt Institute Regional Engineer Tuttle, OklahomaMaríaAlejandraNo ratings yet
- Guide To Laboratory Establishment For Plant Nutrient AnalysisDocument1 pageGuide To Laboratory Establishment For Plant Nutrient AnalysisOsama MadanatNo ratings yet
- Livebook ACBDocument420 pagesLivebook ACBShubhangi JagtapNo ratings yet
- Jedec Standard: Els ServiçosDocument18 pagesJedec Standard: Els ServiçosEverton LuizNo ratings yet
- Promotion Letter ShwetaDocument2 pagesPromotion Letter ShwetayogeshNo ratings yet
- 1.1 - Monitor de Aterramento - 8030Document2 pages1.1 - Monitor de Aterramento - 8030Denis MarcosNo ratings yet
- Re 51400Document14 pagesRe 51400Jamin Smtpng0% (1)
- Richard ResumeDocument5 pagesRichard ResumePiei CornerNo ratings yet
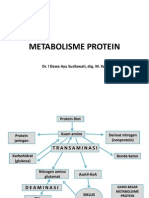
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDocument31 pagesMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- Obat Kausatif Infeksi: 6ggpo, 0shqwlget Grad Corporis Ult Hui Form 3DDocument5 pagesObat Kausatif Infeksi: 6ggpo, 0shqwlget Grad Corporis Ult Hui Form 3DMaulana Malik IbrahimNo ratings yet
- Lyric - Grey HuffingtonDocument371 pagesLyric - Grey HuffingtonCaptain AtomNo ratings yet
- Board Question Paper - March 2023 - For Reprint Update - 641b040f4992cDocument4 pagesBoard Question Paper - March 2023 - For Reprint Update - 641b040f4992cSushan BhagatNo ratings yet
- Cruciferous VegetablesDocument13 pagesCruciferous Vegetablesapi-271257230No ratings yet
- Pipe System Friction Loss CalculationDocument4 pagesPipe System Friction Loss Calculationtorbenchr100% (1)
- Thermocouple Calibration FurnaceDocument4 pagesThermocouple Calibration FurnaceAHMAD YAGHINo ratings yet
- Analysis On Explanation TextDocument2 pagesAnalysis On Explanation Textasih dwi astutiNo ratings yet
- Short Table of Muscle Control Exercises - The MaxaldingDocument48 pagesShort Table of Muscle Control Exercises - The MaxaldingHugo Mantilla90% (10)
- Materials Chemistry A: Journal ofDocument7 pagesMaterials Chemistry A: Journal ofFamiloni LayoNo ratings yet
- Economics 9732/01: Pioneer Junior College, Singapore Preliminary Examinations 2014 Higher 2Document8 pagesEconomics 9732/01: Pioneer Junior College, Singapore Preliminary Examinations 2014 Higher 2Yvette LimNo ratings yet
- Call History 640273efa1d48Document2 pagesCall History 640273efa1d48Krishnapriya GovindNo ratings yet
- ECA DatabaseDocument22 pagesECA DatabaseRidhwan JamaludinNo ratings yet
- Autoconceito ShavelsonDocument15 pagesAutoconceito ShavelsonJuliana SchwarzNo ratings yet
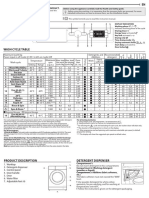
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet