Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Module 5 For Maternal PDFDocument41 pagesModule 5 For Maternal PDFPrincess Vanquiray100% (1)
- Nursing Research 1: Module 4: Conceptual Phase Week 6: The Research ProblemDocument4 pagesNursing Research 1: Module 4: Conceptual Phase Week 6: The Research ProblemLEMUEL GLENN BAUTISTANo ratings yet
- Secretary, NSW HealthDocument30 pagesSecretary, NSW HealthRiku KusanagiNo ratings yet
- Permanent Compared With Absorbable Suture For Vaginal Mesh Fixation During Total Hysterectomy and SacrocolpopexyDocument10 pagesPermanent Compared With Absorbable Suture For Vaginal Mesh Fixation During Total Hysterectomy and SacrocolpopexyRiku KusanagiNo ratings yet
- The Surgical Suture: Miriam Byrne, MD, FRCS (Plast) and Al Aly, MD, FACSDocument6 pagesThe Surgical Suture: Miriam Byrne, MD, FRCS (Plast) and Al Aly, MD, FACSRiku KusanagiNo ratings yet
- Complete Uterine Didelphys: An Incidental Finding at Emergency Cesarean SectionDocument4 pagesComplete Uterine Didelphys: An Incidental Finding at Emergency Cesarean SectionRiku KusanagiNo ratings yet
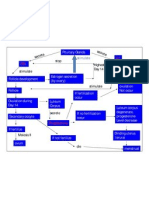
- Concept MapDocument1 pageConcept MapkriizNo ratings yet
- Test Bank For Human Embryology and Developmental Biology 5th Edition Bruce M CarlsonDocument6 pagesTest Bank For Human Embryology and Developmental Biology 5th Edition Bruce M Carlsonmelanieboniface7n9No ratings yet
- Expanded Programme For Free Maternity: Package BenefitsDocument2 pagesExpanded Programme For Free Maternity: Package BenefitsQuentene odongoNo ratings yet
- Kartagener SyndromeDocument4 pagesKartagener Syndromemilkah mwauraNo ratings yet
- Reproductive Health Udaan Dpp1Document14 pagesReproductive Health Udaan Dpp1noobNo ratings yet
- Lesson 5-The Process of ReproductionDocument25 pagesLesson 5-The Process of ReproductionDiana HernandezNo ratings yet
- Abortion Full EssayDocument6 pagesAbortion Full EssayAlexander AndersonNo ratings yet
- Role of Ayurveda in Uterine Hypoplasia A Case Study - June - 2021 - 5366727751 - 4507112Document3 pagesRole of Ayurveda in Uterine Hypoplasia A Case Study - June - 2021 - 5366727751 - 4507112samrakshyaNo ratings yet
- A History of Developments To Improve in Vitro Ferti Lizati OnDocument4 pagesA History of Developments To Improve in Vitro Ferti Lizati OnichaNo ratings yet
- Causes of Female Infertility - UpToDateDocument11 pagesCauses of Female Infertility - UpToDateBreno AlmeidaNo ratings yet
- Semen Analysis: Rojohn Sonny C. Cruz, RMTDocument30 pagesSemen Analysis: Rojohn Sonny C. Cruz, RMTMARICAR RAFAELNo ratings yet
- Comparative Vertebrate Anatomy (Lab Final Exam) Name: Deanne Marie S. Derecho Date: October 23, 2020 Topic: Reproductive SystemDocument6 pagesComparative Vertebrate Anatomy (Lab Final Exam) Name: Deanne Marie S. Derecho Date: October 23, 2020 Topic: Reproductive SystemShaira CogollodoNo ratings yet
- Argumentative EssayDocument3 pagesArgumentative EssayMax ZinNo ratings yet
- Learning Activity Sheet 3.1: Melc 1Document7 pagesLearning Activity Sheet 3.1: Melc 1Ricah PrestonNo ratings yet
- Multiple GestationDocument24 pagesMultiple GestationNura BamaiyiNo ratings yet
- Abortion. DebateDocument5 pagesAbortion. DebateJaxeny MolinaNo ratings yet
- Thesis Summary PDFDocument29 pagesThesis Summary PDFMahima MakkarNo ratings yet
- AQA Biology GCSE Unit 4.5 Homeostasis and Response Higher Revision Activity MatDocument4 pagesAQA Biology GCSE Unit 4.5 Homeostasis and Response Higher Revision Activity MatJessica DaiNo ratings yet
- Year 8 Reproduction Test 2022 Marking ScheduleDocument6 pagesYear 8 Reproduction Test 2022 Marking ScheduleMiji LiNo ratings yet
- CloningDocument6 pagesCloningAngel L.No ratings yet
- Reproduction in Animals Notes Part-2Document5 pagesReproduction in Animals Notes Part-2kapsarcNo ratings yet
- Prenatal Care: Dr. Ruby E Robiso, Fpogs Davao Medical School Foundation, IncDocument33 pagesPrenatal Care: Dr. Ruby E Robiso, Fpogs Davao Medical School Foundation, IncISFAHAN MASULOTNo ratings yet
- MCN Mod6 Quiz LecDocument7 pagesMCN Mod6 Quiz LecKiahana PascualNo ratings yet
- The Female Reproductive System: Chapter 16: Lesson 3Document17 pagesThe Female Reproductive System: Chapter 16: Lesson 3NARDITO TUMAMPILNo ratings yet
- Calendar MethodDocument2 pagesCalendar MethodAriane AlicpalaNo ratings yet
- Prevalence of Bioethical Issues EuthanasiaDocument58 pagesPrevalence of Bioethical Issues EuthanasiaMeep MeepNo ratings yet
- Female Infertility - Causes - UpToDateDocument13 pagesFemale Infertility - Causes - UpToDateTaís CidrãoNo ratings yet
- Commercial Surrogacy Versus Altruistic Surrogacy: Analysing The Even and OddDocument14 pagesCommercial Surrogacy Versus Altruistic Surrogacy: Analysing The Even and OddSagar KamraniNo ratings yet