Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- TESCO Systems Integration BrochureDocument2 pagesTESCO Systems Integration Brochuredavev2005No ratings yet
- 2020 07 18 Transformer Bushing FailuresDocument34 pages2020 07 18 Transformer Bushing FailuresPradeep SinghNo ratings yet
- Concept of Atomic Number Leads To The Synthesis of New Element To The LaboratyDocument6 pagesConcept of Atomic Number Leads To The Synthesis of New Element To The LaboratyDIANA DORADO100% (5)
- Secretary, NSW HealthDocument30 pagesSecretary, NSW HealthRiku KusanagiNo ratings yet
- Permanent Compared With Absorbable Suture For Vaginal Mesh Fixation During Total Hysterectomy and SacrocolpopexyDocument10 pagesPermanent Compared With Absorbable Suture For Vaginal Mesh Fixation During Total Hysterectomy and SacrocolpopexyRiku KusanagiNo ratings yet
- The Surgical Suture: Miriam Byrne, MD, FRCS (Plast) and Al Aly, MD, FACSDocument6 pagesThe Surgical Suture: Miriam Byrne, MD, FRCS (Plast) and Al Aly, MD, FACSRiku KusanagiNo ratings yet
- Complete Uterine Didelphys: An Incidental Finding at Emergency Cesarean SectionDocument4 pagesComplete Uterine Didelphys: An Incidental Finding at Emergency Cesarean SectionRiku KusanagiNo ratings yet
- Solucion Ejercicios Impares Ed NagleDocument748 pagesSolucion Ejercicios Impares Ed NagleDavid García100% (1)
- Flex Appliance AdministrationDocument196 pagesFlex Appliance Administrationrolhan17No ratings yet
- On January 2Document2 pagesOn January 2Chris Tian FlorendoNo ratings yet
- Yarn Examining MachineDocument3 pagesYarn Examining MachineAbrõ Wazir100% (1)
- Textbook Engineering Economics Financial Decision Making For Engineers 5Th Edition Niall Fraser Ebook All Chapter PDFDocument33 pagesTextbook Engineering Economics Financial Decision Making For Engineers 5Th Edition Niall Fraser Ebook All Chapter PDFjennifer.bias411100% (15)
- Workflow: Accelerated Generation of CNC CodeDocument2 pagesWorkflow: Accelerated Generation of CNC CodeMarcos Paulo LimaNo ratings yet
- Blank 6 Panel Comic StripDocument2 pagesBlank 6 Panel Comic Stripapi-524714491No ratings yet
- Linde C-Matic AutobonicsDocument6 pagesLinde C-Matic AutobonicsJONHHY NGUYEN DANGNo ratings yet
- TADANO Gr300ex3Document157 pagesTADANO Gr300ex3Abi Jith100% (1)
- Class Notes - Module I - Diffraction PDFDocument20 pagesClass Notes - Module I - Diffraction PDFGajula RajithaNo ratings yet
- 01 - Fundamental ConceptDocument9 pages01 - Fundamental ConceptMehul MunshiNo ratings yet
- Van Der Waals Integration of High-Oxides and Two-Dimensional SemiconductorsDocument8 pagesVan Der Waals Integration of High-Oxides and Two-Dimensional SemiconductorsAnahí TessaNo ratings yet
- Bpe300 Um enDocument37 pagesBpe300 Um encaioalmeida492No ratings yet
- B 4 Qoq Pa PRDG 6 C XPDocument9 pagesB 4 Qoq Pa PRDG 6 C XPdhaval.desai98No ratings yet
- Roots B Centrifugal BrochureDocument24 pagesRoots B Centrifugal BrochureStephenson ViegasNo ratings yet
- Ih61h-Mhs & Ih61k-Mhs & Ih61m-Mhs - Bios - 110406Document32 pagesIh61h-Mhs & Ih61k-Mhs & Ih61m-Mhs - Bios - 110406WanAbboodNo ratings yet
- Anexo 12.4 Especificaciones Tecnicas de BombasDocument44 pagesAnexo 12.4 Especificaciones Tecnicas de BombasJhonny Miguel NuñezNo ratings yet
- Assessment - 6: Question 1: Write The C Program To Implement A Linked List File Allocation MethodDocument6 pagesAssessment - 6: Question 1: Write The C Program To Implement A Linked List File Allocation MethodVinayak MahadevanNo ratings yet
- New PSC I GirderDocument64 pagesNew PSC I Girderrahul sumanNo ratings yet
- 202 - EE8601, EE6601 Solid State Drives - NotesDocument140 pages202 - EE8601, EE6601 Solid State Drives - NotesUdayNo ratings yet
- 4 Stoichiometry PDFDocument8 pages4 Stoichiometry PDFHakim Abbas Ali PhalasiyaNo ratings yet
- Mass Balance Calculations - March 22 - FermentationDocument13 pagesMass Balance Calculations - March 22 - FermentationRj JunsayNo ratings yet
- Application of Capital Structure Theories. A Systematic ReviewDocument27 pagesApplication of Capital Structure Theories. A Systematic ReviewAhmed BakhtNo ratings yet
- Artifical Intelligence - For IT AuditorsDocument16 pagesArtifical Intelligence - For IT AuditorssumairianNo ratings yet
- CT AbdomenDocument2 pagesCT AbdomenVlog Anak DusunNo ratings yet
- CAD of Radial and Mixed Flow TurbomachineryDocument2 pagesCAD of Radial and Mixed Flow TurbomachineryjamesNo ratings yet
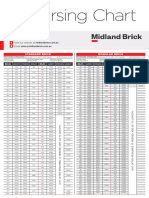
- Midland Brick Coursing ChartDocument2 pagesMidland Brick Coursing ChartMichael Slater100% (1)